MMP-1, -3, and -9 appear to play important roles in the etiopathogenesis of rosacea. Interestingly, patients with AD have increased levels of MMP-3 in their cerebrospinal fluid, and levels of MMP-3 correlate with the duration of AD. Tetracycline reduces kallikrein 5 serine protease activity through inhibition of MMP expression in endothelial cells and keratinocytes, which in turn blocks the proteolytic cleavage of cathelicidin into the AMP LL-37, which is thought to play a role in subtypes of rosacea. It is also notable that results from multiple studies have demonstrated suppressed β-amyloid and tau protein expression, as well as neuroprotective effects, following treatment with tetracycline. This suggests that tetracycline may have therapeutic potential in patients with dementia, including AD, although this is hypothesis-generating and requires further study. Although involvement of AMPs is well-established in rosacea, β-amyloid (which itself is an AMP with proinflammatory abilities) is central to the pathology of AD. The current sum of evidence suggests that certain forms of dementia, in particular AD, have prominent inflammatory components, and MMPs and AMPs may provide mechanistic links for the observed association between rosacea and dementia. However, other proinflammatory mediators may also play a role, and a very recent study found substantial levels of T-cell involvement and increased gene expression levels for a range of cytokines, for example, IL-17 and TNF-α, in facial biopsies of patients with rosacea across all subtypes, and a considerable role for IL-17 in AD has also been suggested. In potential further support of an inflammatory component in AD, studies have associated AD with diabetes, and AD is sometimes referred to as “type 3 diabetes.” Moreover, numerous epidemiological studies have demonstrated a significant decreased risk of AD following treatment with nonsteroidal anti-inflammatory drugs.
Ocular rosacea is a chronic potentially sight-threatening inflammatory condition, which can occur in approximately 20% of patients without skin involvement. However, an accurate diagnosis of ocular rosacea has not been defined yet due to its rather nonspecific symptoms and clinical findings. Therefore, this article updates the current recommendations for diagnosis and treatment of ocular rosacea and the previously published consensus recommendations from the ROSCO expert panel on the management of rosacea.
Spironolactone is a diuretic with antiandrogenic action. Daily use provides some improvement in some adult patients with acne vulgaris. To study the effect of spironolactone on the risk for developing rosacea, investigators conducted a large population-based, case-control analysis using the U.K.-based General Practice Research Database. Each of 53,927 rosacea cases were randomly matched to one control case on the basis of age, sex, general practice, calendar time, and years of recorded history in the database. Results were adjusted for smoking, alcohol consumption, body mass, and diuretic use (15.5% of patients had received a diuretic).
Use of high- and low-ceiling diuretics and amilioride/triamterene diuretics showed no decreased “risk” in rosacea. Spironolactone use, however, decreased risk (odds ratio among 281 cases and 327 controls, 0.47; 95% confidence interval, 0.35-0.63). Among current spironolactone users without a previous diagnosis of an androgenic skin disease, the OR for rosacea was 0.39 (95% CI, 0.27-0.64; consistent findings in both men and women). These results suggest that spironolactone recipients have a decreased risk for developing rosacea during active use.
Dry eye, the most common eye disorder [1], is frequently accompanied by blepharitis (eyelid inflammation) which has an overall prevalence of nearly 40%, ranging from around 20% in 10–19 year-olds to 70% in those over 60 [2]. Meibomian gland dysfunction (MGD) is the leading cause of evaporative dry eye and is a type of posterior blepharitis that encompasses inflammation posterior to the grey line of the lid margin [3]. Rosacea is a chronic inflammatory skin disease and is also a common disorder with estimates of upwards of 10% of individuals affected [4,5]. Ocular rosacea is present in up to 58% of cases and is frequently under-recognised by ophthalmologists and other eyecare professionals as ocular signs precede skin involvement in 15% of the cases [6,7,8]. It is characterised most commonly by MGD and posterior blepharitis [9]. Studies have found significant differences in MG secretion (meibum) composition between those with MGD and controls, including the consistent presence of cholesterol esters in MGD patients [10]. Young and middle-aged MGD sufferers, as well as rosacea patients, have both been documented to have a significantly higher blood cholesterol than controls [11,12]. We hypothesise that ocular rosacea patients may have associated elevated cholesterol levels and increased systemic inflammation, such that ocular rosacea maybe a marker that healthcare professionals could use to enable the earlier identification and control of cardiovascular disease and tear film stability through timely cholesterol-lowering and inflammation reduction with statins.
Several studies have explored the pathogenesis of rosacea, and our understanding of the cutaneous biology of the disease has evolved considerably. 25 Specifically, several biologic aberrancies appear to contribute to the development of rosacea, including toll‐like receptors, 26 , 27 kallikrein‐related peptidase 5 and cathelicidin LL‐37, 28 nuclear factor κB, 29 myeloid differential factor‐88, 30 and multiple genetic factors. 31 , 32 These steps towards a pathogenetic construct suggest multiple discrete checkpoints that may be amenable to selective manipulation for the treatment of rosacea.
Wladis et al previously implicated p38 and ERK in the pathogenesis of rosacea, 9 suggesting a role for suppression of the MAPK pathway to arrest rosacea. MAPK inhibition has emerged as a meaningful treatment strategy for several diseases, including melanoma, non‐small cell lung cancer, and neurofibromatosis. 33 , 34 , 35 The current study repurposed an FDA‐approved MEK inhibitor as a topical preparation to target rosacea. To minimise systemic absorption, we suspended trametinib in a highly hydrophobic base. Consistent with minimal absorption, we did not detect any drug in circulation, indicating that patients are very unlikely to experience systemic adverse events. Furthermore, we did not detect any local adverse events, and the active medication was well‐tolerated.
Several studies have explored the pathogenesis of rosacea, and our understanding of the cutaneous biology of the disease has evolved considerably. 25 Specifically, several biologic aberrancies appear to contribute to the development of rosacea, including toll‐like receptors, 26 , 27 kallikrein‐related peptidase 5 and cathelicidin LL‐37, 28 nuclear factor κB, 29 myeloid differential factor‐88, 30 and multiple genetic factors. 31 , 32 These steps towards a pathogenetic construct suggest multiple discrete checkpoints that may be amenable to selective manipulation for the treatment of rosacea.
A treatment for ocular rosacea using p38 and Erk kinase pathway inhibitors, which are believed to block the initial reaction to rosacea triggers and thus make it possible to prevent or minimize the skin reaction. The treatment is premised on a careful analysis of the alteration of cell-signaling pathways that facilitate the development of rosacea, which led to the identification of discrete targets for highly specific therapeutic intervention in the management of rosacea.
Rosacea is a chronic inflammatory skin disease originated from damaged skin barrier and innate/adaptive immune dysregulation. Toll-like receptors (TLRs) sense injured skin and initiate downstream inflammatory and immune responses, whose role in rosacea is not fully understood. Here, via RNA-sequencing analysis, we found that the TLR signaling pathway is the top-ranked signaling pathway enriched in rosacea skin lesions, in which TLR7 is highlighted and positively correlated with the inflammation severity of disease. In LL37-induced rosacea-like mouse models, silencing TLR7 prevented the development of rosacea-like skin inflammation. Specifically, we demonstrated that overexpressing TLR7 in keratinocytes stimulates rapamycin-sensitive mTOR complex 1 (mTORC1) pathway via NFκB signaling. Ultimately, TLR7/NFκ B/mTORC1 axis promotes the production of cytokines and chemokines, leading to the migration of CD4+T cells, which are infiltrated in the lesional skin of rosacea. Our report reveals the crucial role of TLR7 in rosacea pathogenesis and indicatesa promising candidate for rosacea treatments.
Similar to the result of NFκB inhibition, inhibition of mTORC1 by RAPA downregulated the production of cytokines and chemokines, as well as the migration of human T cells raised by R848 (Fig. 5F, Figs. S5D–S5F).
In summary, hyperactivated TLR7/NFκB signaling may stimulate mTORC1 signaling, and encourage the production of cytokines and chemokines to recruit T cells afterward.
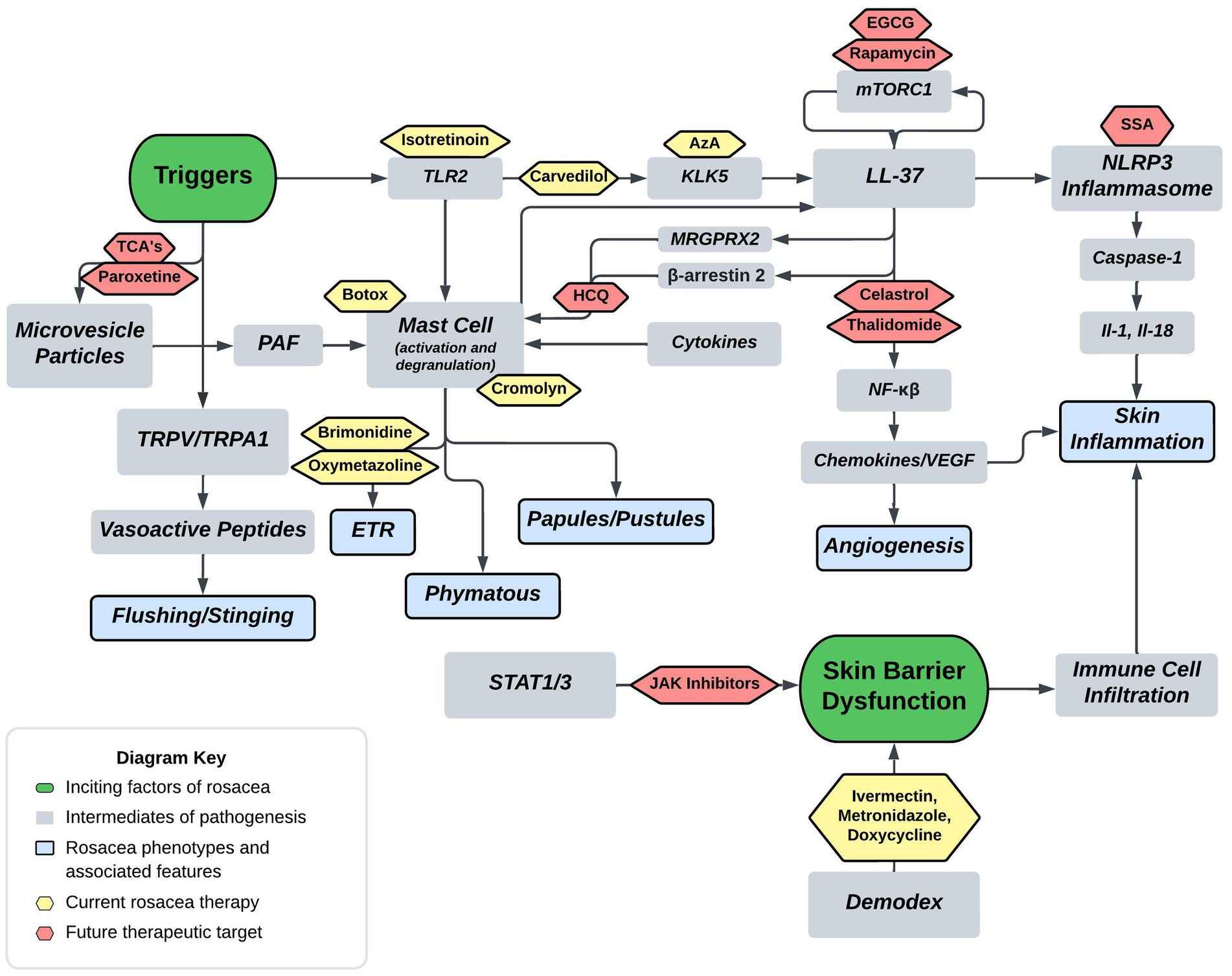
Cathelicidin pathway
