Gosh you’re right, that’s insane. An example of inefficiency in a state run system. But i agree, most if what they do produce is decent.
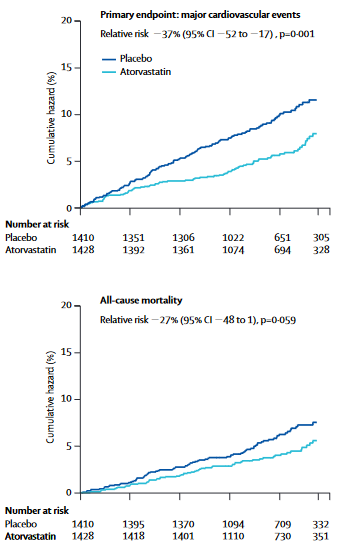
This study halted prematurely as well, the end is a follow up, and led to the statistical significant effect, so it is a limitation (see end of LLA in the graph, which also “converged” a bit).
1 Like
When comparing statins with more or less the same lipid-lowering properties there are still some differences in outcomes.
So, are there some beneficial effects from statins that are not related to their lipid-lowering properties? If so, what are the beneficial side effects of the different statins?
1 Like
I understand that besides their lipid-lowering effect, statins also:
- Decrease hsCRP
- Enhance the production of pro-resolving mediators (SPMs) that reduce inflammation: https://www.sciencedirect.com/science/article/abs/pii/S0026049522000890
Other potential effects:
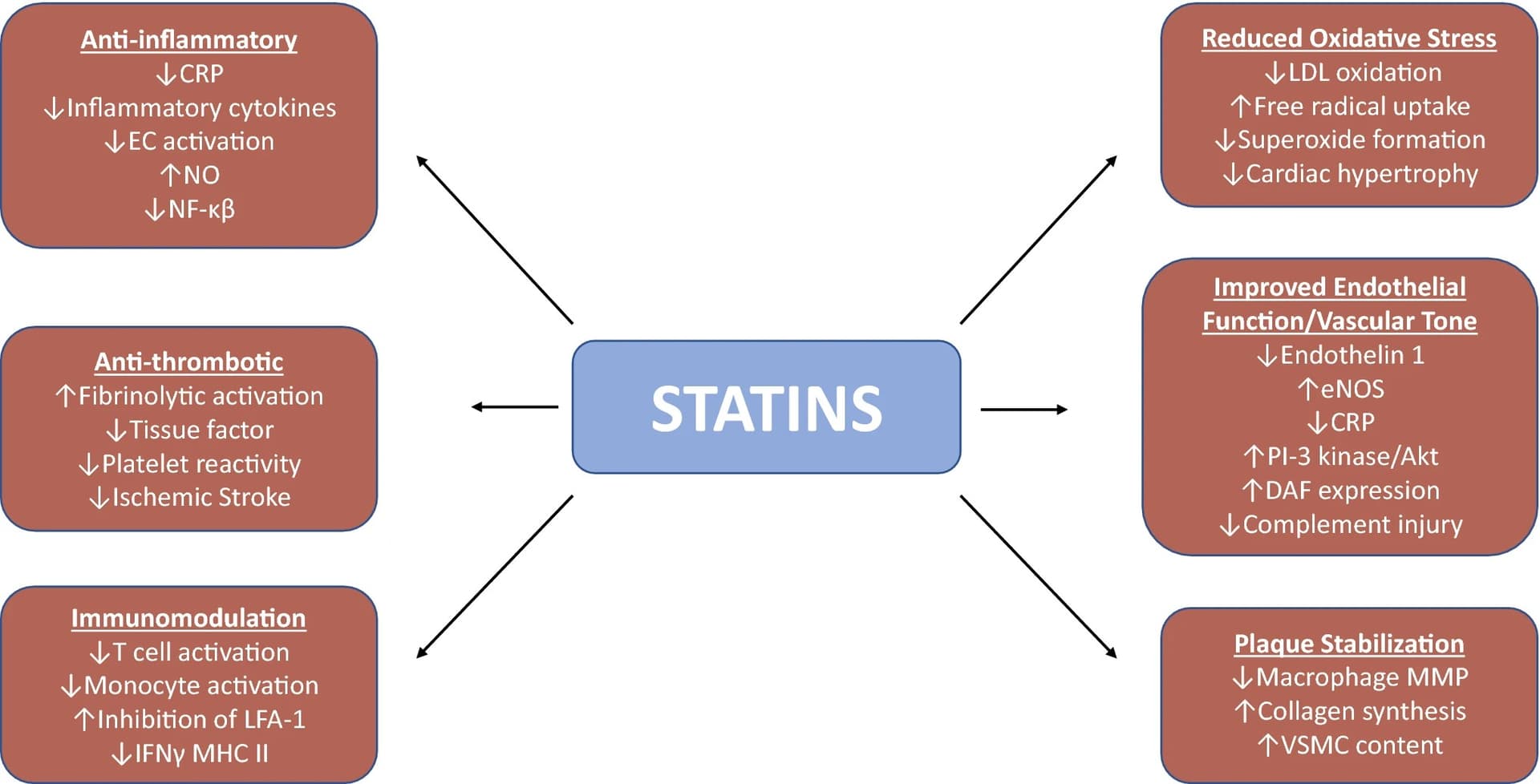
Understanding the molecular mechanisms of statin pleiotropic effects 2023
