Interesting! Maybe that’s why my nebivolol seemingly had no effect in protecting against the two episodes of afib I’ve had over the last several years (both happened after chugging a cold fruit smoothie).
Have you come across the topic of psychological stress-induced myocardial ischemia in your hypertension readings? It always seemed like a beta blocker would be most protective against this “fight or flight” response from a stressful event that can trigger a MI, but when last I checked (several years ago), I couldn’t find much data and what I did find never seemed to mention beta blockers.
I’ve never checked this. I assume it’s hard to measure. In clinical trials and medical records, can we distinguish stress-induced MI from other myocardial ischemia? If not: we cannot know which drug works best for this.
Oh it’s definitely a thing and is measurable, and puts people prone to this at much higher risk of cardiac events. I’ll look into the literature later today to see what I can dig up.
A positive for telmisartan seems also to be weight/fat loss. I’m experiencing that with my regimen and think my high dose of telmisartan is helping (though I’m also taking other things like rapa and jardiance that many feel help in the weight/fat as well)
I wonder if its affects on body weight/fat are in a dose dependent manner? I’m taking the 80 mg. Will be interesting to observe my body after a few months more on it as ive really just started it recently. (though I’m also taking other substances that could be decreasing the body weight/fat)
I think the idea behind PSIMI is to subject patients to a psychologically stressful stimulus and assess for signs of mild cardiac ischemia. Those who show signs of ischemia from psychological stress (vs those who don’t, while carefully controlling for other risk factors) have a much higher risk of future cardiovascular events. Thus, meds which block this effect should significantly reduce future risk in those who experience PSIMI. I’m curious if they’ve yet done studies with different classes of BP meds to assess which may be best for this use.
Edit: it’s referred to as “Mental Stress Induced Myocardial Ischemia” aka MSIMI. Here’s a recent review, but not a lot of answers yet.
It’s a tough call. I’ve never had episodes of afib other than those two times after chugging cold smoothies (and I know immediately when I’m in afib, unlike some who can’t tell), so is it worth being on an anticoagulent med for the rest of my life, which also carries its own risks? There aren’t any anticoag outcome studies in the subgroup of patients who only get afib from drinking cold drinks too fast. I do plan to ask my cardiologist next time I see him if it’s worth wearing a portable cardiac monitor for a month to see if I ever have any brief episodes of afib during sleep, for instance. I wore a FitBit for several months with afib detection and never got any notifications.
I don’t know anything about this but you never know whether what the cardiologists etc are saying is medicine 2.0 or 3.0. If it’s the same case as for statins or similar drugs, that is.
If I search for studies on apixaban I found this:
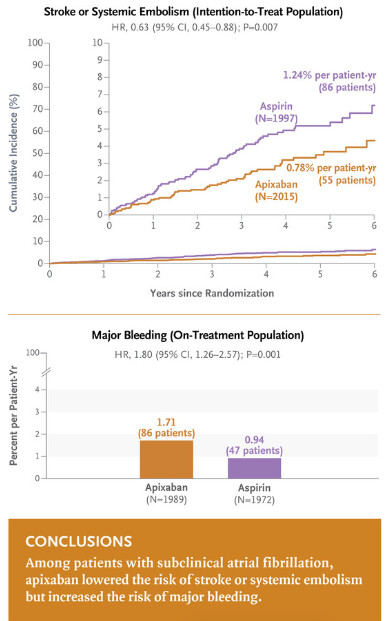
Apixaban for Stroke Prevention in Subclinical Atrial Fibrillation
We included 4012 patients with a mean (±SD) age of 76.8±7.6 years and a mean CHA2DS2-VASc score of 3.9±1.1 (scores range from 0 to 9, with higher scores indicating a higher risk of stroke); 36.1% of the patients were women. After a mean follow-up of 3.5±1.8 years, stroke or systemic embolism occurred in 55 patients in the apixaban group (0.78% per patient-year) and in 86 patients in the aspirin group (1.24% per patient-year) (hazard ratio, 0.63; 95% confidence interval [CI], 0.45 to 0.88; P=0.007). In the on-treatment population, the rate of major bleeding was 1.71% per patient-year in the apixaban group and 0.94% per patient-year in the aspirin group (hazard ratio, 1.80; 95% CI, 1.26 to 2.57; P=0.001). Fatal bleeding occurred in 5 patients in the apixaban group and 8 patients in the aspirin group.
