I’d hold off on using Dasatinib Dasatinib and Quercetin as Senolytic May Cause Brain Damage
4 Likes
roger that.
but its odd that the other studies didn’t mention any weird side effect on the mice.
So paused again on senolytics ![]() Do we return to FOXO4-DRI?
Do we return to FOXO4-DRI?
This peptide while promising also doesn’t have a lot of human data. I myself have also been tempted to try it but honestly it might be harmful.
For senolytics I use quercetin and fisetin. I don’t do it consistently. Once every few months. Piperlongumine is another natural compound that shows promising senolytic effects.
I use more senomorphics than senolytics.
Senolytics are compounds that selectively induce death of senescent cells, reducing their overall burden in tissues. Senomorphics do not remove senescent cells but instead modify their behavior, primarily by suppressing inflammatory and tissue-damaging signaling (the SASP) and improving cellular stress resilience, which can indirectly reduce the rate at which new senescent cells form.
Rapamycin is a great example of a senomorphic:
“Rapamycin extends life span and health span in several laboratory animal models and has multiple cellular effects. It inhibits cellular senescence in a broad range of cells, but its mechanism is not fully established. Hepatocytes from mice treated with rapamycin for 6 months had increased levels of Nrf2, a protein regulating protection against oxidative damage triggered by injury and inflammation (43). Nrf2’s role in mediating rapamycin’s effects on cell senescence was clarified in rodent Nrf2 knockout studies: rapamycin-induced decreases in senescence markers p16 and p21 required Nrf2, but that rapamycin’s diminution of beta-galactosidase and SASP did not (44).”
National Institute on Aging Workshop: Repurposing Drugs or Dietary Supplements for Their Senolytic or Senomorphic Effects: Considerations for Clinical Trials - PMC
Additionally rapamycin activates mitophagy allowing the body to remove and recycle old and damaged mitochondria which can be part of an overall mitochondrial optimization strategy:
“Overall, our findings suggest that rapamycin ameliorates cognitive impairment in 5 ×FAD mice via mitophagy activation and its downstream PINK1-Parkin pathway, which aids in the clearance of amyloid-β (Aβ) and damaged mitochondria. This study reveals a novel mechanism involving mitophagy regulation underlying the therapeutic effect of rapamycin in AD.”
Mitophagy activation by rapamycin enhances mitochondrial function and cognition in 5×FAD mice - PubMed
Metformin is also senomorphic, downregulating SASP cytokines:
“Metformin Downregulates SASP and Lowers Senescent Cell Burden. Metformin, although not exhibiting senolytic properties, has been effective in suppressing cellular senescence and SASP in multiple age-associated dysfunctions. Chronic metformin administration at low doses delays senescence in human diploid fibroblasts and human mesenchymal stem cells, as evidenced by reduced SA-β-gal staining, via Nrf2-mediated upregulation of glutathione peroxidase 7 (GPx7) (Fang et al., 2018). Metformin’s serotherapeutic role is also mediated by its anti-inflammatory effect by preventing NF-κB translocation into the nucleus thereby not phosphorylating IκB and its kinase and inhibiting NF-κB pathway altogether (Moiseeva et al., 2013). Inhibition of NF-κB by metformin in ex vivo cultures of murine olfactory ensheathing cells is also associated with decreased SA-β-gal activity along with a decreased expression of pro-inflammatory cytokines and oxidative stress markers (Śmieszek et al., 2017). In a DICER1-dependent mechanism, metformin is shown to lower the protein levels of p16 and p21 and RNA levels of SASP hallmarks including IL-6 and IL-8 in human fibroblasts (Noren Hooten et al., 2016). Recently, in human periodontal ligament cells, the protective effect against senescence and oxidative stress was linked to metformin-induced stimulation of autophagy, further highlighting the role of metformin in targeting the interconnectedness of these two hallmarks of aging (Kuang et al., 2020). Similarly, in in vitro and in vivo models of intervertebral disk degeneration, metformin treatment reduced senescence in nucleus pulposus cells by upregulating AMPK-mediated autophagy (Chen et al., 2016).