Do we have papers looking at the effects of various statins on oxidative stress, hsCRP, SPMs, and endothelial function?
5 Likes
The antiinflammatory affects are probably very important too. The strong short term benefit post a cvd event is probably due to those. But you make a good point, i should have emphasized that NICE regarded the evidence for atorvastatin benefit as strongest.
Each of the statins interact with different liver enzymes which may partially account for different side effects.
2 Likes
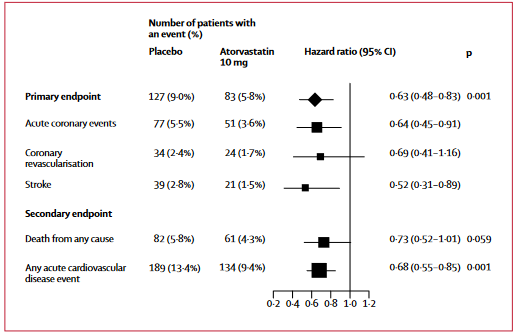
colhoun2004-1.pdf (198.9 KB)
P=0.059 so technically not statistically significant, but I am pretty much convinced that atorvastatin reduce all-cause mortality in primary prevention for heart disease.
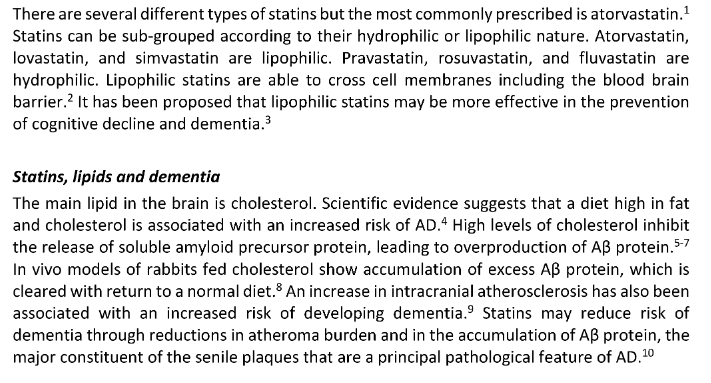
I did try 20 mg atorvastatin for a few days but I switched back to rosuvastatin. I will try again since the drug pretty much reduces all-cause mortality, all statins cross the BBB, and more importantly it has a lower causal risk of diabetes compared with rosuvastatin. If it wasn’t for the latter I wouldn’t try and switch.
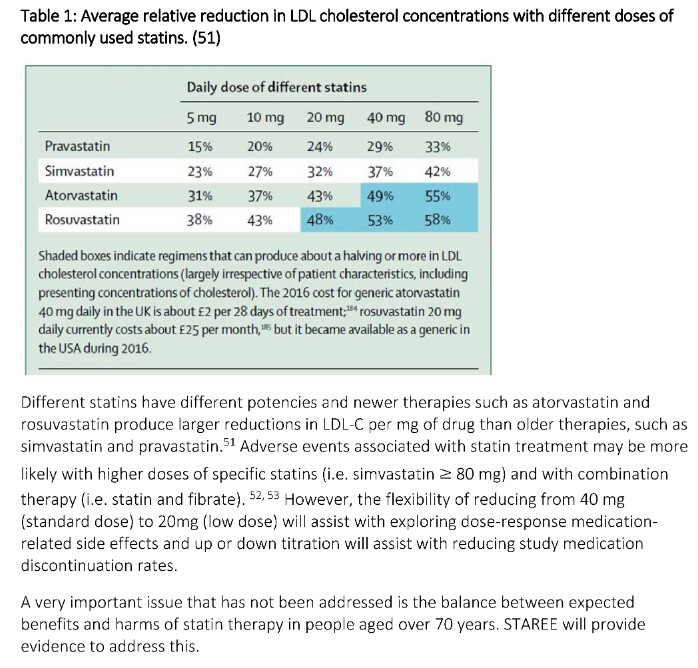
The STAREE trial and STAREE-MIND trial chose 40 mg atorvastatin as well for its research, reading a bit in the supplementary information, they cite research which suggest lipophilic (meaning drugs that can pass the BBB), might be superior for dementia and as many of us know APOB causes Alzheimer’s according to MR studies.
bmjopen-2023-April-13-4–inline-supplementary-material-3.pdf (2.9 MB)
bmjopen-2023-April-13-4–inline-supplementary-material-2.pdf (3.0 MB)
Meanwhile, until we know more about Lipitor vs. Crestor for dementia and Alzheimer’s, for example in E4 carriers of APOE, I think Lipitor is probably better based on current information. The STAREE trial should tell us more? (vs. bempedoic acid, PCSK9i and ezetimibe, I still think statins have more data like for mortality and net benefit, thus they are right now superior?).
1 Like
Alongside a very likely decrease in all cause mortality, statins like atorvastatin seem good in reducing stroke, that does often reduce healthspan significantly I think, even if they are non-fatal.
2 Likes
Regarding AD, this trial found no cognitive improvement after 24 months of aerobic training + atorvastatin 80 mg + losartan + amlodipine in people at high risk of AD: ClinicalTrials.gov
Assumptions:
- The trial was too small?
- The effects can only be seen after a longer period of time?
- High dose statin is detrimental? (cf. UK Biobank study)
- Intensive BP control is detrimental?
2 Likes
Where did you find the study results?
I can’t see any nor any publications.
I emailed the guy to get the results, not yet published.
3 Likes
By the way, if I’m correct, with the exception of the French statin cessation study, we won’t get new RCT results regarding statins and cognition until 2025/2026 (see: Rapamycin and risk of cardiovascular disease - #3064 by adssx ). So only retrospective, MR, or animal studies could bring new insights in the meantime. Or an RCT of another lipid-lowering drug (obicetrapib ![]() ).
).
3 Likes
The study doesn’t mask the cessation of the statin with a placebo pill, and the primary outcome is a subjective measurement using EQ-5D scale. The second primary endpoint is total mortality which is hard to detect in 36 months? That doesn’t sound so useful to me. But it has some other secondary outcomes.
Another massive study testing atorvastatin in older adults for healthspan!
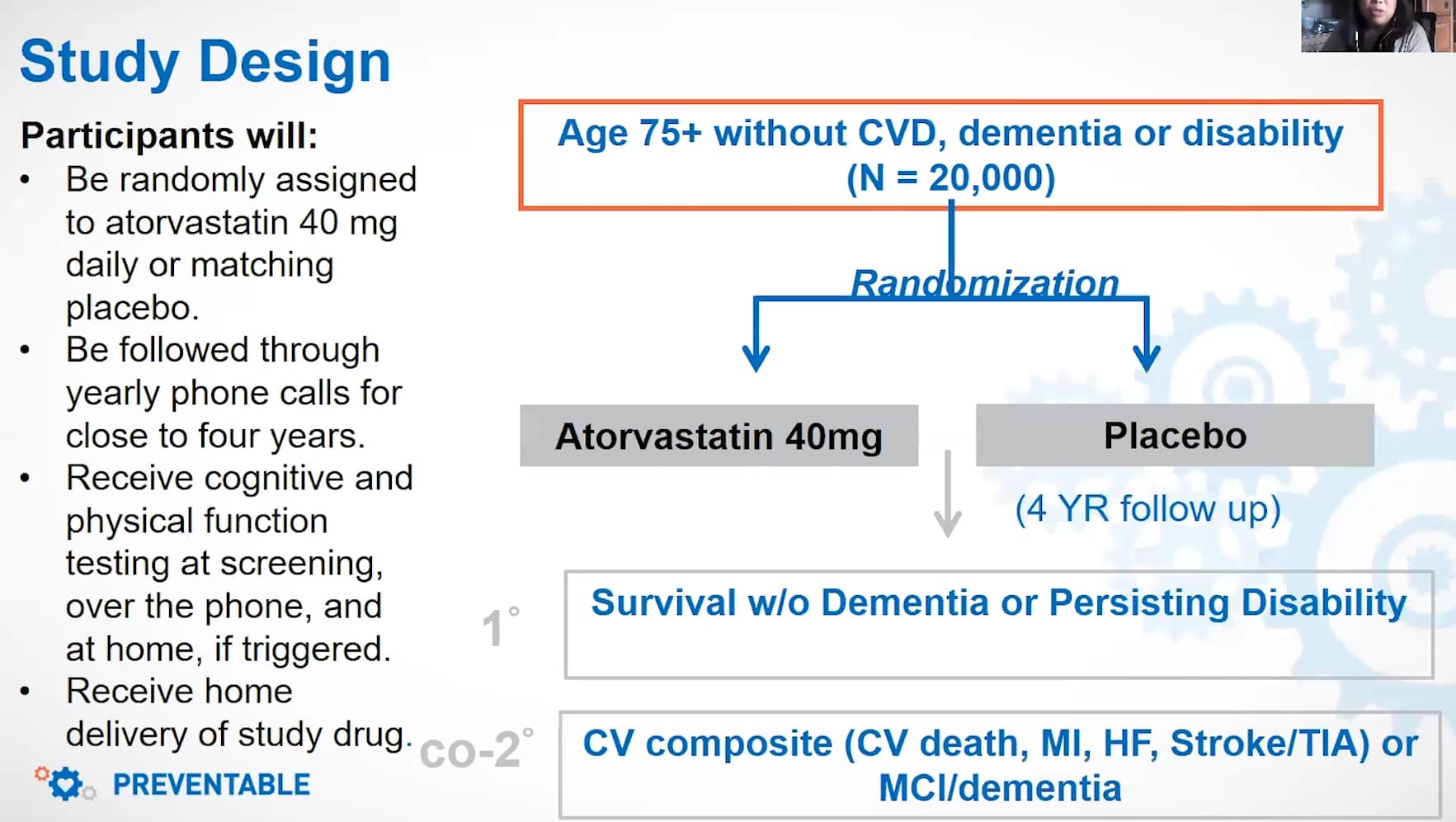
The recruiting PREVENTABLE study, where 20,000 older adults above age of 75 is randomized to 40 mg atorvastatin or placebo.
