I made this rough sketch over four popular compounds. Have I missed some interesting risk or reward parameter to include or some other interesting comparison data? All feedback is welcome ![]()
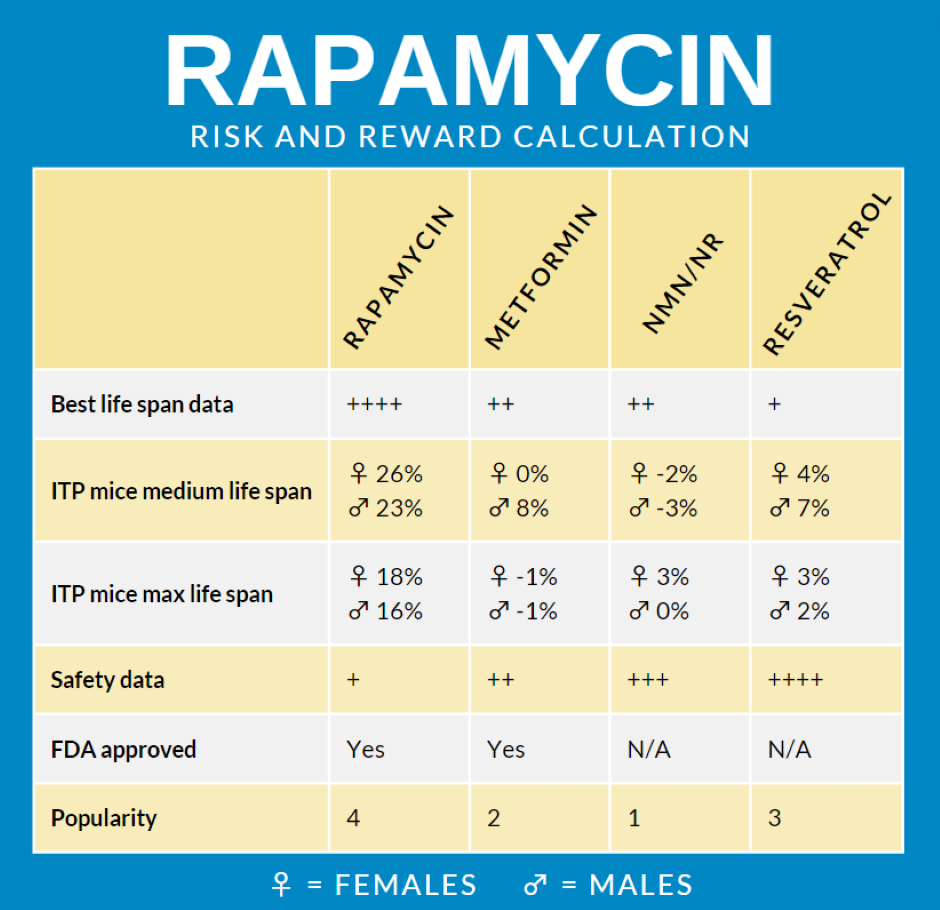
Just my personal opinion: Based on data I have read, I don’t think NMN or resveratrol deserve to be included in this list as having positive benefits.
This article is actually of summary of many that I have read and addresses both NMN and resveratrol:
A ‘Fountain Of Youth’ Pill? Sure, If You’re A Mouse. | Kaiser Health News
4 Likes
The reason why I have added NMN and Resveratrol to the list is because of their popularity. If I would pick four compounds that people talk most about then it would be these four. So it’s very interesting to make a risk and reward comparison between them. What four compounds do you feel are the most popular ones people talk much about in the longevity field?
1 Like
based on this list rapamycin is a no brainer, isn’t it?
2 Likes
Yes, the thing that make people not taking it is because of the safety risks. So the PEARL trial which will be completed next year will be a big contribution to the field. After that I think the rapamycin movement will really take off.
1 Like
I would argue that since metformin and rapamycin are FDA approved 20+ years ago, and used by millions of people, the safety data is actually much better (more data points) than the other compounds.
5 Likes
Is there any real serious side effects with taking NAD boosters or Resveratrol that we know about in humans? I agree that both metformin and rapamycin have decades of historical usage which is good and that they are FDA approved. But the big problem with rapamycin is the immunosuppressive part of it. The field is starting to change towards that it’s more a immunomodulator which means that it can improve or suppress the immune system depending on dose regime. We “know” that but we need a study showing that. Joan Mannicks study is an good indication in the right direction but we should not forget her studies was on rapalog and not rapamycin. The PEARL trial is now testing a dose regime and the “same” drug as the longevity community uses. That is an important safety step in the right direction which is based on science and not anecdotal evidence. We know what the result will most likely be but other people need to see this data to be convinced of the safety.