It is evident that metformin attenuates the increased burden of senescent cells and upregulation of SASP with aging. Its role as a SASP modulator via Nrf2-Gpx7 activation in mediating oxidative stress and via NF-κB inhibition in mediating inflammatory response provides a better understanding of its senotherapeutic mechanism. However, in the context of breast cancer and hepatoma, low-dose metformin has been previously shown to induce SASP gene expression signature and p53-dependent senescence, respectively (Williams et al., 2013, Yi et al., 2013). Thus, metformin’s effect on cellular senescence and SASP is context dependent (anti-cancer by inducing apoptosis and anti-aging by inhibiting inflammation), probing for further understanding of what stimulates metformin to induce an anti-senescence response in aging tissues as opposed to pro-senescence in cancerous tissues. With the advent of clinical trials with senolytics, it is also crucial to understand how metformin can be best utilized in combination with other drugs to optimize the combinatorial effect on senescence and aging.”
https://www.sciencedirect.com/science/article/pii/S1550413120301832
Urolithin A shows promising signs of senomorphic activity:
“Our findings reveal that urolithin A is non-cytotoxic to senescent AD-hMSCs and significantly suppresses the SASP by reducing the secretion of key pro-inflammatory mediators, including MCP1, PAI2, and IL1B. In addition, it was demonstrated that urolithin A was capable of reversing the decline in H3K9me3 levels induced by Doxorubicin treatment, restoring them to levels observed in untreated cells. The results of this study suggest that urolithin A functions as a senomorphic agent, capable of modulating cellular senescence.”
Urolithin A Alleviates Doxorubicin-Induced Senescence in Mesenchymal Stem Cells - PMC
Aspirin possibly has senomorphic activity (caution using aspirin/NSAIDs if you have asthma):
“Aspirin shows senomorphic activity by counteracting the loss of NO production in senescent endothelial cells75 and improves ageing-related vascular relaxation in mice.76 Aspirin has also senolytic effects in a study exploring long-term extra-cardiac adverse effects of doxorubicin.77 Another study, however, reported an opposite, senescence-inducing effect of aspirin on cancer cells.78”
https://academic.oup.com/cardiovascres/article/121/5/730/8046207
Statins show interesting effects on senescence:
“Statins are a staple of lipid-lowering therapy and CV event prevention.79 These drugs show a complex relationship with senescence. Atorvastatin prevents the onset of senescence in endothelial progenitors,80 while simvastatin acts as a senomorphic and antagonizes the pro-inflammatory SASP in senescent fibroblasts in breast cancer.81 These effects may stem from the SASP-activating mevalonate pathway82 or restricting cholesterol lysosomal partitioning that supports the SASP.83 Simvastatin, atorvastatin, and lovastatin, but not pravastatin, are senolytic and trigger senescent cell death at high doses.84 It thus may be speculated that the formation of presumably senescent foam cells85 in atherosclerotic plaques gets prevented by intensive statin therapy. On the other hand, statins sensitize cells to senescence after radiation.86 Due to the complex roles of lipids in senescence, statins may have situationally specific effects in senescent cells.”
https://academic.oup.com/cardiovascres/article/121/5/730/8046207
SGLT2 inhibitors (things like empagliflozin, dapagliflozin, etc.) show promising effects on senescence:
Quercetin in addition to being senolytic is also senomorphic due to it reducing downstream SASP cytokines.
Other natural senomorphic compounds to look into include: curcumin, EGCG, luteolin, apigenin and spermadine
What is your overall longevity protocol if you don’t mind me asking?
I’m not of the opinion that currently available senolytics/senomorphics have a good ROI on longevity unless you’re using things like rapamycin, metformin, SGTL2 inhibitors, etc. and are taking advantage of the off target potential senolytic/senomorphic effects. There are higher ROI things we can be doing for our health right now than singling out specific senolytics in my opinion.
5 Likes
You also forgot taurine. In mouse studies, mice taking taurine had fewer senescent cells than those taking D+Q. It’s better to prevent formation than to remove senescent cells.
5 Likes
Good to know! I’ve been reading a lot about taurine lately for the benefits for sleep, and it has a number of other really promising effects. I’m planning on upping my dose from 1-2g a day to probably closer to 6-10g:
Tau is reported to improve the antioxidant defence networks in different ways.
First, in some tissues (e.g., heart and eye), Tau can directly scavenge free radicals.
Secondly, Tau participates in maintaining the integrity of electron-transport chain of mitochondria, the main sources of ROS in biological systems.
Thirdly, Tau is shown to inhibit the activities of ROS-producing enzymes, including XO and NADP oxidase.