As discussed previously, cathelicidin LL-37 is an anti-microbial effector molecule of the innate immune system, and in rosacea, exhibits defects in expression, function and processing (91). Figure 1 highlights the LL-37’s role in rosacea pathogenesis, including its actions on mast cells, NF-kβ activation, and promotion of NLRP3 mediated inflammasome activation. Additionally, Figure 1 depicts that TLR-2 responds to PAMPs and DAMPs which induces KLK-5 to cleave and activate LL-37. Mammalian target of rapamycin pathway, mTORC1 has been shown to regulate the cathelicidin through a feedback loop, and hyperactivation of its signaling aggravates rosacea features and is required for angiogenesis in the development of rosacea (33, 92). Rapamycin (Sirolimus) is a modulator of mTORC1, that is under investigation as a potential therapeutic. Topical rapamycin has been shown to significantly improve rosacea symptoms through its antiangiogenic and antiproliferative properties (33, 93). The mTOR pathway is a regulator of autophagy in keratinocytes, and reduced autophagy was shown in keratinocytes of a rosacea mouse model (31, 94). Importantly, it has been described that autophagy protects keratinocytes against injury in inflammatory diseases (95).
Rosacea is a chronic facial inflammatory skin disease that occurs with dysfunction of the immune system. Colchicine was reported to have anti-inflammatory properties. However, the impact of colchicine on rosacea remains unclear. In the present study, the phenotype of rosacea lesions was evaluated by the redness score, inflammatory biomarkers were analyzed by reverse transcription PCR (RT‒PCR), and the infiltration of inflammatory cells was assessed by IHC analysis and immunofluorescence in a rosacea-like mouse model. In vitro, RT‒PCR was used to identify the inflammatory factors that Toll-like receptor 2 (TLR2) agonist caused neutrophils to produce, and immunofluorescence and coimmunoprecipitation were used to identify putative signalling pathways. We found that skin erythema and histopathological alterations, as well as elevated proinflammatory factors (IL-1β, IL-6, TNFα, CXCL2) and CAMP, were significantly ameliorated by colchicine treatment in LL37-induced rosacea-like mice. In addition, colchicine reduced the colocalization of TLR2 and neutrophils and the formation of neutrophil extracellular trap networks (NET) in mouse lesions. In neutrophils, colchicine markedly reduced TLR2 agonist-induced inflammatory biomarker expression, NET formation, and ROS production. Moreover, we found that LL37 could bind to TLR2 upon activation of TLR2 in neutrophils. Importantly, colchicine could repress the combination of TLR2 and LL37 in vivo. Finally, bioinformatics methods further validated the key molecules of neutrophil-related inflammation in rosacea, which is consistent with our experimental findings. Collectively, colchicine ameliorated rosacea-like dermatitis by regulating the neutrophil immune response activated by the TLR2 pathway, indicating that it could be an effective therapeutic option for patients with rosacea.
We found that roflumilast treatment improved survival in septic mice by reducing bacterial load locally and systemically, inhibiting the expression of pro-inflammatory cytokines interleukin-6 and tumor necrosis factor alpha, and alleviating liver injury. These effects were associated with the inhibition of nuclear translocation of nuclear factor-kappa B (NF-κB), as well as degradation of NF-κB inhibitory protein alpha. The phosphorylation of p38 mitogen-activated protein kinase (MAPK) was also markedly inhibited by roflumilast. Moreover, roflumilast significantly suppressed the activation of signal transducer and activator of transcription 3 (STAT3) and its upstream Janus kinase 1 and Janus kinase 2. Taken together, these results indicate that roflumilast prevents polymicrobial sepsis likely by suppressing NF-κB, p38 MAPK, and STAT3 pathways.