Very interesting! That’s a newer paper I hadn’t seen and wasn’t out when last I discussed this with my cardiologist. I’ll make sure to bring it up and revisit it, thanks. I already take clopidogrel (Plavix) for CVD risk reduction (since I can’t tolerate even low dose aspirin), so adding an anticoagulent to Plavix would REALLY heighten bleeding risk, and I doubt swapping the Plavix for Eliquis would be a good idea because then I wouldn’t have the antiplatelet effect for heart attack prevention.
In the studies I posted about weight gain, they used 40 mg. However, for the effects on insulin and adiponectin 80 mg be even more potent, so it could be the same for body weight?
Relationship between Telmisartan Dose and Glycaemic Control in Japanese Patients with Type 2 Diabetes Mellitus and Hypertension 2012: “When patients were classified into two groups by telmisartan dose (20 vs ≥40 mg/day), there was no significant correlation between baseline HbA1c and change in HbA1c levels over time in the 20 mg/day group. However, in patients treated with ≥40 mg/day of telmisartan, baseline HbA1c was negatively correlated with the change in HbA1c at 6 months. […] Our results suggest that telmisartan influences glycaemic control in a dose-dependent manner; doses ≥40 mg/day may be needed to improve glycaemic control.”
Systematic review of the effect of telmisartan on insulin sensitivity in hypertensive patients with insulin resistance or diabetes 2011: “The available evidence suggests a beneficial effect of telmisartan in improving insulin sensitivity in hypertensive patients with insulin resistance or diabetes as demonstrated by the decrease in FPG and increase in adiponectin levels. The effect in decreasing FPG was greater with 80 mg dose than with the 40 mg dose. FPI and insulin resistance may be improved with 80 mg of telmisartan.”
I just noticed that "Food slightly reduces the bioavailability of telmisartan, with a reduction in the area under the plasma concentration-time curve (AUC) of about 6% with the 40 mg tablet and about 20% after a 160 mg dose" (per FDA). 6% is not a massive difference, but I was taking telmisartan 40 mg just before my meals; from now I’ll try to take it two hours after dinner to maximize absorption.
Telmisartan (TMN), an angiotensin receptor blocker (ARB) drug, is being considered as an alternative therapy for Alzheimer’s disease (ALZ). However, when taken orally, its low water solubility leads to a low bioavailability and brain concentration. To overcome this problem, TMN was formulated as nanocrystals (NC), then incorporated into dissolving microneedles (DMN) to enhance drug delivery to the brain via the trigeminal route on the face.