Fourthly, by interacting with transcription factors (e.g., Nrf2 and NF-κB) and inducing AO enzymes, Tau can maintain the optimal redox status of the cell.
Finally, by activating vitagenes, including SOD, HSP, thioredoxin, sirtuins, etc., Tau can provide additional protection in stress conditions and help in the creation of an effective adaptative response to stresses.
From the literature data analysed above, it could be concluded that:
Tau plays a vital role in the AO defence network. However, the direct antioxidant effects of Tau in biological systems are limited.
The stabilizing effects of Tau on mitochondria under various stress conditions, including commercial animal and poultry production, deserve more attention.
A range of toxicological models clearly showed the protective antioxidant-related effects of Tau.
Until now, major Tau applications have been related to human health, including the prevention/treatment of various diseases or decreasing the detrimental effects of various essential drugs used in human medicine.
Furthermore, there are a range of publications confirming the protective effects of Tau (alone or in combination with other antioxidants) in various stress conditions of commercial meat and egg production.
Anti-inflammatory and immunomodulatory properties of Tau are of great importance for veterinary medicine.
Indirect antioxidant activities of Tau due to the modulation of transcription factors and vitagenes leading to the upregulation of the antioxidant defence network are likely to be major molecular mechanisms of Tau’s antioxidant and anti-inflammatory activities, and they deserve more attention and further investigations.
https://www.mdpi.com/2076-3921/10/12/1876
1 Like
IASO AEGIS PROTOCOL
v17.4
Status: Phase 5 (Stabilization) — ACTIVE (Post-Senolytic Scout / Integrating 5-LOX Ramp)
Objective: Aortic Shielding, 5-LOX Inhibition, & Phenotype Preparation
Compiled 22 May 2026 · Personal reference copy
I. THE STACKS
MORNING (10:00 AM) — Peptides (Sub-Q)
GHK-Cu + KPV (Custom/Research): 2.0 mg / 250 mcg — Schedule: Mon–Fri (5/2)
Retatrutide (Custom/Research): 2.0 mg — Schedule: Mon / Thu
MORNING (10:00 AM) — Daily Oral Support (With Breakfast / Fats)
Olmesartan (Prescription): 10 mg (Split)
5-Loxin AKBA (Vitacost-Synergy): 150 mg (1 Cap) — (NEW: Week 1 GI Tolerance Ramp)
Note: Taken directly with breakfast. After Day 7 this cap remains here as the AM half of the permanent maintenance split.
Pycnogenol (Swanson): 100 mg — Current anchor; running until supply is exhausted.
BioCoenzymated Active B Complex (Natural Factors): 1 Cap
Taurine (Organika): 1,000 mg
Vitamin C (Jamieson): 250 mg
Magnesium Bis-Glycinate (CanPrev): 200 mg
MORNING (10:00 AM) — 5/2 Phenolic Stagger (Mon–Fri)
Citrus Bergamot (Swanson): 600 mg
Berberine (PlantVital): 500 mg
Bamboo Silica (Swanson): 300 mg
Curcumin Meriva (Webber Naturals): 500 mg — Strictly locked at 1×/day.
Quercetin Pulse (Nutrawave): 1,200 mg — Schedule: Tue / Wed / Thu ONLY (take min. 3 h after GHK-Cu).
MIDDAY (2:00 PM) — Mitochondrial / Repair (Daily)
NMNH Complex (California Gold): 1 Cap (NMNH 250 mg, PQQ 20 mg, CoQ10 100 mg, Ergo 5 mg) — current active complex.
TMG (Just Glow): 500 mg
NAC (Natural Factors): 600 mg — Schedule: Mon / Wed / Fri base.
Manganese Chelate (Natural Factors): ~1.25 mg (split 2.5 mg tab).
Zinc Picolinate 3-in-1 (Herba): 1 Cap (Zn 25 mg / Cu 2 mg / Se 200 mcg).
Vitamin D3 + K2 (Nutritionn): 5k IU / 240 mcg (2 Caps).
TUDCA (Generic): 500 mg — Optimized safety baseline dose.
Dill-Berry Extract (Custom): 500 mL (European seeds only).
EVENING MEAL (With Dinner / Fats) — 5-LOX Maintenance Window
5-Loxin AKBA (Vitacost-Synergy): 150 mg (1 Cap) — (ON HOLD FOR WEEK 1)
Note: Starts on Day 8. Placing this cap at dinner keeps it inside a robust fat window for 24-hour steady-state coverage.
