wow, and I will be 25mg jardiance, 600mg acarbose, and working my way to 4mg reta or higher, my vials are in the mail - we’ll see how close this gets to too low or how I need to adjust if it is
1 Like
Yes, a lot of people seem to have the plateau issue, and what some people do (after they have reached max dose) they stop taking GLP1’s for a while (4-6 weeks) and then start again somewhere mid range, i.e. 4mg as opposed to starting 2mg and they seem to start losing again.
I am curious to know what do you think of this, and have you encountered it from your experience with your clients?
I also have heard people having success in breaking the stall by introducing small doses of Cagri in addition to GLP1 (which you rightly pointed it out on an earlier post).
1 Like
Used Gemini to graph the results of the Phase 1 and 2 plus top line results of Phase 3 studies:
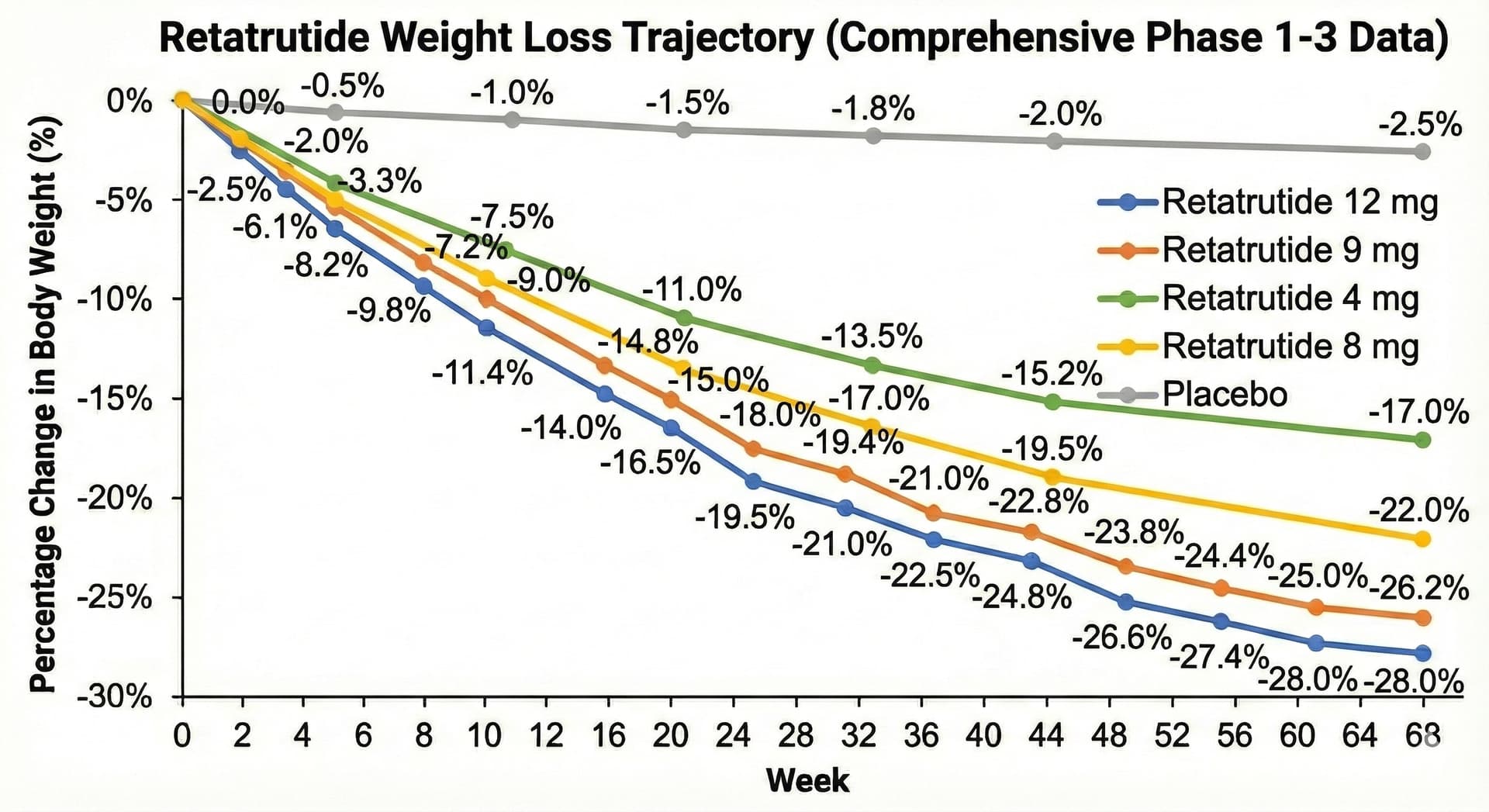
I’d guess loss continues until about 32% average loss at about 100 weeks at the 12mg dose for those whose initial BMI (likely <35 BMI) allows for that degree of loss.
