There’s no doubt that Aspirin interferes with clotting. The question is does that benefit outweigh the risk?
Have you read the studies or just spitballing?
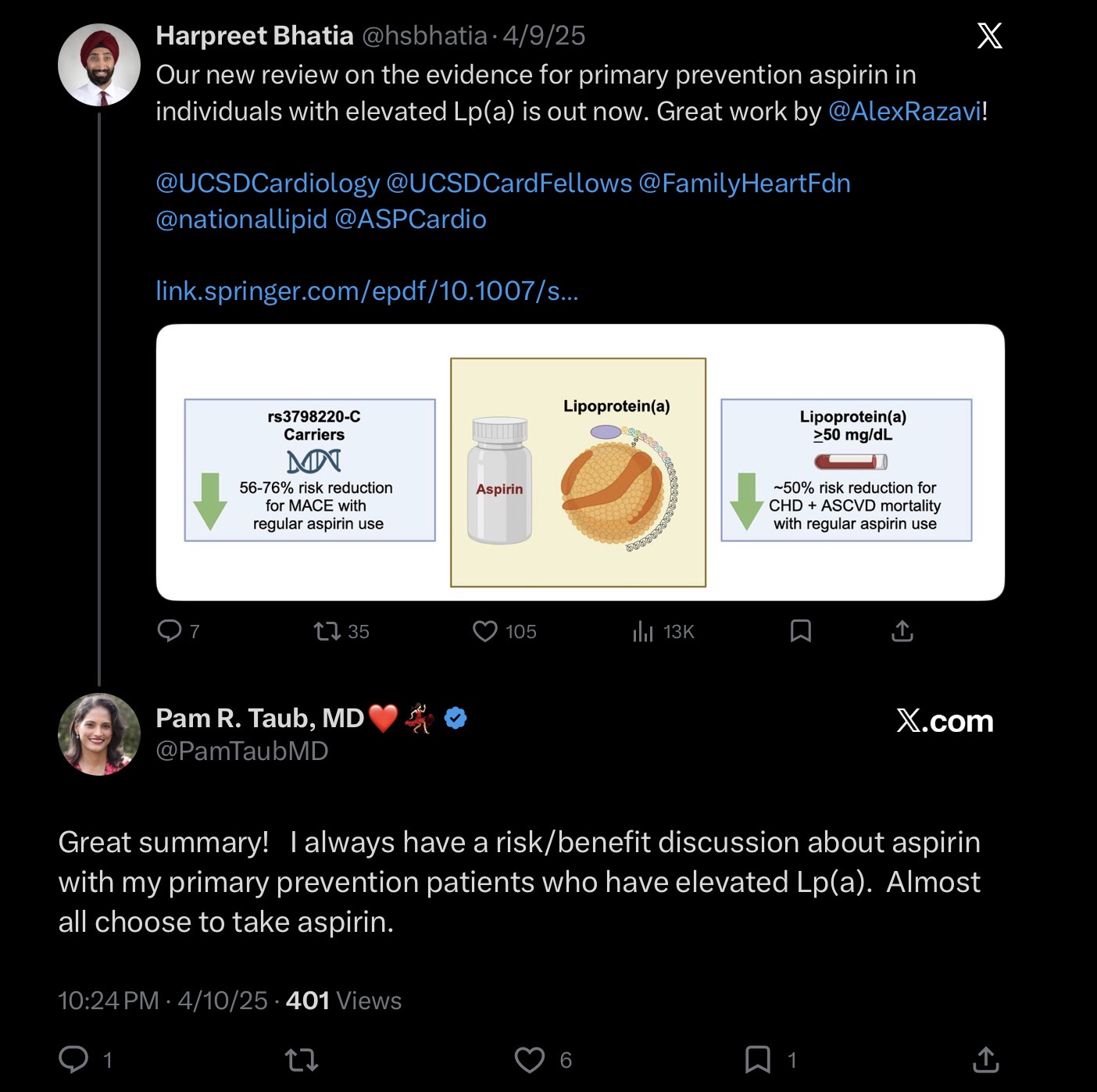
https://academic.oup.com/eurheartj/article/46/Supplement_1/ehaf784.4275/8312526
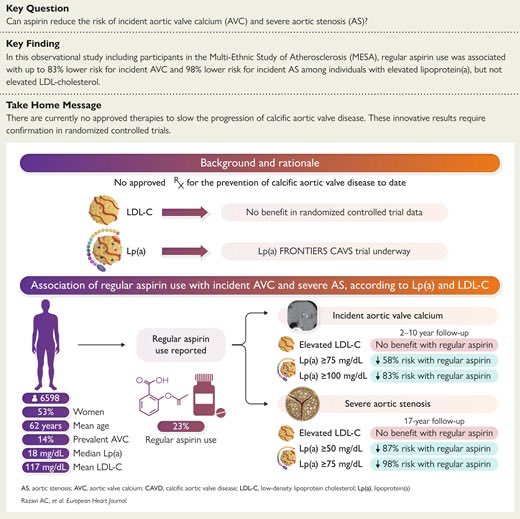
https://www.ahajournals.org/doi/10.1161/JAHA.123.033562
https://www.sciencedirect.com/science/article/pii/S2666667724000424
1 Like
All of those studies conclude that Aspirin “may” be beneficial in individuals with elevated lpa. Need a bigger study.
Exactly. Although an odd post on a Rapamycin forum. ![]() but if you have high lp(a) and you are older, you should follow your physician’s advice. If they are knowledgeable, they will likely recommend aspirin if you are not at a high risk of bleeding.
but if you have high lp(a) and you are older, you should follow your physician’s advice. If they are knowledgeable, they will likely recommend aspirin if you are not at a high risk of bleeding.
Not sure what the reference to Rapamycin means.
If you are “older” (>60), the recommendation is to not take aspirin.
1 Like
If you are older and have very high lp(a) and you are consulting a cardiologist or lipidologist that specializes in treating patients with lp(a) it is highly likely that they will recommend low-dose aspirin if you are not otherwise at a high risk of bleeding. If they don’t, and particularly if they don’t discuss it, that would be a red flag on your choice of physician. I’m not saying that a GP or an ER doctor would recommend aspirin.
The reference to rapamycin is that there are no studies with humans that would recommend off label use (possibly one with women). Certainly nothing that would come close to the studies that indicate a potential benefit from aspirin use for individuals with high lp(a).
You’ve had a Cardiologist recommend this to you?
Agree with you on the Rapamycin. There is currently no good evidence that it is beneficial to humans, especially humans that are doing other recommended health span extending activities.
Hi @KarlT … fwiw, I’ve had multiple cardiologists recommend this to me (although the first one a decade ago only suggested EOD), and my internist… and my sister and brother’s cardiologists each recommended they each take one daily. I don’t like it, but I’d feel foolish if I ignored their advice and then had an MI.
1 Like
Not low risk, but well over 60
Sister is 65 and brother is 69. Each with a very high CAC (and high cholesterol prior to statins) but not nearly what mine is.
I might have misunderstood and I thought this was about prevention vs treatment after an MI…, now I see you are questioning preventative use without any known heart disease… because elevated lp(a) alone is probably not what I’d be treating w/ baby aspirin either.
Yes, of course. I’m not sure that you would find any cardiologist that specializes in treating people with high lp(a) that wouldn’t consider it on a case by case basis. Have you read any of the studies? My guess is that you have not. If you don’t have high lp(a) then none of them would. The bleeding risk outweighs any potential benefit. People with high lp(a) have a significantly higher risk of an MI or stroke.
@zazim can you show me these studies?
My understanding is that for primary prevention of heart attacks, ASA is not recommended for anyone over 60 (USPSTF), or 70 (ACA).

Where are the patient ages discussed?
I’m going to continue to prefer medical association opinions over X posts.
The problem with waiting for medical associations to actually come out with new guidelines is that it usually takes years if not longer for those gears to move; meanwhile, patients are dying. People on a forum like RapaNews aren’t typically ones to wait for medical associations.
1 Like
Again, you’re not a cardiologist and so there’s no harm in your following the guidelines. But people that actually deal with people with high lp(a) don’t wait for guidelines to change. Europe and Canada recommended testing for lp(a) a decade ago. We changed only our recommendation this year. The guidelines don’t recommend testing for ApoB even though it is clear evidence that risk follows ApoB and not LDL-C when they diverge. I know a doctor from MD Andersen who has similar levels to mine. He’s in his 40s and he takes daily aspirin. You clearly didn’t read any of the studies I linked.
1 Like
I would tend to agree that cardiologists don’t wait for guidelines. Primary care uses guidelines.
10 years ago, every cardiologist I talked to recommended apoB and calcium scores for further risk stratification like the guidelines state that came out last week. They also recommended statins earlier than guidelines and dismissed the 10yr AVSCD risk model that primary care uses.
Guidelines have a role. They are extremely delayed and conservative. I would argue that represent the bare minimum and they reflect cost issues with treating populations.
The “do no harm” is very powerful and you need to convince a lot of MDs to change guidelines. It was always a nice feeling to finally have guidelines state what you have been practicing for years.
I know the data about aspirin and GI bleeds and personally don’t take it (my lpa is 16) I also have never seen a significant GI bleed on 81 mg. I’ve taken care of a significant number of NSAID related bleeding but 81 mg of aspirin is just such a tiny dose.
Aortic valve issues get to be pretty significant as you get 80. I also had a colon polyp. So I won’t be surprised if I decide to start taking asa. Might be nice to have a baseline echo - I am 55.
3 Likes
Could you share more about the aortic valve issues and what you mean by that?
You have yet to show a study recommending aspirin for elderly patients
I don’t doubt that is your experience, but in my little world this is what I know….
My brother and sister see cardiologists on the east coast. They’ve each been on statins for over a decade and we have an awful family history. It was only this year that they finally had a CAC, tested for lp(a) and ApoB, and started ezetimibe. It was all them asking about it, not one of their cardiologists brought any of those options up on their own.
Of course I have no idea how good their cardiologist are, but until recently, I was at UCSF for over a decade, and including my first cardiologist there who is considered to be a very big deal, not one of them ever mentioned ApoB to me (nor ezetimibe or bempodioc acid, and I asked about colchine and was told ‘great idea’ ).
To his credit, I was put on repatha and he did test my lp(a) before I knew what that was. It’s not that they had not heard of ApoB but I wonder why they never tested mine. Was it they figure we know you are high risk so more info is not useful? Regardless, I realized I was wasting my money because my care was not worth their fees, so I don’t go there anymore.
Also, regarding guidelines…
My first cardiologist at UCSF (I had been seeing cardiologists for the 10 years prior to that and the advice I was getting from them was fairly useless) was the only one ‘bold’ enough to mention baby aspirin to me. He said the guidelines are you shouldn’t take it, but if you were my sister, I would tell you to take it EOD. He eventually kicked me out of his practice because he mostly does research and only kept his more interesting cases… or much more connected people:)
No one mentioned baby aspirin to my brother and sister, so last year, when I asked them what their docs advise (because I was always wondering if I should be taking my EOD dose at all), they each brought it up to their docs, and only at that point did their cardiologists advise to take it daily. I then approached my new UCSF doc about it and he said, yes, definitely take it daily… I also ran it by my internist and he agreed.
My point of bringing up UCSF is only to share that you can go to one of the more respected places and still not get the most cutting edge advice.
2 Likes