BEDTIME (10:00 PM) — The Shield Engine (Daily)
Olmesartan (Prescription): 10 mg (Split)
Honokiol (Econugenics, HonoPure): 250 mg — Schedule: 5 days ON / 2 days OFF.
MT-1 (Custom/Research): PAUSED (holding post-Fisetin Scout evaluation).
EGCG (EBYSU): 500 mg — Schedule: Mon–Fri EVENING (5/2).
Citrus Bergamot (Swanson): 600 mg — Schedule: Mon–Fri PM.
Berberine (PlantVital): 500 mg — Schedule: Mon–Fri PM.
Amino Stack (Custom Mix): 11.5 g total (Glycine 5 g, Proline 3 g, Valine 2 g, Lysine 1.5 g).
CoQ10 (Ubiquinol): 100 mg
Taurine (Organika): 1,000 mg
Vitamin C (Jamieson): 250 mg
Magnesium Bis-Glycinate (CanPrev): 200 mg
II. INTEGRATED PHASES & GATES
Phase 1: Foundation (Aortic Shield): (ACTIVE) Olmesartan (10 mg BID) and Honokiol running permanently.
Phase 2: Cellular Reset: (COMPLETE) Epitalon (10 days). Repeats every 6 months.
Phase 3: Mitochondrial Sprint: (COMPLETE) SS-31 for ETC stabilization (6–8 weeks).
Phase 4: Mitochondrial Biogenesis: (COMPLETE) MOTS-c extended course (4–6 weeks).
Phase 5: Stabilization: (ACTIVE) Current state. Static post-scout mapping and 5-LOX titration.
Phase 6: Senolytic Clearance (Response-Driven):
Fisetin Scout: 3-day clean pulse (1,500 mg) — COMPLETE.
D+Q (Dasatinib / Quercetin): frequency is response-driven, based on baseline recovery.
Recovery Gate: 21–35 days post-pulse. BP / RHR / sleep / spine pain must return to baseline for 5 consecutive days.
Phase 7: Regen (The ATRA Pulse): exploratory transcriptional probe.
Schedule: 14 days ON / 14 days OFF (3 cycles / 12 weeks total).
Dose Escalation: 10 mg → 15 mg → 20 mg based on tolerance / imaging.
Rule: suspend Berberine / Bergamot. Vitamin C reduced to 250 mg total daily. Honokiol CONTINUES.
5-LOX Rule: drop the PM Boswellia completely — run only 150 mg (1 Cap) total daily in the AM. Halving the dose trims CYP3A4 competitive inhibition while keeping baseline 5-LOX coverage during active ATRA exposure.
Phase 8: Quiet Window: (6 weeks) preceding the September Scan. Zero active peptide / phenolic signaling. Olmesartan NEVER paused.
III. APPENDIX: OPERATIONAL RULES & PAUSE MAPS
1. Permanent Timing & Mapping Rules
Copper Separation: Tue / Wed / Thu Quercetin pulses must be taken a minimum of 3 hours after the morning GHK-Cu injection.
Mapping Principle: log BP, RHR, spine pain (0–10) and water intake 3× daily (Waking, Midday, Pre-PM Olmesartan).
Actionable limits: standing SBP repeatedly < 95 mmHg requires immediate fluid / electrolyte / food recruitment before altering any medication parameters.
2. The v17.4 Extended Pause Map (For Future Senolytic Cycles)
Definitely Pause: MT-1, GHK-Cu, KPV, Dill-Berry, Amino Stack, Epitalon, ATRA, Berberine, 5-Loxin AKBA (all caps), EGCG, extra Quercetin, Retatrutide.
Cautious-Pause (1st Cycle Only): Citrus Bergamot, Curcumin Meriva.
Continue: Olmesartan, Honokiol, NAC (shift to daily), TUDCA (1,000 mg high-protection dose), D3 / K2, B-Complex, TMG, Magnesium, Taurine, Vitamin C (500 mg).
3. 5-Loxin Structural Interactions
Olmesartan Integration: zero interference. Olmesartan is cleared via esterase hydrolysis, so Boswellia’s mild CYP3A4 activity has no kinetic cross-talk with the primary vascular anchor.
ATRA Interaction Management: ATRA relies heavily on CYP3A4 for clearance. A full 300 mg maintenance dose of Boswellia could cause slight ATRA accumulation. During active Phase 7 ON-weeks the evening-meal Boswellia capsule is suspended entirely to protect this clearance pathway.
4. Potential Add-Ins & Watchlist Compounds
Melatonin (1 mg bedtime): pending. Targets ADAM17 inhibition to prevent protective ACE2 shedding. Hold until baseline mapping stabilizes.
Genistein (40–60 mg bedtime): pending supply. ERβ agonism driving upstream SIRT1 / ACE2 and eNOS upregulation.
Citrus Peel Extract / PMFs (Polymethoxylated Flavones): tracked for lipid-lowering and anti-inflammatory synergy alongside Bergamot / Berberine.
C21 / Buloxibutid: oral AT2R agonist. Tracked as a high-affinity pharmacological option for aortic dilation protection.
Urolithin A: tracked for targeted mitophagy via PINK1 / Parkin pathways.
Icariside II (ICS-II): tracked for mechanosensory VSMC phenotype locking, pending a highly bioavailable phospholipid complex option.
IV. PENDING TRANSITIONS & HOLD LIST (Future Implementation)
Sustained-Release Nicotinic Acid (Metagenics Niatain): 500 mg — future NAD+ / lipid anchor; on hold until current NMNH complex supply runs out.
Grape Seed Extract Extra Strength (Natural Factors): 400 mg — future vascular-support replacement for Pycnogenol; on hold until current Pycnogenol supply is exhausted.
CoQ10 (Ubiquinol): 100 mg — future standalone midday addition; on hold until NMNH unbundling occurs.
PQQ: 20 mg — future standalone midday addition; on hold until NMNH unbundling occurs.
Ergothioneine: 5 mg — future standalone midday addition; on hold until NMNH unbundling occurs.
1 Like
I skipped my quercetin this week.
I was going to hit D&Q mid June.
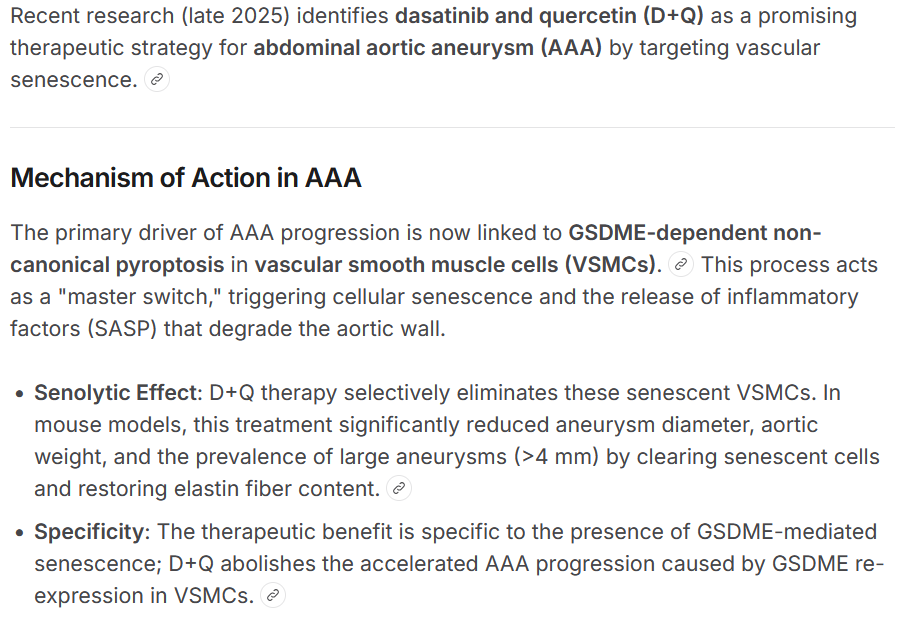
My aortic root is dilated and I’m trying what I can to shrink it.
I was going to incorporate ATRA but alas another finding suggesting cardiac hypertrophy, which is really too bad. I’m still on the fence about it.
The way my dilation is, I think this is inflammation based, too many injuries, and my spine is affected. But one never really knows.
The dosing schedule is different in this study than the hit-and-run pulse used in humans.
Also, I’d like to add this:
1 Like
Impressive protocol. I just wanted to caution on dasatinib. It’s up to you if you want to use it.
From what I’ve read there isn’t anything that can shrink a dilated aortic root (other than surgery), but your blood pressure medicine should help prevent it getting worse. What is your blood pressure at the moment?
~90/60. My BP has never been very high, but the olmesartan is a powerful AT1R inverse agonist, much better than losartan. It also inhibits mechanical stretch signalling.
I’ve found some evidence for regression of the aorta. I wish I could speak with some old researchers who reversed some elderly people’s aortas.
I thank you for the cautionary note; it is a reminder that I’m still very ignorant regarding outcomes. I suppose we all are.
2 Likes
Have you tried any senolytics? I did fisetin this month, about a week ago, and have used quercetin for years, but not D&Q nor FOXO4-dri.
I still think they were doping those mice a bit too much, but I will heed your warning and research more; same with ATRA.
After looking into this, I think this is a small concern. You can see my response on the thread you linked. People use dasatinib chronically for a long time and they are fine. There is an association with demyelination, but it appears to be reversible.
Dasatinib-associated reversible demyelinating peripheral polyneuropathy in a case of chronic myeloid leukemia
she used it for 7 months before her symptoms (?) I’m not sure maybe 2 weeks, either way though, not after a two-day regime.
High dose fisetin and quercetin.
1 Like
One more reason to figure out senescent cell management.
I take the mercenary approach, kill them.
I’m not interested in rehabilitation (with seno-morphics) of already damaged cells, just eliminate them and their harmful SASP and let the body rejuvenate and make new cells.
Of course it is impossible to kill all senescent cells so don’t worry about that. This argument is often used to “be careful you don’t kill them all” when that is an impossibility.
Finding the balance of senescent cell count is nigh on impossible without a good commercially available test that can help identify our SASP burden.
Also the fact that senescent cells are continuously created tells us we will always have them. Especially as we age and our weakening immune system can’t keep up to the senescent cell load.
Senescent cells dodge cell death by rewiring fat metabolism, study shows
by German Cancer Research Center
https://medicalxpress.com/news/2026-06-senescent-cells-dodge-cell-death.html
1 Like
I think it is relatively clear that senescent cells end up where there is a lot of cell division. There is an argument that they are the cells created from stem cells that have not managed to fully differentiate.
senescent cells: argument that they are the cells created from stem cells that have not managed to fully differentiate
The provided search context does not support the argument that senescent cells are defined as stem cells that have failed to fully differentiate. In fact, the context explicitly defines cellular senescence as a state of stable cell cycle arrest in proliferating cells, distinct from the state of stem cells or terminally differentiated cells.
Key distinctions from the context include:
- Distinct Cell States: Senescent cells are described as distinct from both quiescent cells (which can re-enter the cell cycle) and terminally differentiated cells (which have ceased division permanently as part of normal maturation).
- Trigger Mechanisms: Senescence is typically triggered by DNA damage, telomere shortening (replicative senescence), or oncogenic signaling, rather than a failure of differentiation. It serves as an anti-tumor mechanism to prevent the replication of damaged cells.
- Stem Cell Relationship: While stem cells can undergo replicative senescence after limited divisions (the Hayflick limit), and aging stem cells may lose regenerative capacity, senescent cells are not characterized as “incomplete” or “failed” differentiated cells. Instead, they are viable, metabolically active cells that have adopted a pro-inflammatory Senescence-Associated Secretory Phenotype (SASP).
- Reversibility and Plasticity: Recent findings suggest senescence is not necessarily irreversible; cells can exit senescence and regain proliferative capacity, sometimes exhibiting stem-like properties or phenotypic plasticity, but this is a response to stress or specific molecular interventions (like miR-302b), not a default state of failed differentiation.
In summary, the context portrays senescent cells as arrested, non-dividing cells resulting from stress or damage, rather than undifferentiated or partially differentiated stem cell derivatives.
Senescent cell are generated in a variety of ways, not one way.
How they are created is irrelevant to clearing out the excess ones that are a root cause of inflammation.
senescent cells, how are they created.pdf (338.5 KB)
1 Like
How long have you been doing senolytics? I was still planning on doing my first D&Q treatment in a couple weeks. Any guidance is much appreciated. Have you ever tried navitoclax?
edit: sometimes i find Brave’s AI, Leo, to be more concise then other AI engines. That’s what I used in my earlier response. I haven’t really messed with perplexity much.
I started my senolytic journey in 2018 and developed a dietary formula in 2019
I developed a dietary supplement based on some ideas related to the Mayo Clinic trials with D+Q and Fisetin. I learned that the dose of Q and F they used was significantly higher than what people think it is and I learned about the low bioavailability of polyphenol flavonoids and how that was addressed. The problem is the volume required for those compounds to be effective is very high if you do not use Dasatinib. Which I could not use in a dietary supplement.
I’ve posted the formula and use protocol several times on this forum and there is a link in my bio to a thread I started with this information.
I was looking for a “test” and settled on epigenetic DNA testing. Started with one company (Liz Parrish’s company) that stopped offering the test and switched to www.trudiagnostic.com Ryan, Hanna and their group are on the bleeding edge of this tech.
I have also posted a little evaluation we did with a few people who participated in a 7 month eval. Every one experienced a decline in bio age. Whether those tests are valid can be debated and I don’t disagree with their limitations, but they do show trends.
My wife and I did 4 cycles a year for 4 years. We saw continuous improvements in our various epigenetic markers over those 4 years.
2 years ago we switched to FOX04-DRI twice a year.
My current CRP is 0.2
At the age of 70 most of my predecessors, father, mother, grandfathers on both sides, my grandmothers were all bent over with arthritis. I’m not. I do have it and continue to fight that but I only have a bit in my left hand, predominantly my little finger LoL!
So I’m very happy about that.
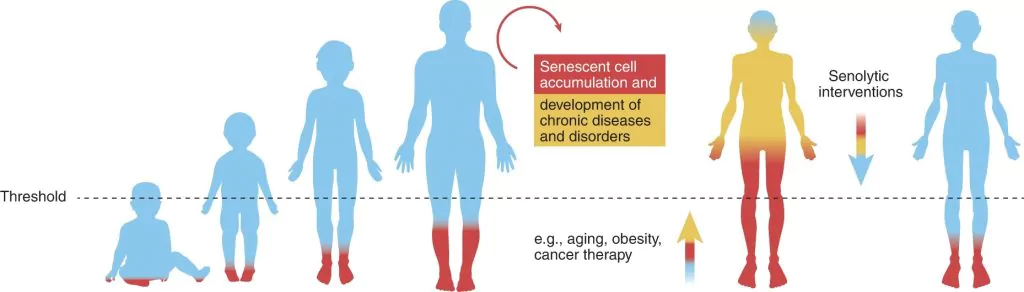
I subscribe to the Threshold Theory of Senescence
5 Likes
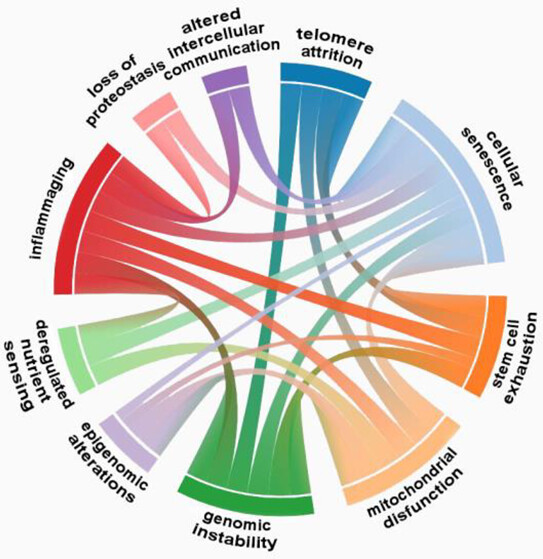
If the 12 Hallmarks of Aging have meaning, then one aspect is to evaluate how they interact with each other. Which Hallmarks have the highest level of interactions? If that matters, then addressing the Hallmarks in order of interaction may be a interesting idea.
- Senescence - 8 interactions
- Inflammaging - 7 interactions
- mitochondrial disfunction - 6 interactions
- genomic instability - 6 interactions
- stem cell exhaustion - 5 interactions
on down the line
This is just an idea as some of the Hallmarks that have fewer interactions may have greater harm/benefit if addressed.
2 Likes
@RapAdmin Sorry, late to this party. Not sure how I missed it ![]()
Testing requires phlebotomy collection, then shipped back in a special cooler we provide. No dry ice, postage to and from included in the price.
And yes, @DrFraser has access. I also did a podcast a week or so ago that goes over what we test and why. Dr Fraser will post the link in the near future
1 Like