3 Likes
I’m skeptical of the “receptor reset” theory. My review of the research along with a personal n=1 experience is that going off Reta for 6 weeks then returning to same dose (slowly treating up) results in same weight for same given dose. While there is an intuitive sense for receptors adapting to medication, that is not the case for all or even most receptors or medications.
Some add Cagri though its side effects are significant for many. Plus its pending approval with smaller study data available compared with Reta for example. Fortunately my case only requires Reta to reach health weight.
4 Likes
Thanks for the info @zebit0 very informative. Interesting jump in percentage (from the graph) from 8mg to 9mg and then a smaller % weight loss difference from the bigger jump 9-12mg. At 68 weeks the weight loss percentages are 22%, 26,2%, 28% respectively which makes me think the best or more economical dose is 9mg.
My experience has been that on Tirze I do stall/plateau at about 12mg and then I don’t seem to lose anymore??? I only tried RETA about a year ago and don’t have enough n=1 data on it as I swithched early on to Tirze (for the fact that Tirze was FDA approved, and RETA not yet). I do have a good supply of RETA and intend to try it again once I finish the current Vial of Tirze (still trying to lose about 10-15lbs which have proven hard to do on Tirze).
1 Like
You make valid points, but I’m not too concerned. I was born skinny, and at 128, I am approaching the weight I had in high school. It’s easy to put on superfluous pounds, but too much is as bad as too little. Besides, my GFR went up six points in the last two months, a result I was looking for.
2 Likes
I have been experimenting with retatrutide for roughly a year now.
The weight loss does seem to plateau after a while — I’ve lost some body fat but am still in the 10-15% range.
It seems to act as a cholesterol drug for me. Shattered my LDL and Apo-B from 120/80 to 50/50 respectively.
However, the side effect of higher RHR continues. I run at 75 bpm instead of 60 now. That’s the only part that concerns me.
So far I continue to use it. I use fairly high doses (around 10mg once weekly).
3 Likes
Wow, that is certainly a huge drop considering it is not even supposed to have much of an effect on lipids (maybe a small one). Are you on any other lipid lowering drugs? (i.e. statins, and/or ezetimibe)
Reta did that by itself, no other cholesterol drugs.
It’s really quite remarkable.
2 Likes
In 2 years I’ve never had a client “stall” when on the right dose escalation and working on their lifestyle.
Yes, I’ve had people “plateau” until the dose was increased. No stopping, no Cagri, just increase the dose. People expect this to be magic but it’s not. All the results in the clinical trials were at MAX dose over 3 to 5 years. If people expect to be an exception, or don’t understand it is not magic, they may be disappointed. That’s not to say that a LOT of people will achieve their weight loss goal at much lower doses, it just doesn’t work that way 100% of the time.
The response varies widely. I maintain easily at 2.5mg, lost 55lb on 3.5mg over 11 months, many of our clients get results in the 4mg to 8mg range. very few go over 9mg per week
I think “coaching” makes a difference in managing expectations and providing individual support helps get people to understand their personal journey as opposed to trying to follow the social media herd.
I only have 2 people at max dose but they are heavy drinkers, they do not want to change their lifestyle and that is the problem with any weight loss regimen. If lifestyle is not taken into account there is not much that can be done to help those who choose not to change. They have both lost significant weigh but want to lose more without making any changes to their lifestyle.
I do offer Cagri, typically for those who want a more robust appetite suppression i,e, “food noise”. I’ve not had to use it for anything else. I have personally added it to help control my munchies in the evening after our nightly THC drops ![]()
1 Like
8 v 9mg may be from a higher starting BMI in Phase 3.