Like when I talked to a physician last week. She asked me if I’m not concerned about the immunosuppression risk of rapamycin. I smiled and told her what we know today and that I’m not affraid of that. But they need the data and the PEARL trial will make it possible for us to easy give it to them ![]()
Yes, perhaps to be as accurate as possible the “safety data” might be better labeled as “potential side effects” or something like that.
1 Like
I like the idea of adding another parameter for pointing out the risk some how. “Potential side effects” is little bit to general because you could for example get different mild side effects which are not any risk. What do you think about “Unsafe side effects”?
I think thats too scary and misleading because most people don’t get the “unsafe” side effects of rapamycin.
I’m not sure what the right wording is… you want something that conveys that in general people are more likely to see side effects with rapamycin than probably NMN or resveratrol, but most of these side effects are minor.
Perhaps something like “frequency of side effects”. or Side Effect Profile (with NMN and Res. being “low” and rapamycin being “moderate” or “dose dependent”?
1 Like
Also - the “popularity” line is potentially confusing. I’m not sure, on the face of it, if a popularity of 4 means its more popular (my first thought) or if you are ranking them from 1 to 4 with 1 being the most popular, and 4 being least popular. There needs to be more clarity on that. For someone new to longevity compounds they would have no idea.
Perhaps something like Number of Users, with rough estimates of 10K for Rapa, 100K+ Metformin and Millions for NMN and Resveratrol?
1 Like
Yes, unsafe is little bit scary. What about “risk” (low, medium and high)? But even that is not good. Rapamycin is not a high risk. It’s more medium risk? And the other ones could be set to low risk?
Very good that you point out the popularity. I have an idea of improvement there and it’s to use google trend from 2004-2022 and show the graph in that box. Here are for example trending for metformin
https://trends.google.com/trends/explore?date=all&q=metformin
https://trends.google.com/trends/explore?date=all&q=rapamycin
I like the google trends links. I would just set it to the past 5 years instead of past 20 years. LIke this:
https://trends.google.com/trends/explore?date=today%205-y&q=NMN
Very good suggestion in narrowing it down to 5 years!
Maybe… but I still think its deceiving since at low weekly doses the side effects for rapamycin are generally not much different than for NMN (other than the occasional canker sore).
How about: Side Effects: Rapa: Dose Dependent, Metformin: Low, NMN: low, Res: Low
1 Like
Not perfect with dose dependent either. Because if you take to high doses of some other compound then most likely you will get more side effects. I want to highlight some how the common view which researchers and physicians have about rapamycin and it’s that it’s not risk free. This is also something people like Alan Green, Matt Kaeberlein and Peter Attia also point out. So some how this must be put in as an parameter. If it would not be any serious risk at all then the rapamycin movement would have taken off already. I would say this is the parameter which holds the a feet on the brake because people are scared of what can happen. So I understand their worry and their wish for more data before they start taking rapamycin and/or prescribe it as off label for longevity.
Let’s see what a good night sleep can generate for ideas in the topic ![]() If someone else has any good suggestions let us now
If someone else has any good suggestions let us now ![]()
1 Like
I disagree. Perception is what matters, not reality. Asprin is deadly, but the perception is its benign: A nationwide study of mortality associated with hospital admission due to severe gastrointestinal events and those associated with nonsteroidal antiinflammatory drug use - PubMed
Death rate attributed to NSAID/aspirin use was between 21.0 and 24.8 cases/million people, respectively, or 15.3 deaths/100,000 NSAID/aspirin users. Up to one-third of all NSAID/aspirin deaths can be attributed to low-dose aspirin use.
According to wikipedia, aspirin has been used (either in its precursor form - Willow bark - or current tablet form) for 2400 years by humans and is generally assumed to be safe, but here is a 2010 conclusion on aspirin: Critical Overview on the Benefits and Harms of Aspirin - PMC
Conclusions
This overview of recently published meta-analyses suggests that aspirin therapy has significant benefits in a variety of clinical settings, but there are still uncertainties that will require more research. Current evidence suggests that aspirin is beneficial for secondary prevention for cardiovascular disease, primary prevention of pre-eclampsia, and secondary prevention of colorectal adenomas. However, use of aspirin in primary prevention of cardiovascular disease, or in patients with diabetes mellitus, or in those with peripheral vascular disease is not supported by the current evidence. It is also clear that aspirin has considerable potential for harm in patients undergoing surgical procedures. The benefits of aspirin use must be weighed clinically against the risk of adverse events such as gastrointestinal and intracranial bleeding.
