@McAlister had several very informative posts about studies that showed that a dosage of 20 mg (20 ng/ml) or below would evade MTOR2 inhibition. The danger zone lies above 20 mg where if you take 40 mg you have about a 50% chance of being someone who gets MTOR2 inhibition. No one knows the chances between 21-40 and above 40. We just have 2 data points. 20 mg and below, no MTOR2 inhibition. 40 mg, 50% chance of MTOR2 inhibition.
If you want to go above 20 mg equivalent, you’re taking your chances. As Clint Eastwood would say, “Do you feel lucky, punk?”
The fee was/is to the doctor, I was not charged any other fee.
Prescriptions was sent electronically to the pharmacy I chose.
Went/go to the pharmacy picked up and paid for the item.
If you want to know the doctor that was assigned to me and that I use writing me through the message system. As most doctors do not want public attention.
I did 3 peak tests at Labcorp exactly 2 hours after taking 6 mg of sirolimus made by different manufacturers, to test 2 that were prescribed to me (Ascend and NorthstarRx) and a different one prescribed to my husband (Dr. Reddy’s). I did the tests at the same time of day and took the sirolimus the same way, with a cheese stick, some fresh berries, 1 tbs of fish oil, and green tea.
My 2-hr peak with the NorthstarRx was 28.8 ng/mL, with the Ascend was 28.7 ng/mL, and with the Dr. Reddy’s was 22.2 ng/mL. I’m not convinced the Dr. Reddy’s was less bioavailable - it could have been something else going on with my body that day or that I ate breakfast a little later than usual.
Based on what I’ve read about others’ peak serum levels, I think mine is unusually high and I don’t know why. I do NOT use grapefruit juice. I also did a trough serum test on day 7 the morning before taking another dose, and that was 0.6 ng/mL.
What a great experiment! Well designed and implemented - thanks for sharing!. I agree - the variation with the Dr. Reddy’s sirolimus seems likely to be random noise due to environmental factors, etc.
How much do you weigh? Any side effects at that dosing? Unfortunately we really don’t have enough information yet to know what an optimal blood level is (peak, AUC, or any other measure)… or know what the optimal dosing schedule (weekly or every two weeks, or low dose daily)…
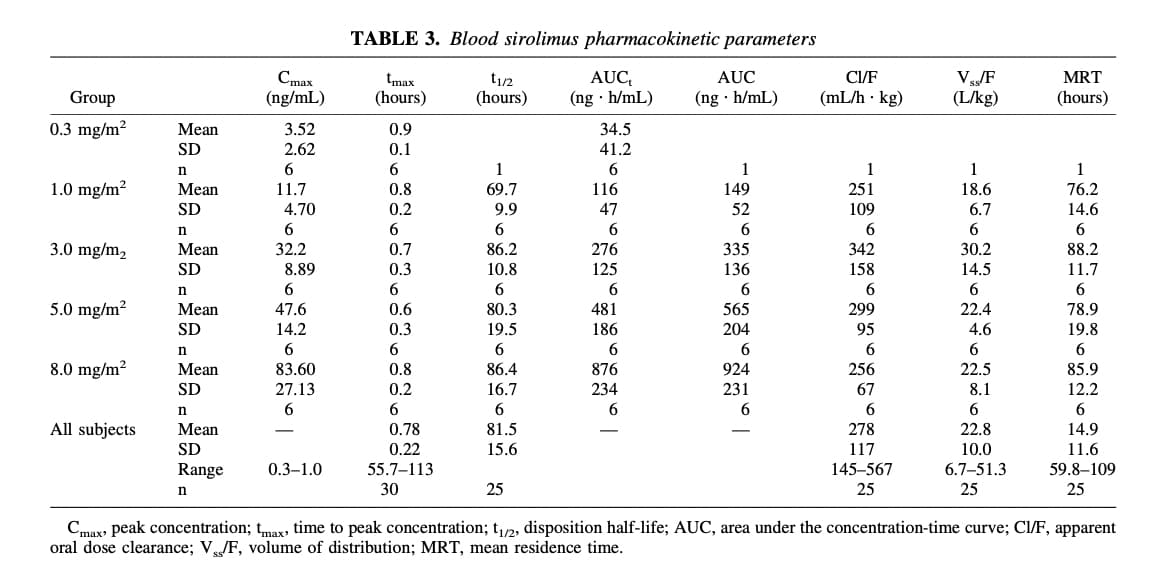
There is quite a bit of individual variation with rapamycin. If you want to understand more (or see examples in a study in healthy people) see here. You can see how large the standard deviations from the mean are for this sample, so there is obviously a significant amount of personal variation.
Sadly, I don’t think those lab results are that useful as we really want to know levels once everything has distributed into tissues as it is only at that point that you know what the effective level is. With people in the 180 lb range a single dose of 8 mg seems to have a level at 24 hrs of around 3-5. I’m sure if tested at 2 hrs it would be very high, but it needs to tissue distribute before we can really then apply the approach of using the half life to look at how long you’ll be above the therapeutic level of 3.
I’d suggest that doing a level at 18 to 24 hours post dosing and once at a dose that generates a solid therapeutic level getting a repeat 24 to 48 hours later can give an idea of what your personal half life is, then you can sort out what proportion of time you think is reasonable to be under significant mTOR inhibition and sort out your dosing interval.
This is just my approach… think it is pretty similar to Dr Green’s approach.
Anyway 2 hr levels indicate absorption, at 2 hrs and I don’t think one can make useful decisions from this.
Thanks, I’d seen that study in your “side effects” post. Those men took a liquid form of rapamycin on an empty stomach and reached their peak blood levels in under an hour. I waited 2 hours because I took it with food.
I’m 65" tall and was 155-158 lbs, and I thought I’d calculated my m2 (BSA) before, but having a hard time figuring it out now. I think it’s 1.79? If that’s right, my dose was 3.35 mg/m2 on that table, so I was in the ballpark. Still, several people in this forum who take 6 mg/wk seemed to get much lower peak serum levels.
As for side effects, when I first started a few months ago at the dose of 2-4 mg every 10 days, I developed an itchy rash on the tops of both shoulders and an itchy spot the size of a dime on my knee, which came and went. I also developed a small, inflammed bump at the edge of my upper lip on day 8 or 9, which lasted a few hours and then disappeared. Also joint pain in both shoulders and one knee in the days after taking a dose.
Since I started taking 6 mg per week just 6 weeks ago, I have no more joint pains or lip bumps. I still get the transient itchy rash on my shoulders and spot on my knee. My latest theory is that, as my sirolimus levels fluctuate, it’s causing some sort of cytokine imbalance and/or affecting my keratinocytes in such a way as to increase thymus and activation-regulated chemokine (TARC) levels and eosinophils, which are associated with sirolimus-induced rash. I did a lot of research, most of which I do not fully understand. This case report was my starting point: https://onlinelibrary.wiley.com/doi/full/10.1002/cia2.12075. From there, I found other info indicating that topical corticosteroids together with antihistimines (H1 and H2 blockers) can help. Triamcinolone did not work well for me. Antihistamines do seem to help but I’ll need to experiment more to know for sure. Hoping that my body adjusts to the rapamycin after a while and I won’t have this side effect anymore.
I think the key thing people are testing when they do the short term Cmax test is really if the medication is getting into the blood stream at reasonable levels (so they can be confident in that source/brand of rapamycin). Beyond that… yes, not a whole lot of value given the state of the science.
Absolutely, but I guess the issue is whether more is absorbed by 3 or 4 hours and redistributed. I’d suggest that a better understanding of what is going to really make up the AUC will be a level once everything is absorbed and tissue distributed.
Don’t be sad, I was just testing my absorption and any differences between the various brands. Maybe later I’ll do some testing at 2, 3 or 4 days to see what’s going on, but I’m not sure I care or what I would do differently based on the results. One change I might make is to decrease my dosage if my trough level the morning of day 7 was higher than expected, say above 1.
Bryan Johnson published his blood test results at 90 minutes and 4 days after taking 13 mg, per his “Blueprint Protocol” page. His 4-day level is below the therapeutic range at 2.5 ng/mL. I can only guess he thinks that 3 days of mTOR inhibition within the therapeutic range is enough and/or that he just wanted to verify the half-life.
I’m not sure the 2 hr level accurately addresses absorption. For example if you have version a that absorbs rapidly and let’s say you take 10 mg and 5 get absorbed in an hour but then no more vs version b that absorbs over 4 hrs but 8 mg are absorbed. The peak will be way higher on version a but the actual impact on mTOR inhibition much greater in version b. This is where a bit of a delayed test normalises this
Is there any data indicating that different versions of sirolimus which result in similar peak serum levels (after 1-2 hours) can then have signficantly varying levels of bioavailability in subsequent days, or any protocol for when the serum level does not remain at a specified level for at least X number of hours/days, in people who are doing intermittent dosing for longevity?
I haven’t heard of it, and between my husband and myself, we’re working with 3 doctors who prescribe rapamycin, including Dr. Green. None of the doctors even suggested sirolimus blood testing.
I did it on my own for three main reasons: I’m a new user of rapamycin and wanted to see my peak levels as compared to others; I wanted to know my baseline peak levels in case I make changes that might impact bioavailability in the future (such as adding back curcumin to my supplements or decreasing the sirolimus dosage and taking it with grapefruit juice, etc.); and I wanted to compare 2 India-manufactured generics (Ascend, Dr. Reddy’s) and a U.S. manufactured generic (NorthstarRx) due to articles like this one: https://wapo.st/3TmLMdf.
I may do a trough test in a few more weeks to make sure my blood levels don’t remain too high on day 6 or 7, but anything beyond that would probably not be useful.
Don’t waste your time on a trough, as it will not be useful and will be below range with standard weekly dosing.
Dr. Green reports that he tests - although I think this is when he is optimizing for people with risk of neurocognitive decline - e.g. positive ApoE4’s.
I’d suggest, having had a fair bit of education in pharmacology and pharmacokinetics, that your most useful approach is as I previously stated, look at where you are at, at 18-24 hours post dose, which will give a valid level as it will represent the drug being fully absorbed and distributed through your body, and yes, some will have been metabolized.
If you are interested in see how quickly you are metabolizing the rapamycin, you can get a repeat level in 48 hours and see how much is left, and then it is pretty straight forward to estimate your half life of the drug. Simplistically, if your level is <50% of the initial level then you will have a less than 48 hr half life, if you have >50% of the initial level then it is >48 hours. There are mathematical models to further determine this, but this is a quick approach.
Most modest single doses seem to run more in the 30’s hrs for the half life and bigger doses do seem to prolong half life - in my limited experience - I’ll get more certainty on this and better numbers over the next year as I gather more data. But that is my initial experience - but too limited to generalize.