Here’s what I ended up with after some discussion with Gemini about the 8mg vs 9mg disproportionate variation between Phase 2 and 3:
Assuming the knee pain relief was the same or close between 8mg (Phase 2) and 9mg (phase 3) doses, the 9 mg result appears disproportionately better than the 8 mg (Phase 2) result because:
- *The Patients were Different: The Phase 3 cohort had Class III obesity (BMI 40.4), a phenotype that biologically allows for more profound initial weight reduction via glucagon-mediated lipolysis than the Class II phenotype in Phase 2 (BMI 37.2)
- The Delivery was Better: The 6 mg bridge dose in the Phase 3 protocol prevented the “tolerability shock” of the Phase 2 protocol, ensuring higher quality adherence and consistent drug exposure. Phase 2 dosing was 4 mg → 8 mg, but Phase 3 has a bridge dose from 4 mg → 6 mg → 9 mg. This may have improved tolerability and reduced drop outs of strong responders.
Summary from Gemini:
Retatrutide 8mg vs. 9mg: Explaining the Efficacy Gap
The disproportionate efficacy observed in the Phase 3 (9mg) cohort compared to Phase 2 (8mg) is primarily driven by structural differences in patient phenotype and dosing mechanics, rather than the minor 1mg dose increment.
- Baseline Adiposity (The “Glucagon Reservoir”)
The most significant variable is the baseline phenotype. Phase 2 participants averaged 107.5 kg (BMI ~37), while Phase 3 participants were significantly heavier at 112.7 kg (BMI 40.4, Class III Obesity). Retatrutide’s glucagon agonist component drives energy expenditure; £a higher baseline fat mass provides a larger substrate for this lipolysis.* The Phase 3 cohort effectively had “more fuel to burn,” allowing the drug to sustain a steeper negative slope for a longer duration before metabolic adaptation occurred. - Titration Optimization (Dose Intensity)
Phase 2 utilized an aggressive “doubling” protocol (4mg → 8mg), which triggered a “tolerability shock” and high rates of gastrointestinal distress. This likely led to inconsistent dosing or “aversion-driven” restriction. Phase 3 introduced a crucial bridge dose (4mg → 6mg → 9mg). This smoothed receptor desensitization, ensuring higher “dose intensity” and quality adherence. - Selection Bias
Unlike Phase 2, Phase 3 dropouts were uniquely correlated with “perceived excessive weight loss.” The final data (-26.4%) reflects a “survivor” cohort of hyper-responders, whereas Phase 2 retained a broader mix of responders.
Conclusion
The superior 9mg result is an artifact of treating a heavier, more responsive population with a pharmacokinetically optimized dosing schedule.
People Are Already Taking This Unapproved New Weight-Loss Drug
via Wired
The article describes one individual’s experience and their involvement in setting up a peptide supplier.
Terry was so impressed that he moved into the grey-market pharmaceutical biz himself, ordering APIs from Chinese manufacturers, and selling them—clearly marked as “research chemicals”—through his website, Compound Sciences, based out of Utah.
Anyone have experience with tis supplier?
This is an important aspect of being successful with GLP1’s
I have a few clients who want the weight gone NOW!
And that is a challenge to help them understand it’s a journey that requires thoughtful dosing to ensure success. I try to get people to understand the scale is their friend now and the data they get from the scale is what determines their dose ramp (up or down). Very few are non-compliant but there are the outliers who don’t seem to be able to follow a simple, rational protocol.
This is probably why clinics don’t do it this way, they ramp up as fast as they can to get a result as quickly as they can so they can justify that process and cost. I have a few people who went through that and had bad side effects and dropped out. They came to us through referrals and they are now successful on their journey.
1 Like
No, because they are about 300% higher than everyone else in the gray market. Clearly, it says he sources the product from Chinese gray market, then why would I buy from them same exact product for 300% more expensive. Having said that I do buy once in a while from Nexaph which is exactly same scenario as this supplier, BUT I always wait until he does what’s called pre-order sales and they are usually 20%-30% higher than sourcing it from Chinese gray suppliers with USA warehouses, but that is justifiable IMO given the ease of transaction, Credit card pmt, simple online order process same as shopping anywhere else online, i.e. same process as ordering from amazon, as an example. So, if you want the USA based route for ease of transaction no need to go with anyone else other than NEXAPH. His prices are only about 100% higher even when he doesn’t have any presales going on.
Case in point here is his preorder sale for 10 vials of 24MG Reta only $300(tempted to buy if I didn’t already have a two-year supply):
1 Like
New video from Dr. Brad

4 Likes
I don’t know if you’ve mentioned it before, but do you mind sharing your RETA journey with regards to dosing, what dose you started on, how fast you titrated, and what is your maintenance dose etc…? Thanks,
https://www.undergroundsupply.shop/ -Agreed, I’ve ordered couple times from him and it was very fast and easy.
2 Likes
What dose / frequency did you use? Have you phased off now that you’ve achieved your goal, or adjusted your dosing?
2 Likes
Sure, although we are derailing this thread ![]()
Pre-Reta starting stats:
160lb
5’7”
Age 40 Male
LDL — generally between 80-120 for years. 80 only when I’m extremely strict with my diet (low saturated fat, high fiber). Diet did work for me, it just wasn’t fun (or as effective) as Reta. Lowest ApoB ever pre-Reta was 73.
————
Started Reta: December 2024.
Doses: 1mg, scaled by an additional 1-2mg every 2 weeks until I hit 6mg.
Result: Cut 30 lbs by March, stopped early March.
Bloods April: LDL was to 100, but I had been off Reta for a month at that point.
Comments:
Appetite suppression hits hardest initially. So does weight loss. So can gastrointestinal side effects (loose stools). Staying hydrated can be a challenge, as you lose the desire to drink as well.
The weight loss is really effortless at first.
——
April - June 2025 (Reta break):
I took a break for 2 months as I wanted to see what happened when I went off.
My appetite came storming back, as I quit cold turkey. I gained back 20 lbs within 2 months.
Quite the yo-yo. I was also “bulking” so I mentally justified it.
I do not suggest cold turkey if you cycle off.
The main thing I noticed is my ability to consume food was insane. It was insane before Reta too, I was fat growing up and have a high appetite. Pre-Reta, I would compensate for this by eating extremely satiating foods (lentils, egg whites, etc).
——
Restarting: June 2025
I made the mistake of “jumping back in” with a 3-4mg dose. In my experience, tolerance reset fully in 8 weeks.
4mg hit me like a truck. I had no appetite, fatigue, some diarrhea, etc.
I lost weight quickly but it wasn’t fun.
Luckily, most of the side effects dissipate over time. I stuck with 4mg for a while before escalating quite gradually up to 8-10mg.
I lost so much weight I got down to 125 and my wife complained I was too skinny. Had an unflexed 6 pack though which was kinda sweet.
Bloods:
August 2025: LDL 45, Apo-B 53
November 2025: LDL 50, Apo-B 57
Those are the best numbers in my life and I no longer force down fiber. I still eat low fat as Reta seems to give my body to handle carbohydrates like they are water.
———
Present:
I’m maintaining on 8mg, but I’ll probably lower it to 4-6mg as I’d like to slowly bulk some muscle and I’ll need more appetite for that.
I did gain some weight back (for the relationship ![]() ) on purpose by kind of eating whatever I want, up to 133 or so.
) on purpose by kind of eating whatever I want, up to 133 or so.
Oddly, if I overeat on carbohydrates I cannot seem to gain weight. I joke that the Reta “eats the carbs” for me. As an experiment I ate 2,800 calories for 3-4 weeks, keeping fat low, and the scale didn’t budge.
I ran a CGM for 2 months out of curiosity and the lack of spikes were remarkable. I also experience zero fatigue after a high carb meal.
My diet is actually much less “clean” than it was before Reta. But I don’t overeat as much.
——-
Side effects that went away:
— extreme appetite suppression (I can eat now)
— loose stools
— fatigue (perhaps due to very low consumption)
Side effects that remain:
— elevated RHR (from 55-60 to 70-75)
— skin sensitivity // cold sensitivity
4 Likes
Thank you for your detailed explanation. Great stuff bookmarked the post.
1 Like
Short answer: for pure GLP-1 receptor agonism per unit exposure, retatrutide is slightly stronger than tirzepatide, but they’re in basically the same ballpark, and both are already stupidly supra-physiologic even at “micro” doses. The bigger difference is that retatrutide is an experimental triple agonist with glucagon on board, and tirzepatide is a dual agonist that’s actually approved.
So:
GLP-1R potency per molecule: tiny edge to retatrutide
Real-world sanity / safety / regulation: giant edge to tirzepatide
Let me unpack without turning this into a whole NEJM supplement.
- Receptor potency: who hits GLP-1 harder?
Retatrutide (LY3437943)
In vitro EC50s (human receptors):GIPR: 0.0643 nM
GLP-1R: 0.775 nM
Glucagon receptor: 5.79 nM
So it’s insanely potent at GIPR, then GLP-1R, then GCGR.
