I initially dismissed GLP-1 agonists as merely appetite suppressing causing weight loss which resulted in many benefits of losing weight. However there is clearly a lot more going here. They were found to have anti-inflammatory effects as well.
Personally I tried 4-5 injections of small dose about 0.8 mg every other week (basically what was left over in a vial after my wife used her 2.5 mg/0.5 ml). My initial weight was already in low normal range at 155 lbs and 5 11 height - athletic build. I managed to lose another 10 lbs on top of that. My appetite did not seem that much affected and I really didn’t reduce my calorie intake by all that much. So something else was happening for sure, because I never dropped weight so easily before (I can provide my DEXA results after I do my repeat DEXA). It was almost too much loss as my face got a bit too gaunt but the clearly defined six pack was nice. I suspect that the drug increased the metabolism although I couldn’t find any evidence online to support this.
Anyway, I am getting a sense that these class of drugs may be the actual path to anti-aging. I am not sure how they fit with everything else like rapamycin. My weight is slowly coming back about 1 lb per month, so I am thinking about some small dose on monthly basis or more.
I already stopped my weekly rapamycin (discussed in another thread) and looking to do some form intermittent dosing.
EXCITING TIMES TO BE LIVING IN !
Executive Summary
The central thesis of the provided material is the emergence of GLP-1 receptor agonists (e.g., semaglutide) as potent regulators of systemic tissue regeneration, specifically targeting the historically “irreplaceable” articular cartilage. Originally derived from Exendin-4, a peptide found in Gila Monster venom, these compounds have evolved from glycemic control agents to multi-organ therapeutics. The transcript highlights a paradigm shift in orthopedic medicine: challenging the 280-year-old dogma that ulcerated cartilage cannot recover.
Recent preclinical and pilot clinical data suggest that semaglutide exerts a weight-loss-independent protective effect on joints. While mechanical unloading (losing weight) undeniably reduces joint stress (a 1kg loss results in ~4kg less pressure on knees), mechanistic studies using pair-fed mouse models demonstrate that semaglutide specifically halts cartilage deterioration and reduces bone spurs even when weight loss is matched. This is mediated by newly discovered GLP-1 receptors on chondrocytes (cartilage cells).
Mechanistically, semaglutide appears to “flip a metabolic switch” within chondrocytes, shifting them from inefficient glycolysis to oxidative phosphorylation via the AMPK/PFKFB3 signaling cascade. This metabolic upgrade provides the requisite cellular energy for extracellular matrix repair. Preliminary human data from a 24-week pilot study involving MRI analysis showed a 17% increase in cartilage thickness in patients receiving semaglutide compared to <1% in controls. While these results are transformative, the transcript cautions that human evidence remains at the “pilot” stage, requiring larger, longitudinal RCTs to confirm regenerative claims and long-term safety.
Insight Bullets
The Venom Origin: Semaglutide is a synthetic analog of Exendin-4, a peptide from Gila Monster venom that is 53% identical to human GLP-1 but possesses a significantly longer half-life.
Weight-Loss Independence: Pair-fed mouse studies prove that cartilage preservation occurs even when caloric restriction is identical, isolating the drug effect from the mechanical effect of weight loss.
Chondrocyte Energy Upgrade: Semaglutide activates the AMPK-PFKFB3 pathway, shifting cartilage cells from “spluttering” glycolysis to efficient oxidative phosphorylation.
Cartilage Regeneration: A 20-patient pilot study demonstrated a 17% increase in cartilage thickness over 24 weeks via MRI—a result previously deemed biologically impossible * Study: Qin, Yu, Chen et al. (2026). “Semaglutide ameliorates osteoarthritis progression through a weight loss-independent metabolic restoration mechanism.” Cell Metabolism. Qin et al., 2026 (or via PubMed: 41666927)
Cardiovascular Risk Reduction: The SELECT trial confirmed a 20% reduction in major cardiovascular events (MACE) in non-diabetic obese patients (Lincoff et al., 2023).
Reward System Dampening: GLP-1 receptors in the brain reduce the “reward” response to food, alcohol (18% drop), nicotine (20% drop), and opioids (25% drop).
Kidney Protection: The FLOW trial showed significant slowing of chronic kidney disease progression, independent of glycemic control or weight loss (Perkovic et al., 2024).
Nerve/Blood Supply Barrier: Cartilage’s lack of nerves and blood vessels typically prevents repair; semaglutide bypasses this by activating resident chondrocytes directly.
Bone Spur Inhibition: Semaglutide treated groups showed significantly fewer osteophytes (bone spurs) compared to weight-matched controls.
Knee Arthritis (STEP 9): Semaglutide improved pain scores by 42 points vs. 28 for placebo in patients with knee osteoarthritis (Bliddal et al., 2024).
Universal Receptor Distribution: GLP-1 receptors are now confirmed in the heart, kidneys, brain, and cartilage, explaining the drug’s “multi-hat” efficacy.
Metabolic Switch Mechanism: The shift to oxidative phosphorylation provides the ATP necessary for chondrocytes to synthesize new extracellular matrix.
History of Dogma: Orthopedic medicine has operated since 1743 under the belief that destroyed cartilage is “never recovered.”
Systemic Anti-inflammatory: Beyond metabolic effects, the drug class exhibits profound dampening of systemic and localized (intra-articular) inflammation.
Pilot Limitation: The human cartilage regeneration data is based on 20 patients; statistical significance is high, but the cohort size is small.
Actionable Protocol (Prioritized)
High Confidence Tier (Level A/B Evidence)
Cardiovascular Protection: Utilize semaglutide (2.4mg weekly) for 20% reduction in MACE in patients with BMI >27 and pre-existing CVD, regardless of diabetes status.
Osteoarthritis Symptom Relief: Semaglutide is a validated tool for reducing OA-related pain via a combination of mechanical unloading (~13-15% weight loss) and anti-inflammatory pathways.
Kidney Preservation: For patients with Type 2 Diabetes and CKD, GLP-1 agonists should be considered to reduce the risk of kidney failure and death.
Experimental Tier (Level C/D Evidence)
Cartilage Regeneration Protocol: Based on the Chen pilot study, weekly semaglutide (titrated to 1.0mg or 2.4mg) may be paired with hyaluronic acid injections for potential structural cartilage regrowth.
Addiction/Cravings Mitigation: Off-label use for dampening reward-seeking behavior in alcohol or nicotine dependence, though large-scale RCTs specifically for cessation are still pending.
Oxidative Phosphorylation Support: Pairing GLP-1 therapy with lifestyle factors that support AMPK activation (e.g., Zone 2 exercise) to synergize chondrocyte metabolic health.
Red Flag Zone (Safety Risks)
“Magic Bullet” Fallacy: While cartilage regrew in a pilot study, it is not yet standard of care. Avoid assuming GLP-1s replace the need for joint-strengthening exercise or physical therapy.
Muscle Mass Atrophy: Aggressive weight loss via GLP-1s often involves “Sarcopenic Obesity” risks; resistance training is mandatory to prevent lean tissue loss.
Gastrointestinal Side Effects: Nausea, vomiting, and delayed gastric emptying are common; titration must be slow to ensure long-term compliance.
Pilot Data Caution: Do not interpret a 17% increase in a 20-person study as a universal guarantee of “regrowing your knees” until validated by Phase III trials.
Don’t worry, you’re not the only one with this bias. Fortunately, there are a ton of studies (on real humans!) about all the metabolic aspects that this class of drug improves coming out regularly. Hopefully more people on this forum start paying attention to them.
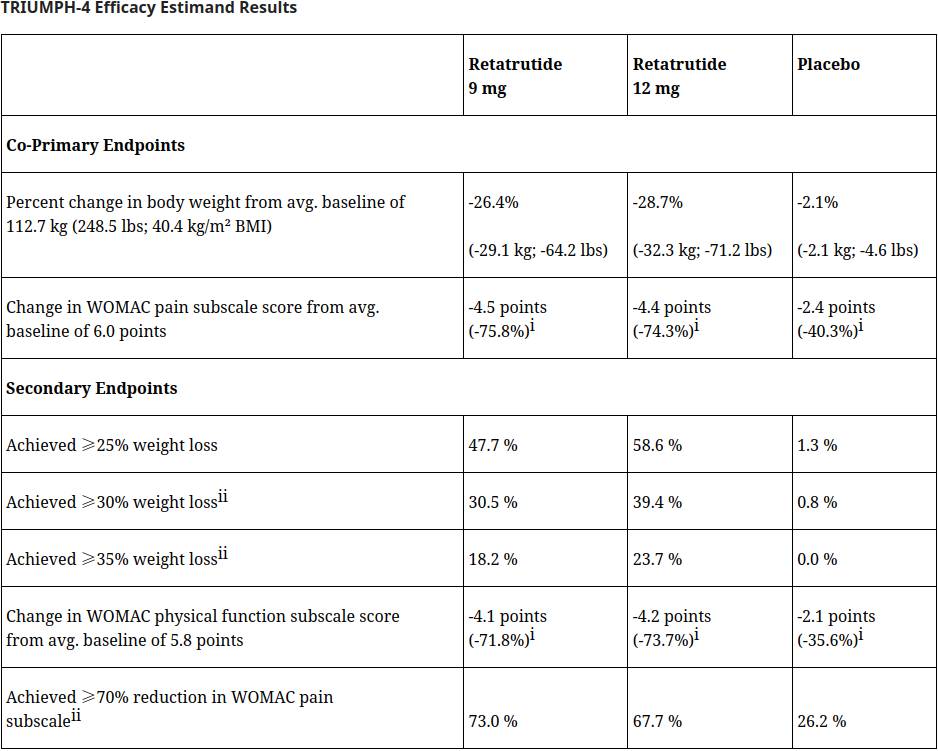
Lilly has done their own study on the effect of retatrutide on knee OA in the TRIUMPH-4 trial. Hopefully, they publish their paper on it soon, but for now here are the topline results, which show substantial knee pain reduction:
In the first-of-its-kind TOGETHER-PsO study, 27.1% of participants receiving Taltz and Zepbound reached complete skin clearance (Psoriasis Area Severity Index (PASI) 100) and at least 10% weight loss, compared to 5.8% of patients treated with Taltz alone, meeting the primary endpoint (p<0.001). In a key secondary endpoint, Taltz plus Zepbound delivered a 40% relative increase over Taltz monotherapy in the proportion of patients who achieved PASI 100 (40.6% of patients vs. 29.0%, respectively, p<0.05), demonstrating that treatment of obesity or overweight with Zepbound reduced the burden of psoriasis
To me, any drug that purports to improve metabolic outcomes on the heart, kidney, liver should at least match GLP1s.