As Matt Kaeberlein has said, rapamycin is not popular yet, because of
“Bad (undeserved) reputation, Lack of profit motive (generic drug), Bureaucratic barriers”
and your infographic, if you highlight or focus on the perceived risk and worse case scenarios, will further stigmatize the medication. You could make the case that Aspirin is deadly and shouldn’t be sold, but that wouldn’t be helpful for most people (but of course, aspirin has had a huge company Bayer, marketing aspirin for decades). Similar situation with rapamycin… but without the marketing.
See this thread/discussion below:
And this post:
People have tried to overdose on rapamycin, taking 103mg at once, and suffered no serious negative effects… so please, don’t make rapamycin out to be more risky than it actually is:
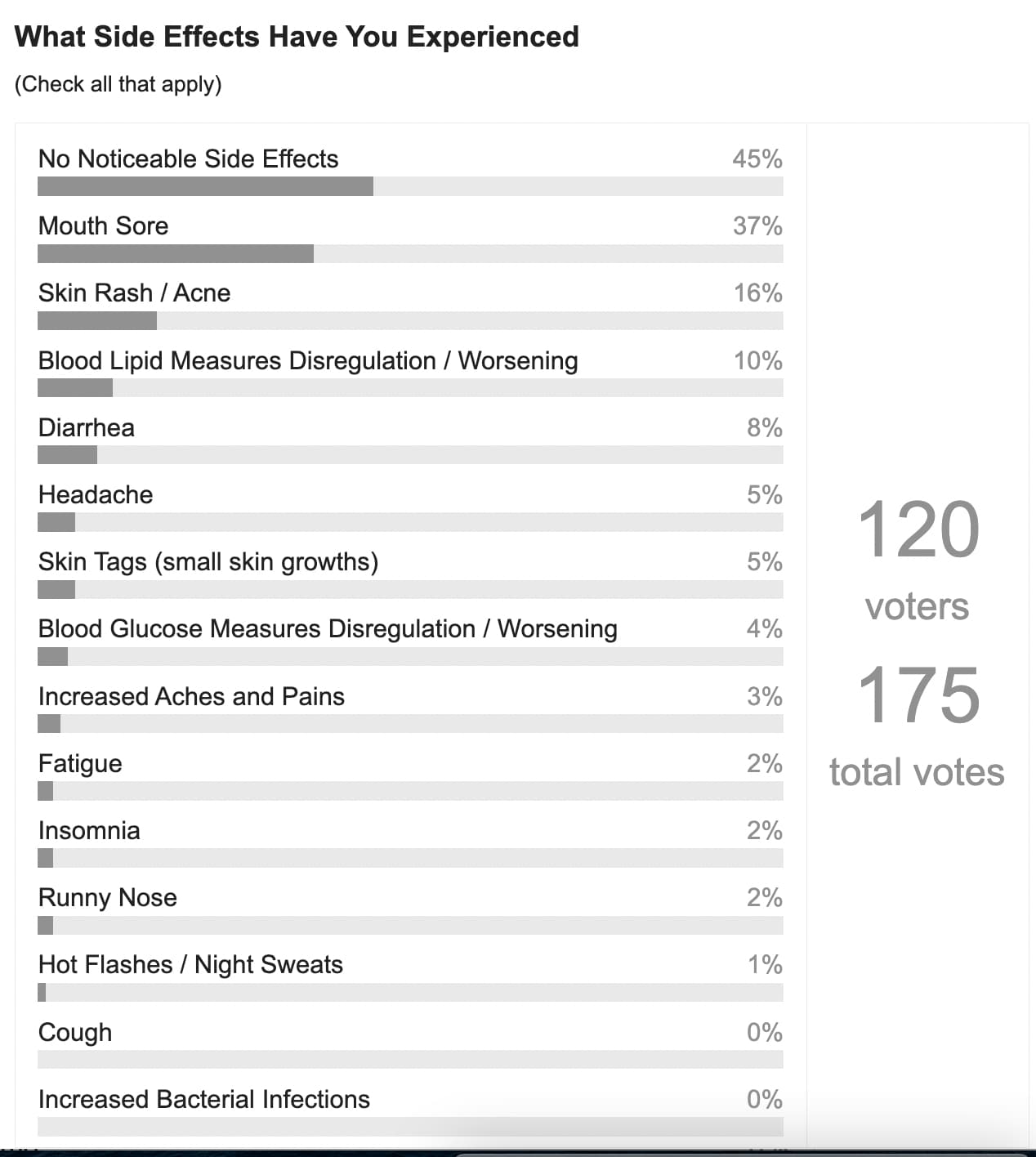
As we’ve seen reported by the users here, side effects are mostly minor and temporary and go away without treatment or with cessation. I think you’d likely get a side effect profile that is similar if you compared “exercise” and “periodic alcohol consumption” with the rapamycin side effects - yet rapamycin has a demonstrated effect of lengthening lifespans in all organisms tested by 15% to 25% typically.
Humans (generally) have great difficulty in risk/reward tradeoffs and calculations, and the simplistic “do no harm” approach of the modern medicine establishment results in significant harm to vast segments of the population (I believe), in terms of avoiding preventative approaches like rapamycin.
And, its important to put things in perspective… people recommend / or participate in things like exercise and alcohol consumption, both of which likely have much higher side effect profiles than rapamycin:
Also - some other observations:
5 Likes
The best thing is when perception goes hand in hand with reality. Both you and me have a perception that the longevity dose regime is most likely safe. We have different data which we can back that up but we don’t have the big trials behind to back this up. To really start convincing other more conservative people you really need more data. Most people are not pioneers like you and me. They are not either very conservative. They are something in the middle. If we would stop all the science studies on rapamycin today I can promise you that rapamycin would never be a mainstream longevity compound. It would be only used by people who have read the literature and has the courage to self experiment. So we need more safety data on the longevity dose regime and that data will eventually convince more than just pioneers.
He also recently pointed out the real risks with rapamycin. Even if it’s “slight” the risks are there:
If you remember the Fitbit you had when you got rashes from it. It was most likely a bacterial infection problem there I would say. So there exists things we don’t really understand. What would happen if you would have continued using the fitbit year by year and ignored those signals?
This makes me also think of one thing that the metformin researcher Nir Barzilai said in an Peter Attia interview when Peter asked him why he had choosen to study metformin and not rapamycin in the TAME trial.
“We don’t want to kill anybody on the road. With rapamycin we won’t be sure. … So we have to play it safe.”
Source: #35 – Nir Barzilai, M.D.: How to tame aging - YouTube
I believe that the rapamycin is the best compound out there when it comes to longevity and I really hope that one day more people will be able to take it and we have more data on it. My goal is for example to invest around 30000 dollars to my N=1 rapamycin study. I don’t want to stimatize the drug but I don’t want to hide things that are uncertain. It’s very interesting to get anecdotal data here on this site but it’s important to know that this data has many limitation. For example, how many of the people who have got serious side effects are included in the statistics that has been gathered? The people who are included in the statistics are probably also quite healthy people. How will rapamycin work on unhealthy persons? Would we see another side effect profile? There are many questions. And we are pioneers in the area.
This reminds me also about some recent posts that I have seen.
“I had one of the worse side effects. After 2nd week of 3mg rapamycin, I developed a recurrent infection that required surgery to fix
. The risk is real, even if it is rare.”
Source: https://twitter.com/hongwingl/status/1595545870556024833
“Though I’ve been taking it for less than 2 months I have already had two serious bacterial infections that require antibiotics and have had chronic effects on my life”
Source: Too many bacterial infections have to stop, low WBC - #2 by KarlT
“I had a bacterial infection while taking Rapamycin a few weeks ago. I had to stop the Rapamycin and take antibiotics.”
Too many bacterial infections have to stop, low WBC - #22 by DeStrider
David Sinclair: “I did try it (rapamycin) once. I caught a cold for the first time in years and so you know I’m little bit warried about it. But I think the science behind it is really strong.”
Source: Rapamycin | Dr David Sinclair Interview Clips - YouTube
“I personally got a cold after starting Rapa…5mgs (weekly)”
Source: Rapamycin | Facebook
“Rapamycin induced inflammatory syndrome is a very serious risk of this drug. The husband of one of the members in this group ended up in the ER in serious pain as a result. There are many people taking the drug, including professional geroscientists, who clearly do not understand this syndrome and have no idea that it can occur.”
Source: Rapamycin | Facebook
I’m not worried about the side effects when I start but there are risks out there even on longevity dose regimes and when people ease up the dose. We don’t fully understand everything yet.
1 Like
How about adding a line for “Fasting” that clearly point out its potentially riskier than rapamycin?
3 Likes
That extended fasting for several days or calorie restriction suppresses immune system is well known I would say. The interesting thing here is that this study shows bigger suppression than rapamycin. It would be good with studies in humans where a comparision is made between rapamycin and extended fasting/calorie restriction. When it comes to short term fasting like the classic 16:8 fasting (8 hour eating window every day) I have not seen any data on that it’s suppresses immune system. If someone finds out some study here let me know. Would be very interesting to read that.
Interesting suggestion to add a new column with fasting/CR to the image but I wonder if the image would be little bit strange when it focuses on the four most popular compounds. But I’m working on another image already which will focus on the four best longevity interventions and there CR and rapamycin is included. Or how would I solve it in a good way in this? All suggestions are welcome ![]()
Here are some comments I had on Matts tweet
1 Like