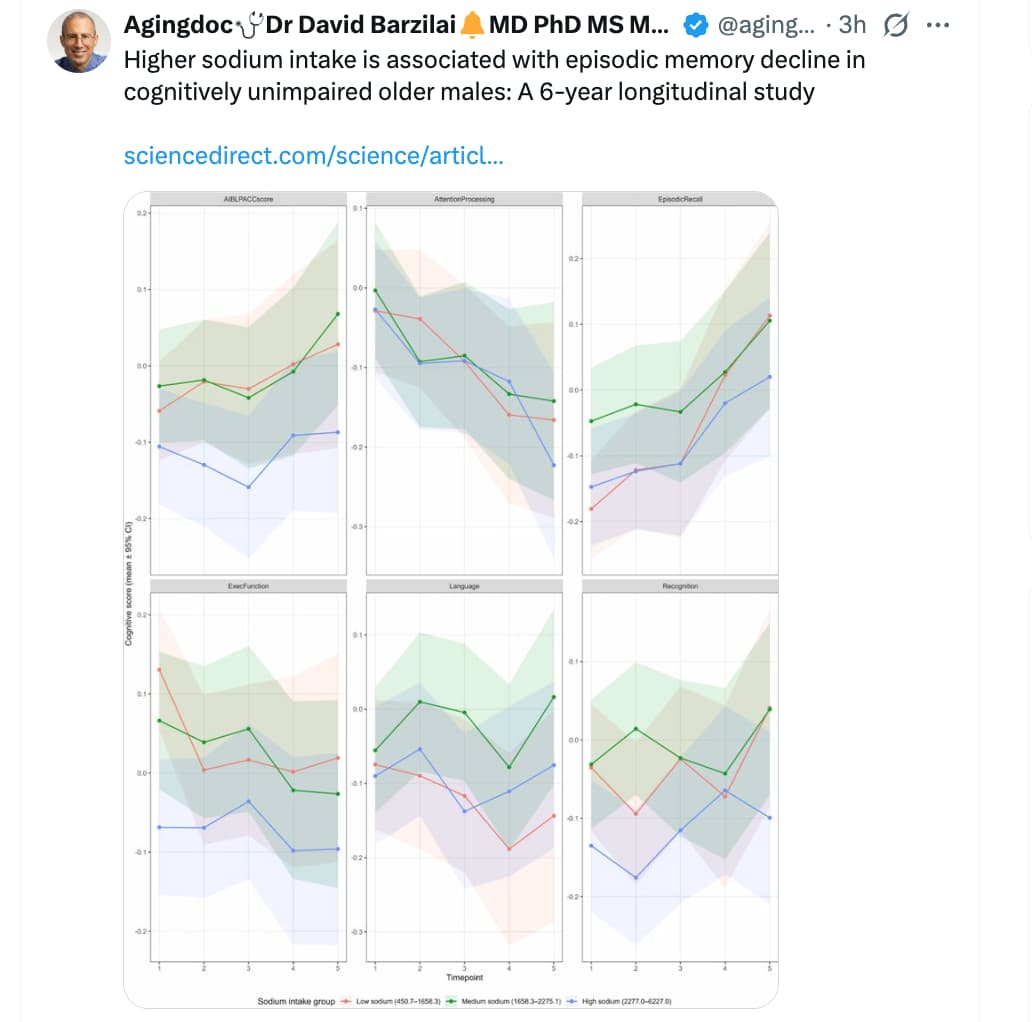
I know what you may be thinking. I have cherry picked one study to make a point. Well yes, this is just one study. However, it is the biggest and longest ever done. It represents one small part of the National Health and Nutrition Examination Survey (NHANES).
And, although it is only a small part, it represents very nearly ‘one-million-person years’ of observation. Of course, like all nutritional studies it has its weaknesses, but you will find nothing bigger, longer, or better than this. And if you want to find one that contradicts it – feel free – and good luck.
This is the full study, which has many more graphs like the one used. Most ages go up in a U shape, but that one was for people 40-60 and it did not.:
Apparently, almost everything that I like to eat accelerates aging. Some people, including one of my daughters, enjoy very low or no salt in their food. I do not need excess salt, but many things that I eat like steak and potatoes, are very bland without it
If food is not a joy to eat, I’m not interested.
As you know well, with age people’s ability to taste salt declines. This is a big reason why many elderly people tend to put a lot of salt in their food - I’ve observed this with a friend of mine who prided himself in being a great amateur chef. He loved throwing parties and serving up a feast he cooked. Well, when he moved into his 70’s, we all noticed his food got notably saltier, to the point where some of us could no longer enjoy it, while others who aged in concert with him kept loving it.
As I have low blood pressure, LDL and triglycerides I personally am not worried about increased heart attack risk from salt intake. But there seems to be strong evidence it causes stomach cancer. You see this in Japan in places where they eat huge amounts of miso. So I would avoid excess intake regardless.
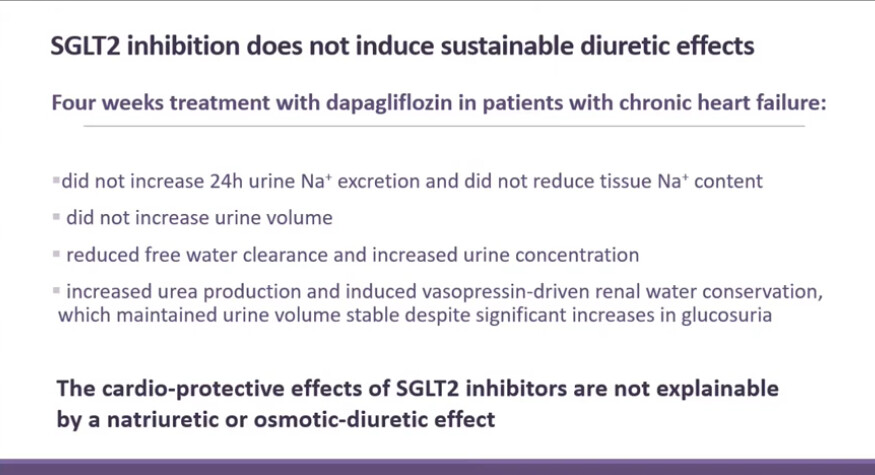
Titze claimed also that dietary salt does not increase blood pressure through extra cell volume expansion, which is the common view. Makes sense in the scenario salt increases risk of chronic hypertension (regardless of later intake after diagnosis), and salt exposure might cause hypertension in some way seen as hypertension prevalence with aging?
This is also why excess salt intake might be bad even if you have low or normal blood pressure @Tilmitt
I take a mix of potassium bicarbonate, sodium bicarbonate, sodium chloride and magnesium chloride for gout, which is working quite well as far as uric acid levels. The mix which I take daily gives me an intake of 1.78 g of sodium and 4.6 grams of potassium, along with 0.3 grams of magnesium. This gives a potassium:sodium ratio of 2.6. The daily intake of sodium chloride equivalent from the salt and baking soda is 4.54 gms/day. Which is ~3 grams higher than recommended. I do not have high blood pressure.
My reasoning is that the literature strongly suggests that it is not sodium intake that correlates with blood pressure in some individuals, but the potassium to sodium intake, that ideally should be 3:1. Rarely accomplished in an American diet, in fact, it is the inverse.
Aldosterone secretion is inversely proportional to sodium intake. And where it gets interesting is that aldosterone levels correlate well with measures of inflammation such as hsCRP, along with other pleiotropic effects on the heart and immune system.
My conjecture is that maybe pushing a low sodium intake of 1.5 grams a day, without paying attention to potassium intake, may not be ideal, for either normotensives, nor hypertensives, as it will result in relatively higher aldosterone levels and higher levels of inflammation, along with its less than ideal effects on the whole Renin-Angiotensin-Aldosterone System (RAAS).
Of course, there is a lot of interacting physiology here, in the context of genetic variations in response to diet.
You should measure your urinary pH. I use citrate (I am nowhere near gout, but I use citrate anyway). My urinary pH a few minutes ago was about 9.5.
I personally I am not a fan of supplementing chloride and I have not tried bicarbonate in recent years (when I have been measuring everything). I would be, however, interested in any reasons why bicarbonate is better than citrate for alkanizing.
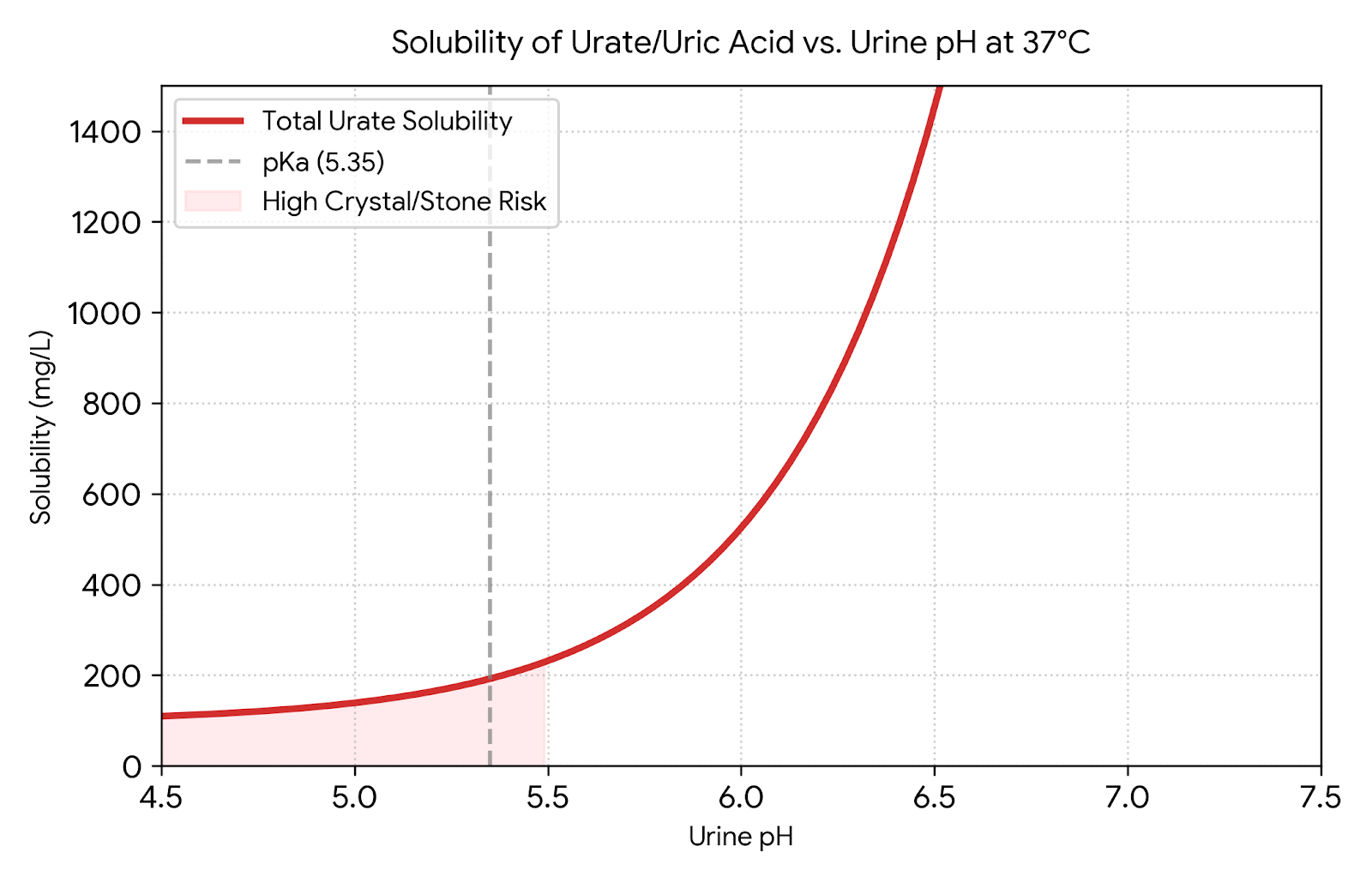
Here is part of a chatGPT (5.5 paid) answer about the solubility of urate (uric acid) in urine at various pHs.
Below is an approximate theoretical chart of total uric acid/urate that could remain dissolved across the usual urine pH range. I used:
This assumes an undissociated uric acid solubility of about 96 mg/L at 37°C and a pKa around 5.35. In real urine, sodium, potassium, ammonium, ionic strength, temperature, and nucleation surfaces can alter this. Urine pH commonly ranges roughly 4.8–7.4, and low urine pH is a key driver of uric acid crystallisation. (PMC)
Urine pH
Approx. dissolved total urate species, mg/L
Approx. mmol/L
4.8
123
0.73
5.0
139
0.83
5.2
164
0.98
5.35
192
1.14
5.5
232
1.38
5.8
367
2.18
6.0
525
3.12
6.2
776
4.61
6.5
1,452
8.64
6.8
2,802
16.67
7.0
4,384
26.08
7.2
6,892
41.00
7.4
10,867
64.64
The main point is that small pH shifts matter a lot. Moving urine from pH 5.0 to 6.0 increases estimated soluble urate species by roughly 3.8-fold; moving from 5.0 to 6.5 by roughly 10-fold. This is why uric-acid stone prevention/dissolution strategies often focus on urine alkalinisation, while avoiding over-alkalinisation because of other stone risks.
If people are being cautious they target 6.8 as that reduces the risk of CaP stones.
I measure urine pH at least once or twice a day and it stays >8, and as you point out, this is key to keeping urate in solution and increasing its renal clearance. I take potassium bicarbonate and a bit of sodium bicarbonate instead of potassium citrate (I assume this is the form of citrate you are using). When the citrate is metabolized the strong anions K+, it drives up the pH. KHCO3 is a more direct way of achieving the same aim. I find citrate upsets my stomach a tad, and both bicarbonates are cheaper. I also don’t have calcium stones, so I don’t need the citrate in the urine. Potassium bicarbonate also lowers bone turnover and keeps the K:Na ratio closer to 3, which may help with blood pressure, though I do not have that problem, at least for now. I was influenced by the reports of inflammatory effects of aldosterone, so while waiting for further data, figured a bit more Na in the diet is not a bad thing, if counterbalanced by additional K.
Nice chart! Thanks! Taking it to my rheumatologist at our next meeting! He is still sceptical in spite of much literature on urinary alkalinization driving down serum urate. Also in spite of my success: went from ~10 to 5.2 mg/dL over a few months with no attacks. But at least he continues to work and care for an unusually idiosyncratic patient, unlike other physicians I have known.
Forgot to mention another reason I add NaCl to the mix. I drink 54 oz of the electrolyte mix in RO water a day. I added a bit of salt because because when I first started the regimen, I was peeing a whole lot, which meant on the physiological level, that I was supressing vasopressin (anti-diuretic hormone) by diluting the Na level in blood with “free water,” as the nephrologists like to call it, so the kidneys immediately responded to lower vasopressin levels by opening up the gates.