To be fair, anyone can publish results that weight loss helps almost everything when you are overweight. And that doesn’t mean anything beyond weight loss.
You have to do the studies and get an effect without weight loss or it doesn’t matter.
I am a bariatric surgeon and use GLP-1s all the time. Love them. But all the effects you see, from my perspective, you see with surgery also.
You also see it with calorie restriction. We put people on protein shake diet pre-op and see arthritis improve. All the time. We expect skin psoriasis to improve with surgery although it isn’t universal.
And life expectancy gains of 7-10 years are common.
If you are obese with a western diet, the positive results from fixing that are universal and unbelievable. And glp-1s are a great way to get there. But it proves nothing beyond weight loss fixing everything. This mice study is interesting but it is in mice.
The other issue is food choice. You can get benefits day 1 from calorie restriction - before weight loss. And benefits are also muddled by food eliminations without weight loss. You can hold weight on a glp-1 but likely not with the same food choices. So results are muddled unless you are a mouse.
And yes. I am a carpenter/hammer and weight is my nail. I am hopeful about secondary effects but it is a tough path to prove it.
As a side note, you may see some effects with lowering blood sugars even in absence of weight loss so another muddling. That of course would be a secondary effect but have to prove better than SGLT2s, metformin or acarbose to be meaningful (and to justify the cost).
Did you miss the fine print that the effect was weight-loss independent? The control cohort lost as much weight as the semaglutide cohort but didn’t show cartilage regeneration.
My question is is this specific to sema or a universal property of all GLP-1a’s? Asking for a friend on tirza .
Agreed, but I think most people assume they are due to weight loss alone, when there is an hormonal component too (e.g., GLP1 secretions increases by a lot after surgery).
LEADER Trial: Liraglutide reduced the risk of death from cardiovascular causes by 22%. Subsequent analyses confirmed that the reduction in cardiovascular events was disproportionately large compared to the relatively modest weight loss (approx. 2-3 kg) observed in this specific study population: https://www.nejm.org/doi/full/10.1056/NEJMoa1603827
FLOW Trial: GLP-1 RAs reduce albuminuria and slow the decline of GFR. These effects are partly due to the drug’s ability to reduce glomerular hyperfiltration and local inflammation within the kidney’s filtration units, and it occurs almost immediately upon starting the medication, well before weight loss occurs: https://www.nejm.org/doi/full/10.1056/NEJMoa2403347
GLP-1 medicines also exert antiinflammatory effects independent of their metabolic benefits. For example, a single dose of exenatide or semaglutide reduced circulating TNF-α levels in mice challenged with LPS (21, 22). Separately, exenatide inhibited binding of NF-κB to DNA and downregulated TNF and IL1B in human PBMCs (23). These acute effects occur within hours and precede any meaningful weight loss.
Clinical trial data further support weight loss–independent antiinflammatory effects of GLP-1 medicines. In the semaglutide SUSTAIN and PIONEER trials, reductions in glucose and weight explained only 20%–60% of the observed CRP reductions (17). In PIONEER 2, oral semaglutide reduced CRP by 30%, whereas empagliflozin had no effect despite similar approximately 4% weight loss (24). Proteomic analyses from the STEP weight loss trials in people with or without T2D revealed semaglutide-induced changes in inflammatory and immune regulatory pathways that could not be fully attributed to metabolic improvements alone (25). Hence, preclinical and clinical studies of GLP-1 medicines, administered either acutely or chronically, suggest that a significant portion of the antiinflammatory effects of GLP-1 medicines is mediated by mechanisms independent of metabolic changes.
Yes. But in this case they seem to understand the underlying mechanism of action. And I’m curious if it’s one that is shared by them all. Or at least, in my case, tirza.
The fine print I got (I think) - it is a mice study and mice studies don’t always or even usually carry over to humans.
Without going through all the studies - the Select trial and probably others has results explainable by calorie restriction. The reps loves to point out that risk was reduced day 1 before meaningful weight loss. Sure, but after calorie restriction. The authors think in terms of weight only but restricting calories - particularly average US calories - is hugely anti inflammatory.
Yes, surgery impacts hormone levels. But some of that is just calorie restriction impacting hormone levels. Surgeons love to use the hormone argument (and I am one) but is it really something that happens independent of weight loss? I personally think so but is heavily dependent on type of surgery. Even though no one does lap bands anymore, they actually caused hormonal changes. And I am fairly certain that is just calorie restriction changes. Small bowel bypasses of various types are a different story.
Now - take a normal weight person and restrict calories with a GLP1 and you will see positive changes - in inflammation particularly. Studies are done on people with crap diets which only magnifies the anti-inflammatory effect. This will happen even if they don’t lose weight. Is this some miraculous GLP1 effect? If so, tell me how you separate any of these effects from eating less pepperoni.
I could be wrong but it is a high burden of proof to separate any effect from calorie restriction. And probably also less alcohol intake. And for some, less other stuff that they might not tell you about.
The Surpass post hoc analysis - I could not find the data that shows an effect independent of weight loss. Maybe just me but I didn’t see in the linked article. It had the obvious limitation of being a post hoc look. I found baseline BMI but didn’t see post treatment BMI.
There was a human study, watch the video again. Small 20 person pilot study with very significant difference in cartilage thickness. I was trying to find it but I don’t have access to the full paper.
Again, just like you I used to think all the benefits were due to the weight loss, I still think that most are but there is definitely mounting evidence of glp-1 having direct effect on cells/tissue independent of weight loss.
I agree. The benefits of calorie restriction are so wast that I’m going to assume that any benefits of GLP-1 drugs are caused entirely or almost entirely by the weight loss rather than by independent effects. To prove otherwise someone would have to do a study where the people take low doses of GLP-1 drugs and make sure to not eat any less or lose any weight. If that still shows benefits then we can assume it has significant independent health benefits.
That is, controlling for calorie intake in humans. I just clicked on one link that was a study that literally showed that people on GLP1s lost more weight and had a reduction in knee pain score compared to placebo. Like that isn’t helpful.
Understand some skepticism here. These are some of the most profitable drugs ever produced. Denmark’s GDP is smaller than the market value of Novo Nordisk. Novo is the primary driver of GDP growth in Denmark.
Controlling for calorie intake in humans is almost impossible outside of prison. So the skeptics know that you can’t really prove a benefit outside of calorie restriction.
I spent my career hearing from people who had less pain (and various other markers of inflammation) from calorie restriction before significant weight loss. Like magic they thought.
I tried clicking on the Cell article about cartilage in humans. All I got was a summary and I did note that it was a Chinese article. But the summary didn’t have much and the full article was behind a paywall.
What do you think is going on with the mental health signal — reward dampening too much?
And yes the benefits seem to extend well beyond weight loss. No one losing weight by any other means had previously been shown to regrow cartilage. I first got excited over them from reading a paper from maybe 2-3 years ago over how tirzapetide had caused multi organ rejuvenation in mice completely independent of weight loss.
There are also plenty of people taking a GLP1-RA for glucose control and who don’t loose any weight nor appetite at a 5mg dose.
In my case I’ve not lost any weight at all and I’m still at the same 65kg (BMI 21.5) after 1.5 year of TZ.
My diet has not changed, and I’m doing the same marathon training/running.
Besides a small reduction in glucose, I’ve noticed a slight increase in ketones and my DEXA body fat went from 18% to 14% which is nice.
The study is mainly Chinese, but has also authors from Aberdeen and Washington university
The Cell article is only about metabolic OA, not OA in general.
In both trials, mice and human, all particpipants were obese.
So what might have worked in obese mice/human in this study might not work for non-metabolic OA meaning people with OA which are not obese or having a metabolic disease.
Weight loss was controlled only in the mice study, but not in the human clinic trial. So in humans it might still be a weight loss effect. Although unlikely as cartilage has partially recovered. But maybe nobody checked this before and it happens frequently after significant weight loss?
Nevertheless, the mechansim study with mice looks very sound to me and together with the human trial I inclined to think that it is a GLP1 effect.
For the ones who want to try this: They have used 0.5 Semaglutide per week for 24 weeks.
And no, I would not recommend to use another GLP1 RA if the target is OA as GLP1 is the key driver here. Semglutide has the strongest affinity to GLP1 receptor. The other ones have signfiicant lower GLP-1 activity.