Dr. Ungar said there has been an unmet need for new therapies for SD, noting that the most common treatments are topical antifungals, calcineurin inhibitors such as tacrolimus and pimecrolimus, and topical steroids. “But topical steroids worsen rosacea, and when you have a common comorbid condition, you need to be mindful of that,” he warned. The FDA recently approved topical roflumilast foam, a PDE4 inhibitor that has anti-inflammatory properties, for the treatment of SD. In a phase III clinical trial of 457 patients, 79.5% were clear or almost clear after eight weeks, compared to 58% of those using a placebo.
The pathophysiology of SD and rosacea bear some similarities, Dr. Ungar noted. Both diseases show abnormally high expression of genes related to the Th1 and Th17 immune response pathways, which result in inflammation and skin barrier dysfunction.
“All of the available treatments for papulopustular rosacea are one way or another attacking the disease from an antimicrobial perspective,” Dr. Ungar said. “And so, similar to seborrheic dermatitis, a question we have to ask is whether rosacea is driven by microbial dysregulation or dysbiosis, or is treatment addressing one aspect and missing another part?”
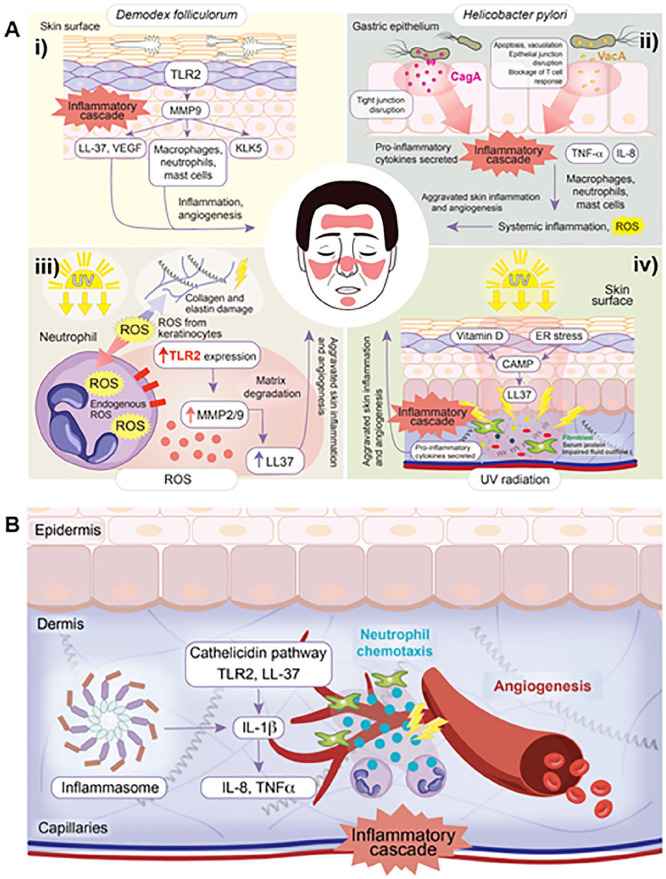
In a study investigating the prevalence of H. pylori in patients with rosacea, participants were compared with age- and sex-matched controls. The prevalence of H. pylori was 88% in rosacea patients and 65% in controls. However, among the H. pylori-positive subjects, there were twice as many rosacea patients with CagA+ strains compared to controls. Interestingly, eradication of the H. pylori infection with a week-long therapy using omeprazole, clarithromycin, and metronidazole resulted in resolution of rosacea symptoms and normalization of the pro-inflammatory cytokines IL-8 and TNF-α. 40 This was corroborated by another study which found that eradication of H. pylori with amoxicillin, metronidazole, and bismuth subcitrate resulted in significant improvements in rosacea symptoms. 41 The use of metronidazole and oral antibiotics, common rosacea treatments, in both of these studies complicates the findings as it is unclear if the resolution of rosacea symptoms is due to eradication of H. pylori or the anti-inflammatory and antioxidative properties of the drugs themselves. Further complicating the potential involvement of H. pylori in rosacea pathogenesis is the results from 2 other independent studies that eradicated H. pylori but observed no improvement in rosacea symptoms.
Once-daily treatment with roflumilast foam 0.3% resulted in significant and clinically meaningful improvements in key signs and symptoms of SD and was well tolerated in patients as young as 9 years of age. Specifically, significantly more roflumilast-treated patients than vehicle-treated patients achieved the primary endpoint, IGA Success at week 8, with 80% of roflumilast-treated patients achieving IGA Success and >50% of patients achieving clearance. The inclusion of adolescent patients was important to demonstrate consistency of efficacy and safety in this age group whose SD onset may be exacerbated with the onset of puberty.
Several possible factors may explain the high level of response to vehicle observed in this study including the therapeutic effect of excipients and moisturizing in patients with SD, which may repair the skin barrier, as well as variability of underlying disease. The water-based foam used for both the roflumilast foam and vehicle foam in this study contains a mild emulsifier commonly used in cosmetic products but not previously used in prescription topical formulations.
Regarding the HMG-CoA reductase inhibitor, statin; it is reported to be effective against many other dermatologic diseases including psoriasis, eczema, graft-versus-host disease, uremic pruritus, vitiligo, and hirsutism17. Also, its topical forms are employed in the treatment of acne, seborrhea, rosacea, and rhinophyma17. With immunomodulatory effects18, its systemic anti-inflammatory action in inflammatory arthritis18 and allergic asthma19 has been demonstrated17. Additionally, statin inhibits the activity of oxidant enzymes20, and up-regulates the activity of antioxidant enzymes17. Statin also has a biphasic effect on angiogenesis in human epidermal microvessel endothelial cells18; low concentrations tend to increase angiogenesis but higher doses induce inhibition of vascular endothelial growth factor synthesis21. Also, statins inhibit the expression and secretion of MMP-1,-2,-3 and -9 from vascular smooth muscle cells and macrophages22, compared with fibrate (no inhibition)23. MMPs play a major role in remodeling the extracellular matrix24,25 and also in the etiopathogenesis of rosacea; so the protective effects of statin on developing rosacea in patients with hyperlipidemia should be considered.
Small intestinal bacterial overgrowth
Multiple studies have associated rosacea with small intestinal bacterial overgrowth (SIBO). A Danish population-based analysis found that rosacea was associated with an increased prevalence of SIBO but not an increased risk of new-onset SIBO diagnosis. A smaller Italian prospective cohort study also found that a significantly higher percentage of patients with rosacea had SIBO at baseline, compared with the control group (41.7% versus 5%). A second Italian prospective cohort study did not find any significant difference in the prevalence of SIBO at baseline between patients with rosacea and controls. The first study used lactulose hydrogen breath test and glucose breath test to verify the presence of SIBO, whereas the second study used the glucose breath test alone.
The association between rosacea and SIBO is additionally supported by several studies that examine the response to SIBO treatment with rifaximin. One prospective cohort study treated rosacea patients with a daily dose of 1,200-mg rifaximin to eradicate SIBO. The investigators found that cutaneous lesions of rosacea significantly improved with successful eradication of SIBO. A second study reported that 46% of rosacea patients treated with rifaximin experienced resolution of or markedly improved rosacea clinical manifestations.
A third prospective cohort study demonstrated that 55% of Italian patients with rosacea experienced normalization of both their SIBO and rosacea clinical manifestations with the same rifaximin regimen. Based on these studies, it appears that there is an association between rosacea and SIBO. Not all patients with rosacea have SIBO and not all SIBO patients have rosacea, and treating SIBO in patients with rosacea does not always lead to resolution or lessening of rosacea signs and symptoms, further demonstrating that SIBO may be one of many contributing factors in the overall pathogenesis of rosacea. It may be worthwhile to consider screening patients with rosacea for the presence of SIBO and eradicating SIBO as a treatment option for rosacea.
Irritable bowel syndrome
Only one study thus far has linked rosacea and irritable bowel syndrome. A population-based analysis in Denmark found that the baseline prevalence of irritable bowel syndrome was significantly higher in Danish patients with rosacea compared with the prevalence in that of controls, with an adjusted hazard ratio of 1.19 to 1.50 for rosacea patients. In addition, patients with rosacea were found to have an increased risk of new-onset irritable bowel syndrome diagnosis. Such association may be underestimated, as dermatologic evaluation of these patients does not usually include a thorough investigation of gastrointestinal symptoms.
The pathophysiology of rosacea involves dysregulation of innate and adaptive immunity, neurovascular changes, chronic inflammation, and, possibly, infections.1 A new pathogenic mechanism was recently suggested after a relationship was observed in a study where 46% of prospective patients with rosacea had small intestinal bacterial overgrowth (SIBO).2 After therapy with rifaximin, a nonabsorbed, gut-active antibiotic, complete resolution of cutaneous lesions in 78% of the patients with SIBO was observed. SIBO may alter immunity and trigger rosacea by increasing tumor necrosis factor-alfa or other cytokines, suppressing interleukin-17, and stimulating the T helper 1-mediated immune response.3 Furthermore, gut bacteria have been shown to mimic immunogens associated with extraintestinal disease (ie, multiple sclerosis).
The aim of this pilot study was to determine the prevalence of SIBO in patients with rosacea seen in a gastroenterology clinic and determine the efficacy of rifaximin in patients with indirect evidence of SIBO (ie, a positive result on lactulose breath test). The study protocol received approval from Sterling Institutional Review Board, Atlanta, Ga. Most patients with rosacea were identified during physical examination by their gastroenterologists before receiving a screening colonoscopy. Rosacea was diagnosed by a dermatologist in 57 cases. Four patients with medicine-refractory ocular rosacea were referred by ophthalmologists. Two cases of rosacea were diagnosed by the investigator. In addition to the ocular cases (3 had facial erythema), 9 had papulopustular and 50 had erythematotelangiectatic rosacea. All patients underwent a lactulose breath test, with a positive test result for SIBO defined as an increase in hydrogen or methane levels greater than 20 ppm from baseline within 90 minutes. Prevalence of SIBO was compared to 2 control groups.
Patients with SIBO received 400 mg of rifaximin 3 times daily for 10 days. Patients completed a self-report questionnaire using a 4-point rosacea improvement scale 10 days after ending rifaximin therapy. A repeated physical examination was performed in 70% of patients treated with rifaximin.
A total of 32 of 63 patients (51%; 6 male and 26 female) with rosacea were given the diagnosis of SIBO compared with 7 of 30 general population control subjects (23%; relative risk, 2.1; 95% confidence interval, 1.1-4.3; P = .02) and 3 of 30 completely healthy control subjects (10%; relative risk, 5.0; 95% confidence interval, 1.7-15.1; P < .001). Of the patients with SIBO, 28 were treated with rifaximin: 46% reported cleared or markedly improved rosacea, 25% reported moderately improved rosacea, and 11% reported mildly improved rosacea. All 4 patients with ocular rosacea and SIBO reported marked improvement. Rosacea was unchanged in 18% of patients. In this study, a subset of patients with rosacea and indirect evidence of SIBO was identified and a significant majority improved after treatment with a nonabsorbable antibiotic. A study screening patients with rosacea in a dermatology clinic using a lactulose breath test for evidence of SIBO and a double-blind clinical study to determine the efficacy of rifaximin in these patients would greatly contribute to an understanding of the potential impact of these findings.
Background: Rosacea is associated with Crohn’s disease, liver disease, chronic pancreatitis, achlorhydria, Helicobacter pylori and recently with idiopathic small intestinal bacterial overgrowth (SIBO). Two publications demonstrated that rifaximin, a non-absorbed, gut-directed antibiotic for SIBO led to improvement in facial rosacea. Ocular manifestations occur in up to 58% of rosacea patients and include dry eyes, foreign body sensation, photosensitivity, eyelid inflammation, neovascularization and corneal ulcers. Methods: Patients who had been diagnosed with ocular rosacea by four ophthalmologists were referred for SIBO testing using the lactulose breath test (LBT). All were refractory to rosacea therapy. An open-label, IRBapproved trial of rifaximin 550 mg/3x/day for 10-14 days was performed in LBT-positive subjects. Ten and twenty days after ending rifaximin, subjects were queried if their eye symptoms had marked, moderate or mild improvement or if they were unchanged.
Results: Twenty four patients (21F/3M), mean age 59 with facial involvement in 4 were tested. The LBT was positive in 9/24 (38%). LBT-positive subjects had chronic gastrointestinal symptoms in 63% vs., 33% in LBTnegative subjects. Rifaximin was prescribed to 9 LBT-positive subjects. Insurance denied the prescription in one subject. One subject was lost was to follow up. Improvement in ocular rosacea symptoms was marked (4), moderate (1) and mild (2).
Conclusions: Rifaximin therapy led to improvement in ocular rosacea in the setting of SIBO. Dysregulation of the innate immune system as a result of gastrointestinal inflammation could lead to an increase in systemic cytokines and microbial antigens/antibodies in the skin and eyelids leading to activation of rosacea.
Dry eye is a disease of the tears and ocular surface. Numerous factors contribute to the onset of the disease, but once dry eye has developed, inflammation of various ocular surface tissues propagates the disease as both cause and consequence of ocular surface damage. Individuals with dry eye suffer from ocular discomfort (dry, gritty feeling; itching; stinging/burning; pain/soreness) and blurred vision. Improvement in these symptoms can be affected by administration of artificial tears, but the relief is transitory as the underlying inflammation persists. Therefore, an agent capable of reducing inflammation and inducing tear secretion should be an effective therapy for dry eye.
The phosphodiesterase 4 (PDE4) enzymes regulate a host of biological processes by degrading the intracellular second messenger cAMP. PDE4 inhibitors have been intensively investigated as anti-inflammatory therapies because increases in cAMP levels are known to attenuate inflammatory responses in multiple cell types. Other agents that increase cAMP have been shown to induce tear secretion. Therefore, PDE4 inhibitors should serve the dual role of reducing inflammation and inducing tear secretion providing an effective treatment for dry eye.
In this letter, we describe our efforts to create a novel, potent series of PDE4 inhibitors with aqueous solubility compatible with topical ocular delivery. Furthermore, we disclose efficacy in an in vivo model for dry eye and an in vivo test for tear secretion.
Having identified a novel series of water soluble PDE4 inhibitors, we sought to demonstrate in vivo efficacy. To explore the anti-inflammatory nature of our compounds, we utilized the rabbit model of lacrimal gland inflammation-induced dry eye, in which corneal staining was used to measure ocular surface health. Of the many new PDE4 inhibitors screened in this model (data not shown), compound 18 looked to be the most promising, so a full dose response study was run. Compound 18 was extremely effective at protecting the eye, equivalent to the corticosteroid dexamethasone from 10 ng/mL to 10 μg/mL. To explore the ability of our compounds to induce tear secretion, we utilized the phenol red thread test in rats. At doses of 10 μg/mL and 100 μg/mL, compound 18 was effective at inducing tear secretion. Thus, compound 18 demonstrates the potential effectiveness of PDE4 inhibitors for the treatment of dry eye.
Following the evaporation of the tear film, activated TRPM8 receptors allow Ca2+ ions to enter the cell [20,21]. The increased intracellular calcium concentration activates calcium-dependent protein kinases (protein kinase C (PKC) and calcium/calmodulin-dependent protein kinase II (CaMKII)). PKC and CaMKII phosphorylate downstream target proteins, resulting in the activation of transcriptional factors (nuclear factors of activated T cells (NFAT) and cAMP response element-binding proteins (CREB)), which enhances the expression of genes that regulate the production and secretion of neuropeptides (substance P and calcitonin gene-related peptide (CGRP)) [20,21]. These neuropeptides stimulate tear production in lacrimal glands. Upon binding to neurokinin-1 and CGRP receptors, substance P and CGRP initiate the activation of cyclic adenosine monophosphate (cAMP) and PLC-driven intracellular signaling cascades within the lacrimal gland cells.
The cAMP pathway stimulates the opening of chloride (Cl-) channels, allowing the secretion of Cl- ions into the lacrimal gland ducts. This is followed by the efflux of sodium (Na+) ions and water, creating an osmotic gradient that drives the secretion of tears. Activated PLC catalyzes the hydrolysis of phosphatidylinositol 4,5-bisphosphate (PIP2) into inositol 1,4,5-trisphosphate (IP3) and diacylglycerol (DAG) [19,20]. IP3 diffuses into the ER of lacrimal gland cells and binds to IP3 receptors, causing the release of Ca2+ ions from intracellular stores. The increase in intracellular calcium concentration activates calcium-activated chloride channels (CaCCs) present on the apical membrane of lacrimal gland cells [20,21]. These channels allow the efflux of chloride ions (Cl-) from the cytoplasm into the lumen of the lacrimal gland ducts. The efflux of chloride ions creates an osmotic gradient, which drives the movement of sodium ions (Na+) and water from the interstitium into the lumen of the ducts through paracellular and transcellular pathways. Along with fluid secretion, the activation of the PLC pathway also stimulates the secretion of electrolytes into the lacrimal gland ducts. The combined effect of fluid and electrolyte secretion in the lacrimal gland results in tear production. Since TRPM8/neuropeptide-dependent activation of cAMP and PLC in lacrimal gland cells is essential for optimal tear production and proper hydration of the ocular surface, any dysfunction of the TRPM8 receptors leads to reduced tear production and causes dryness of the ocular surface.
Approximately half of corneal TRPM8+ neurons express the TRPV1 channel that allows the passage of calcium, sodium, and potassium ions [31]. TRPV1 is highly expressed in corneal and conjunctival TRPM8+ sensory neurons, and in anterior eye samples and trigeminal ganglia of mice and rats with DED [22]. An increased osmolarity of the tear film triggers a conformational change in these TRPV1 channels, leading to their opening. Massive influxes of cations cause disruption to cellular homeostasis [23]. Accordingly, THO-dependent prolonged activation of TRPV1 channels causes tear film instability and compromises the integrity of the epithelial barrier in the eyes, exacerbating DED [23,24]. Also, activation of TRPV1 in human CECs importantly contributes to the development of ocular inflammation in DED patients [32]. TRPV1-dependent increases in the intracellular concentration of calcium, which leads to the activation of mitogen-activated protein kinase (MAPK) and transcriptional factor NF-κB, resulting in an enhanced production of inflammatory cytokines (IL-6 and IL-8) [32]. Additionally, the nociception experienced with DED is a result of TRPV1 activation on the ophthalmic branch of the corneal trigeminal nerve endings [33]. Bearing in mind that a continuous activation of TRPV1 aggravates DED [22,23,24], Benitez-Del-Castillo and colleagues conducted phase I and II pilot clinical trials to test the safety and efficacy of SYL1001 (TRPV1-specific short interfering RNA) in DED patients [34]. Topical administration of SYL1001 significantly extended tear break-up time, prevented THO, improved the disease index score of ocular surfaces, and attenuated conjunctival hyperemia in the eyes of DED patients, without causing any severe side effects [34].
Purpose: Phosphodiesterase type 4 (PDE4) inhibitors prevent catalysis of intracellular cAMP in multiple cell types. With respect to dry eye therapy, relevant consequences of elevated cAMP include anti-inflammatory and pro-secretory effects. Cilomilast is a potent and selective PDE4 inhibitor which inhibits inflammatory cell activation and cytokine secretion. Cilomilast was evaluated for topical ocular efficacy in several models of dry eye disease.
Results: In both the rat and rabbit models of dry eye, cilomilast (BID) provided steroid-equivalent inhibition of corneal staining at concentrations of 0.001 to 0.1% w/v. Topical administration of 0.05% cilomilast normalized tear protein concentrations and tear clearance in sex steroid-deficient rats. Cilomilast significantly increased tear secretion above vehicle from 10 min to 4 hrs after topical administration in normal rats. Topical 0.05% cilomilast (BID) also normalized tear secretion in dry eye rats. Cilomilast inhibited hyperosmolarity-induced TNF secretion in CEPI cells (EC50 = 450 nM).
Conclusions: Topical administration of the anti-inflammatory and pro-secretory selective PDE4 inhibitor cilomilast suppressed corneal staining and normalized tear secretion, clearance, and protein concentration in animal models of dry eye. Pro-secretory effects of cilomilast did not exhibit tachyphylaxis. Anti-inflammatory efficacy was equivalent to dexamethasone. These data support the utility of selective PDE4 inhibitors such as cilomilast in the topical treatment of dry eye.
We investigated the effect of cilomilast on several well-described measures of ocular surface inflammation: proinflammatory cytokine expression and APC infiltration. Dexamethasone was chosen as the comparative treatment because its therapeutic efficacy has been demonstrated in numerous DED experiments.9 The proinflammatory cytokines IL-1α, IL-1β, and TNF-α are elevated in the tears and ocular surface of DED patients.20,28 Topical cilomilast significantly reduced the corneal expression of TNF-α and the conjunctival expression of IL-1α, IL-1β, and TNF-α. These cytokines are produced in large quantities by leukocytes, including APCs such as dendritic cells.29 These cytokines are also produced by corneal and conjunctival epithelium.30,31 Infiltration of the cornea by APCs has been described in both experimental and clinical DED.20,32 APC enumeration was performed, revealing that cilomilast significantly decreased the presence of CD11b+ APCs in the peripheral and central cornea. These findings are consistent with previous reports indicating that PDE4 inhibition reduces the ability of APCs to produce proinflammatory cytokines (e.g., TNF-α) and promote immune activity.29
We also investigated the effect of cilomilast treatment on IL-17–associated immune responses in DED. For this experiment, the DED induction phase was extended to 6 days to ensure that a robust adaptive immune response was generated. Infiltration of the conjunctiva by pathogenic T cells is a universal feature of DED.33 Th17 cells are a recently discovered population of T cells that have been implicated in the immunopathogenesis of DED.3,6–8 IL-6 and IL-23 promote the differentiation and expansion of Th17 cells.34,35 IL-17, the signature cytokine of Th17 cells, promotes DED by disrupting the corneal epithelial barrier following desiccating stress.
Cyclosporine was chosen as the comparative treatment because cyclosporine’s method of action specifically targets T cells, including Th17 cells.36 Treatment with topical cilomilast significantly reduced the conjunctival expression of IL-6, IL-23, and IL-17, and the draining lymph node expression of IL-23 and IL-17. These findings indicate that treatment with topical cilomilast reduces the IL-17–associated immunity.
There was a reduction of 10% to 20% in CFS score in the vehicle-treated compared with the DED-untreated eyes. The vehicle effect was also seen on the infiltration of CD11b+ cells in the cornea and CD45+IL17+ cells in the conjunctiva. This is perhaps due to the lubricating effect of the vehicle on the ocular surface. Lower expression of IL-23 in the draining lymph nodes might be due to the reduced migration of CD11b+ cells to the draining lymph nodes.
Importantly, treatment with topical cilomilast consistently reduced corneal epitheliopathy scores by approximately 40% from baseline. Moreover, topical cilomilast was significantly more effective than its associated vehicle at reversing ocular surface damage, suggesting that the beneficial effects of cilomilast treatment are not solely attributable to lubrication of the ocular surface. Topical application of the anti-inflammatory medications dexamethasone and cyclosporine produced CFS reductions that were comparable to those produced by the topical application of cilomilast. In summary, our findings indicate that topical cilomilast ameliorates DED as determined by clinical and inflammatory measures. The therapeutic efficacy of cilomilast was comparable or superior to that of dexamethasone and cyclosporine. These findings suggest that topical cilomilast may be an effective therapeutic modality for clinical DED. Additional investigations will be required to determine the optimal dosage and duration of cilomilast treatment.
Patients with dry eye disease (DED) often exhibit neurological abnormalities and may even suffer from neuropathic pain and pain-related anxiety or depression. However, addressing nerve abnormalities in DED remains a formidable challenge, as current therapies fail to halt disease progression. Our study found that activating α-7 nicotinic acetylcholine receptor (α7nAChR), a pivotal regulator in the anti-inflammatory pathway connecting the nervous and immune systems, effectively restores corneal epithelium integrity and enhances nerve sensitivity in DED, pointing to its promising therapeutic potential. Furthermore, we have revealed that α7nAChR stimulates genes involved in immune-mediated inflammatory progression and neuroregulation, inhibits the expression of transient receptor potential vanilloid-1 (TRPV1), reinstates corneal nerve density, and alleviates anxiety-like behaviors associated with severe DED by downregulating the proportion of CD86+ M1 macrophages (pro-inflammatory phenotypes). In summary, our findings underscore the activation of α7nAChR as a pioneering therapeutic approach for preserving corneal nerves balance and controlling inflammation in DED.