Atorvastatin, and all statin medications, do more than just lower cholesterol. These drugs also reduce inflammation and they may help prevent memory loss, improve physical function, and even prevent cancer.
Lipid levels are most useful to help understand an individual’s long-term health risk to
prevent heart disease, but you have already lived past age 75 without heart disease. Congratulations!
From the FAQ (2022)
So two massive trials are expected to be done for atorvastatin at 40 mg in older adults: STAREE and PREVENTABLE.
Whether initiation of statins could increase survival free of dementia and disability in adults aged ≥75 years is unknown. PREVENTABLE, a double-blind, placebo-controlled randomized pragmatic clinical trial, will compare high-intensity statin therapy (atorvastatin 40 mg) with placebo in 20,000 community-dwelling adults aged ≥75 years without cardiovascular disease, disability, or dementia at baseline. Exclusion criteria include statin use in the prior year or for >5 years and inability to take a statin. Potential participants are identified using computable phenotypes derived from the electronic health record and local referrals from the community. Participants will undergo baseline cognitive testing, with physical testing and a blinded lipid panel if feasible. Cognitive testing and disability screening will be conducted annually. Multiple data sources will be queried for cardiovascular events, dementia, and disability; survival is site-reported and supplemented by a National Death Index search. The primary outcome is survival free of new dementia or persisting disability. Co-secondary outcomes are a composite of cardiovascular death, hospitalization for unstable angina or myocardial infarction, heart failure, stroke, or coronary revascularization; and a composite of mild cognitive impairment or dementia. Ancillary studies will offer mechanistic insights into the effects of statins on key outcomes. Biorepository samples are obtained and stored for future study. These results will inform the benefit of statins for increasing survival free of dementia and disability among older adults. This is a pioneering pragmatic study testing important questions with low participant burden to align with the needs of the growing population of older adults.
PREVENTABLE will be the largest trial conducted in adults ≥75 years in the United States and is tailored to answer key clinical questions while limiting participant burden
Results will establish whether initiating a high-intensity statin is effective in lengthening health span in older patients without heart disease or dementia
First proven healthspan increasing drug in humans is atorvastatin? What’s the chance for this? It seems high.
3 Likes
I love it - well done! Its this kind of thing that I find really helpful at this site. People making the extra effort to get access to the good new data!
4 Likes
For now, we don’t know whether statins prevent dementia but we know with a high likelihood that they are a net benefit based on all cause mortality data. It is promising two large trials, and the largest trial ever done in older adults in the U.S, and for dementia prevention, has chosen high-intensity atorvastatin for investigation. Is that a signal meanwhile for a very good risk. vs. reward calculation?
1 Like
It just signals that researchers seem to think that atorvastatin is the best statin for dementia prevention. But atorvastatin failed in the previous trial I mentioned. So wait and see.
Two of four groups used atorvastatin in that study and in combination with other drugs so you don’t know what is causing what. It isn’t surprising either because of the relative few participants it couldn’t detect neither harm nor benefit if I understand it correctly in the time period of the study.
I hurt a finger a little bit some while after switching to atorvastatin, is it possible it could affect the tendons in some way (especially in comparison to rosuvastatin)? It felt like something in the knuckle of a finger snapped a bit. It has gotten better over time. Never had a problem like that before, and it felt so random. So I’ll try Crestor 5 mg for awhile again. I might switch back to atorvastatin later, but to be honest I am not so worried about the diabetes risk etc which I can monitor.
@DeStrider I think you have mentioned some study that had to do with something like this at some point.
My tendons have been weak either way so I might’ve been predisposed for my finger to go visit snap city. Exercise most likely helps with this.
Statin treatment increases the clinical risk of tendinopathy through matrix metalloproteinase release – a cohort study design combined with an experimental study
2 Likes