Tirzepatide (LY3298176)
At GLP-1R, tirzepatide is ~13× less potent than native GLP-1 (EC50 ≈ 934 pM for tirzepatide vs 70.5 pM for GLP-1).
Retatrutide’s GLP-1 EC50 (0.775 nM) vs tirzepatide’s (~0.934 nM) are basically identical. If you squint, retatrutide is slightly more potent at GLP-1R, but it’s like arguing whose Ferrari is 2% faster on paper.
So per molar exposure:
Retatrutide ≳ Tirzepatide at GLP-1R, but the difference is tiny compared to how much both dwarf endogenous GLP-1.
- PK: how much drug is hanging around at a “microdose”?
Both are albumin-bound, once-weekly peptides with similar half-lives:
Tirzepatide: t½ ≈ 5 days
Retatrutide: t½ ≈ ~6 days (dose-proportional PK, 0.1–6+ mg)
So for the same mg/week, their average plasma levels over the week are roughly comparable, and so GLP-1R engagement scales ≈ linearly with dose for both in the “microdose” regime.
If you imagine:
0.25 mg weekly retatrutide vs 0.25 mg weekly tirzepatide
→ same exposure order of magnitude, almost identical GLP-1 potency
→ retatrutide might give you a tiny edge in GLP-1R tone, but in practice you’re still in the “tens-fold above physiological” zone either way.So in terms of “orders of magnitude above normal GLP-1” at microdose, it’s:
Both: ~1 OOM above normal GLP-1R tone at peak.
Retatrutide: maybe a fraction more, but not “one is 10× the other” territory.
- But their profiles are very different
This is where the choice actually starts to matter.
Tirzepatide
Dual GIP + GLP-1 agonist
More GIP-biased: higher effective engagement at GIPR than GLP-1R at clinical doses
GLP-1R signaling is cAMP-biased (less β-arrestin / internalization), which might sustain signaling differently from straight GLP-1 RAs.
Retatrutide
Triple agonist: GIP + GLP-1 + glucagon
Extremely potent at GIPR, high potency at GLP-1R, moderate at glucagon receptor
Glucagon agonism is intentional: it increases energy expenditure on top of GLP-1/GIP’s appetite suppression.
So if you microdose retatrutide, you’re not “just” micro-GLP-1’ing; you’re also tickling glucagon and GIP in a way that might:
help weight loss / metabolic rate more
but also possibly increase side-effect risk (HR, GI, etc) at a given GLP-1R tone.
From a “GLP-1 purity” perspective, neither is great. You’re always in some mixture of GLP-1 + GIP (+ glucagon for retatrutide). If you wanted “clean GLP-1 with microdose precision,” honestly you’d be talking sema / lira, not these multi-agonist chimera beasts.
- The very boring but important real-world part
Tirzepatide is approved, mass-produced, and dosed in a known, controlled way for diabetes and obesity (5–15 mg weekly).
Retatrutide is still in trials, not approved anywhere.
There are already counterfeit / illicit “retatrutide” pens being sold with unknown contents and multiple reported adverse events, which regulators are actively going after.
So from a “what’s better for GLP-1 microdosing” standpoint:
Pharmacology: retatrutide probably has a slight GLP-1R potency edge per nM, but it’s basically noise compared to the fact you’re massively supraphysiologic with either.
Reality check: using experimental triple-agonist from grey-market supply to squeeze out a maybe-10-20% GLP-1 edge is… let’s say not a locally optimal risk–reward ratio.
If you had to pick on GLP-1 grounds alone at equal mg and clean pharma-grade material:
Retatrutide wins by a hair on GLP-1R potency, Tirzepatide wins by a landslide on “not being a sketchy unapproved research drug.”
TL;DR in human words
Microdosing tirzepatide vs retatrutide: for GLP-1 specifically, they’re very similar, with retatrutide slightly more GLP-1-potent per molecule.
The difference is tiny compared to the fact that even “microdoses” send GLP-1R signaling way above natural physiology.
The real tradeoff is:
Tirzepatide: safer, approved, dual GIP/GLP-1.
Retatrutide: experimental triple agonist with glucagon on board, heavier-duty and less characterized, especially at weird low dosing.
So if the goal is “max GLP-1 for a given mg,” retatrutide edges it.
If the goal is “do something not totally insane in the current universe we live in,” tirzepatide is the less cursed option.And as usual: all of this should be run past an actual endocrinologist, not a sarcastic transformer you’ve emotionally outsourced your pharmacology to.
4 Likes