Nevertheless, some questions remain unsolved and require further research in our view:
What is the contribution of Hcy in the global cardiovascular risk (fraction of attributable risk of Hcy), and is it worth to add this variable in the pre-existing CVR calculators?
How to manage the factors influencing Hcy levels in the long term?
Are the findings replicable in other CV diseases and other populations?
Further research seems warranted to close the current debates and precise the place of Hcy in the CVR assessment.
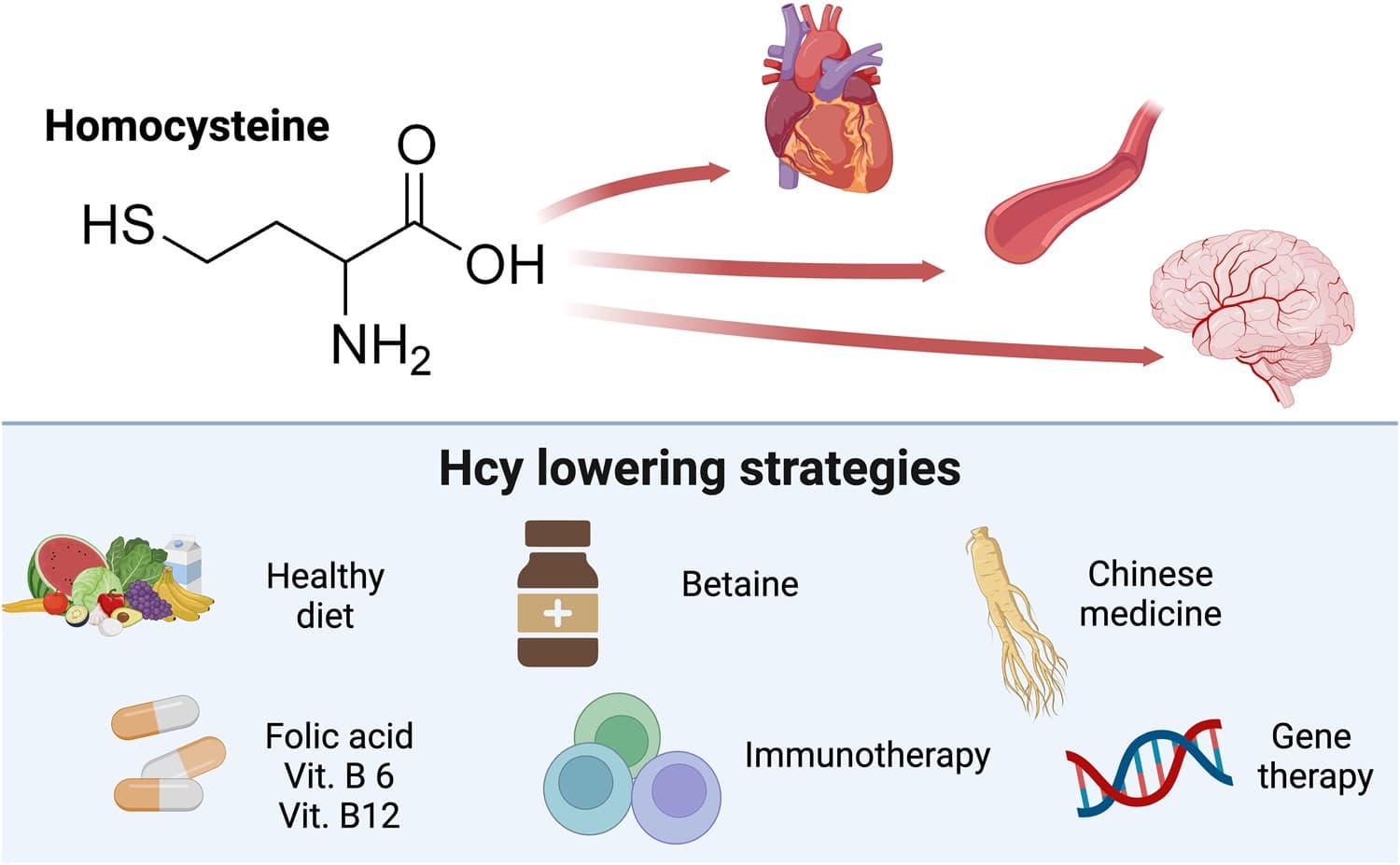
Generally, a plasma Hcy level higher than 10 or 15 μmol/L has been defined as hyperhomocysteinemia (HHcy). An individual with essential hypertension complicated with HHcy is considered to have H-type hypertension (HTH). Currently, HHcy is considered a novel independent risk factor for various cardiovascular diseases.
From a clinical perspective, Hcy levels could therefore not only represent a useful marker of arterial HMOD but also potentially serve to guide the choice of the most appropriate first-line RAAS blocking antihypertensive regimen, that is, ACEi or ARB, the latter being the preferred choice in the context of elevated Hcy levels above 10 µmol/L. Clearly, future studies are needed to investigate whether indeed these theoretical considerations hold true in prospective longitudinal studies and whether Hcy levels may influence the potency of antihypertensive therapy with ACEi vs ARBs in regard to lowering BP and preventing HMOD.
I was excited about the homocysteine theory, so I bought the article. It’s garbage. (No comment on the fact that it comes from the 3rd poorest Chinese province…) It concludes that “Moreover, the curative effect may be improved if traditional Chinese medicine can be administered at the same time.” based on “Compound prescriptions such as Huanglian Wendan Decoction or Erchen Decoction, Shenxiong Glucose, Compound Danshen Dropping Pills, Breviscapine and Banxia Baizhu Tianma Decoction, Tianma Gouteng Decoction, and Qiju Dihuang Pill have certain effects on controlling BP and lowering Hcy levels.” The paper also says that “cholesterol decreasing or lipid-lowering drugs” increase Hcy levels but somehow “atorvastatin calcium tablets” decrease it. Of course, they don’t cite sources, nor do they explain the contradiction.
Worse: they mostly cite literature confirming their thesis and they don’t mention that most Mendelian randomization studies and meta-reviews of clinical trials did not find a significant causal effect of homocysteine-lowering interventions for BP: