Hedging my bets by taking rapamycin, which is already senomorphic. But otherwise, I’ve become more and more skeptical of the current crop of senolytics, especially after listening to the Attia roundtable.
3 Likes
Mice die primarily from cancer - 85-95%. Humans die primarily from heart disease.
I think you have to ponder the question “How much do senescent cells impact cancer?” If the answer is “A lot” then senolytics (as shown by the ITP) probably are not very useful. If the answer is “Not much” but very useful for cardiovascular health or maintaining healthspan in old age, then senolytics may be very useful to humans who do not die primarily from cancer.
6 Likes
Yours too. Thanks for the civil discussion. And absolutely, I support guys like Kirkland pursuing things, and hopefully we can have bigger, better, longer studies to really answer these things.
Honestly, a lot of this could be answered if we had a better method to measure whether the treatment is actually working. For example, I see your protocol mentioned earlier. If there was something you could track or measure that would be super exciting, even in the absence of lifespan data.
2 Likes
There is supposed to be a new test that is only available to health care practitioners.
As you noted, we did use a DNAm test from Trudignositc in an attempt to validate our little eval. Plus it is an easy to do at home test. My hope was those markers might be a proxy for overall SASP reduction, but I can’t prove that. Of the 4 that completed the program (not counting myself and my wife, we both improved over a 4 year span) all showed an improvement. What does that mean/indicate? who knows for sure…
Once I saw it “work” for strangers with no skin in the game, that was enough to give me a bit of hope ![]() regardless of what was actually happening LoL! I’d really love to know;
regardless of what was actually happening LoL! I’d really love to know;
- is it actually clearing senescent cells
- are the improvements due to this clearance
There are so many mouse studies on this that indicate a benefit but those are mice and I don’t always trust rodents ![]() although they do “naturally” experience cellular senescence as opposed to the need to be genetically manipulated as is the case with AD research.
although they do “naturally” experience cellular senescence as opposed to the need to be genetically manipulated as is the case with AD research.
And then if a level of healthy senescence can be determined, and then maintained/iterated with judicious use of senolytics and testing to evaluate levels, my guess is probably not easily maintained as we age, due to the varied types and locations of SNC’s
The D+Q combo with our addition of Fisetin is limited in “reach”. That combo only appears to reduce senescent cells in adipose and endothelial tissues. One of those limitations.
Which is why we started doing cycles of FOX04-DRI in Dec.
5 Likes
Something that has system wide effects on a wide variety of cells and process is probably not inconsequential. Regardless of what lifespan results in mice says…
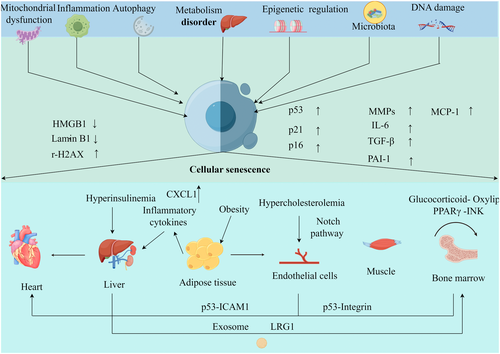
Targeting senescence or delaying aging is emerging as a critical health strategy for solving age-related diseases, especially in the old population. In the current review, we will delineate the mechanisms of organ crosstalk in systemic aging and age-related diseases to provide therapeutic targets for delaying aging.
https://faseb.onlinelibrary.wiley.com/doi/abs/10.1096/fj.202402479RRR
2 Likes
Based on the following paper, an SGLT2I should be a part of senolytic therapies.
5 Likes
I’m using FOX04-DRI, highly diluted because it has a sting. Taking it with MOTS-c, as advised by Alek Kikel.
I pulled a muscle today, but I expect peptide therapy to minimize the damage. I’ve recently added epitalon spray, which does promote extended sleep, to my repertoire.
1 Like
I didn’t find that for me, and a friend who added Epitalon found the opposite effect.
I think the majority of people using this one do find the sleep benefit.
What dose are you using for Epit?
And what dose and schedule are you using for FOX04-DRI if you don’t mind me asking ![]() I’m going to up my dose for our next cycle April 1.
I’m going to up my dose for our next cycle April 1.
April is when we will also do our next Trudiagnostic test. Too many people getting ahead of us on the Rejuvenation Olympics leader board LoL! Over 5700 participants there. Joan is just barely in top 10 and at 50 and I’m out of the top 200 at 206. Still pretty good out of 5700 ![]() I think I may hook up with a Longevity Doc
I think I may hook up with a Longevity Doc ![]()
2 Likes
The spray provides 10 iu per nostril, which is in the microgram range. Whether it increases telomerse length or not, it is said to retard the aging process. Maybe we’re all regressing, and that’s why we sleep like a baby. Or maybe, as somebody else once said, we have one thought less each year.
I take the FOX04 on an EOD schedule. I started with an 18-g vial, which I first diluted with 3 ml of bac water. It wasn’t enough to mitigate the sharp, persistent pain. I gradually upped the diluent to 9 ml, which gives me 2 mg/ml, more or less.
I know you suggest a saline solution for your spray. Any reason you couldn’t use bac water?
2 Likes
No reason at all. From what I know about nasal sprays you could also use distilled water, I get that from Walmart, it’s dirt cheap ![]() I use that in our skin care products so I don’t need to use a chelator.
I use that in our skin care products so I don’t need to use a chelator.
I do prefer a bit of “bacteriostatic” property in a nasal spray though.
That may reduce the risk of contamination, possibly? I also wipe the nozzle before and after use. Ya never know what’s lurking up there and I don’t want it growing in my spray bottle of a month LoL!
The one big BUT with nasal sprays is test the pH. I’ve had a bad experience when I made our NAC+Bromelain nasal spray.
3 Likes
Bac water has alcohol in it so I imagine it would irritate your nose cavity VS the saline
3 Likes
That is a good point. In my Selank and Oxytocin spray use Saline 0.9% Bacteriostatic 10ml Vial- With Preservative and dilute it with 10ml distilled water and no issues. I have not tried to use it full strength.
I use a BAC version as 1 full spray bottle will last about 1 month for 2 people and I’m just a bit concerned about stability.
3 Likes
Yes, a little, but not bad.
1 Like
Somewhere in this thread there is a study on old mice that when treated with senolytics had a positive effect on their testosterone output.
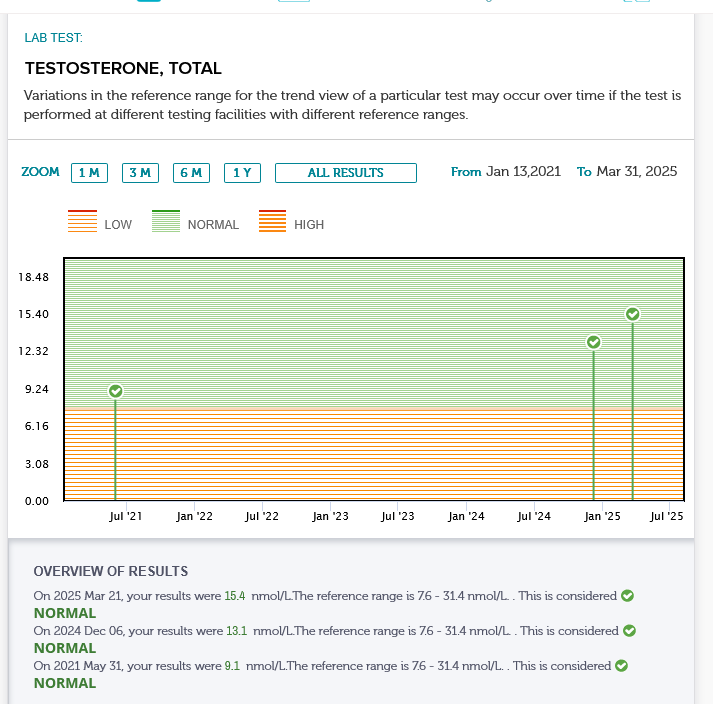
I started FOX04-DRI the end of Dec 26, 2024 and did one 6 day cycle of 3mg per day.
I’ve had 2 recent testosterone tests Dec 6 2024 and Mar 21, 2025 and one back in May 31, 2021.
had a good increase before starting FOX04-DRI and another little bump up after.
No TRT, just peptides. The only confounding factor would be that I also started Gonadorelin early in December.
I would say that made a difference and that quite possibly the FOX04-DRI is helping as well to enable the “boys” to function better with the addition of Gonadorelin.
We will be doing another cycle of FOX04-DRI next week and upping the dose from 3mg per day x 6 days to 4mg per day x 6 days.
Overall I’m pretty happy with these results considering it’s my boys doing the work. I will be getting another Test - test done in 3 months ![]()
5 Likes
I’m really curious what the implementation or ideology of using senolytics looks like.
For example, senescence is an important part of preventing cancer. During the very early stages of cancer development, a cell has picked up mutations and starts to divide abnormally, but will run into senescence as a barrier. Cells which can conquer that (by various mutations) can then keep going, where they will hopefully be picked up by the immune system and killed. The vast, vast majority of cancer cells we make will not make it through these processes. If a person actually has diagnosable cancer, no matter how small, it means that the tumour cells have already gone through that process and escaped from the immune system.
So, with these molecules like D&Q or fisestin, they are being taken orally and they are untargeted, blanket approaches which seem like they can suppress senescence - or at least alter the biomarkers we associate with it (p21, p16INK, SASP secretions etc). I assume that’s good news for tissue like muscle. But is there not a concern that you are also inhibiting one of your main early defences against cancer formation?
Once a senescent cell has done it’s job (a variety of jobs) it hangs around until it or you die. So what is the “natural” process of managing SNC’s? and does that natural process function properly as we age?
According to the studies, those particular senolytic compounds don’t “suppress” they clear, i.e. kill senescent cells (SNC)
Those particular senolytics, DQ and Fisetin are tissue/cell specific. They do not kill senescent cells in every tissue type, they are not systemic. There are about 240 cell types, most but not all can be induced into senescence. The SNC’s comprising adipose and endothelial tissues are the ones that are cleared by D+Q and Fisetin.
From what little I know, FOX04-DRI is the only universal senolytic compound, fortunately it is highly selective and appears to be “safe” in how it functions. I have not grown a horn or had a hang nail since I used it the end of Jan 2025.
When a cell is diverted into becoming senescent, it’s not specifically to “prevent” cancer as cells can become senescent from a wide variety of processes. Our immune system fights cancer directly, not just as a function of senescence.
Inducing existing cancer cells to become senescent with the objective of clearing them with targeted senolytics is a current line of research.
Once a cell becomes senescent the immune systems is supposed to remove it. When we are young our immune system is robust enough to do that and keeps the senescent cell count low. We are in fact born with some senescent cells.
As the number of senescent cells increase, these immortal cells secrete more SASP. As you have noted, SASP is the main issue. Four of these secretions are recruiters, they induce nearby healthy cells to become SNC’s and this is part of the cascade effect.
I have posted previously about the Threshold Theory of Senescence, which in a nut shell, is to try and maintain SNC’s below the harmful level throughout our lives and that becomes more important/difficult as we pass 50.
Of the 12 Hallmarks of Aging, Senescence has an effect on 9 of the other 12, only mitochondrial dysfunction is close at 8.
If one can manage senescence and mitochondrial dysfunction, one should have and excellent base to increase one’s health span.
7 Likes
Includes a section on Rapamycin. Quite interesting.
")
2 Likes
Thank you for this! And for your comments to me directly about fisetin.
I’ve been studying your formula and protocol as well as the Mayo Clinic protocol (which is fisetin only). I have a question for you, if you’re willing.
I gather that you recommend (at my age) your proprietary senolytic blend be taken for four 3-day cycles a month, then that repeated quarterly (for a total of 16 cycles per year.)
That’s different from the once-a-month 3-day cycle of the Mayo Clinic (fisetin) protocol (for a total of 12 cycles per year.)
I’m sure you have a good reason, so I’m curious why you cluster the four 3-day cycles into one month a quarter, rather than repeating them monthly as some other protocols do.
I’ve done one 3-day cycle so far with fisetin and bioperine, and it went well, so I plan to do more. As I’ve explained in our corresondance, I can’t do quercetin, so your blend is out for me. But I could perform the fisetin cycle more often to follow a pattern more like yours. So I’d love to know your thinking here. Thank you!
1 Like
Good questions ![]()
On Fisetin… the 2 published Phase 1 clinical trials I based my formula (and the many previous mouse studies) used Quercetin + Dasatinib, often called the D+Q protocol. Those studies pre-date the Fisetin studies which I don’t think have been published yet, only the trial plan has been published, AFIK, but I haven’t kept up on those. I think I’ve posted links to the 2 D+Q human studies.
I added Fisetin to the mix as it seemed the logical thing to do, combining two potential senolytics - thus the name of the company Combi-nation of seno-lytics = Combilytics. Combination therapies are often used in the pharma industry, so I figured why not ![]()
For the timing I expanded that as the trials are snapshots, no long term studies have been done. I extrapolated from short studies to a life time of killing zombie cells.
Also… neither Q nor F are the best senolytics as polyphenol flavinoids are poorly bio-available. A very high dose is required or they don’t act as senolytics. They still have other benefits at lower doses though.
Bioperine is a good enhancer but I decided to use the kitchen sink approach and used 5, not just 1.
The thing with senescent cells is they are produced slowly, until they reach a critical mass and go exponential with the “recruiting” aspect. So there is no need to do a monthly protocol and that may even be harmful as we do need senescent cells, just not too many.
That is the Threshold Theory of Senescence.
4 Likes
Looking at the Robust Mouse Longevity data, it strikes me that these may be immortal cells because killing them releases whatever caused them to be senescent into the blood stream.
Best guess this dovetails with the recent research that mitochondria can be replaced by an infusion into the blood. Essentially, if you kill a senescent cell, a bunch of defective mitochondria get released into nearby cells, resulting in no net gain.
The robust mouse longevity data also suggests that senelytics might work, if paired with an mtor inhibitor to limit the “spread on death” aspect (or maybe it’s Rapa specific and has to do with the immune effects).