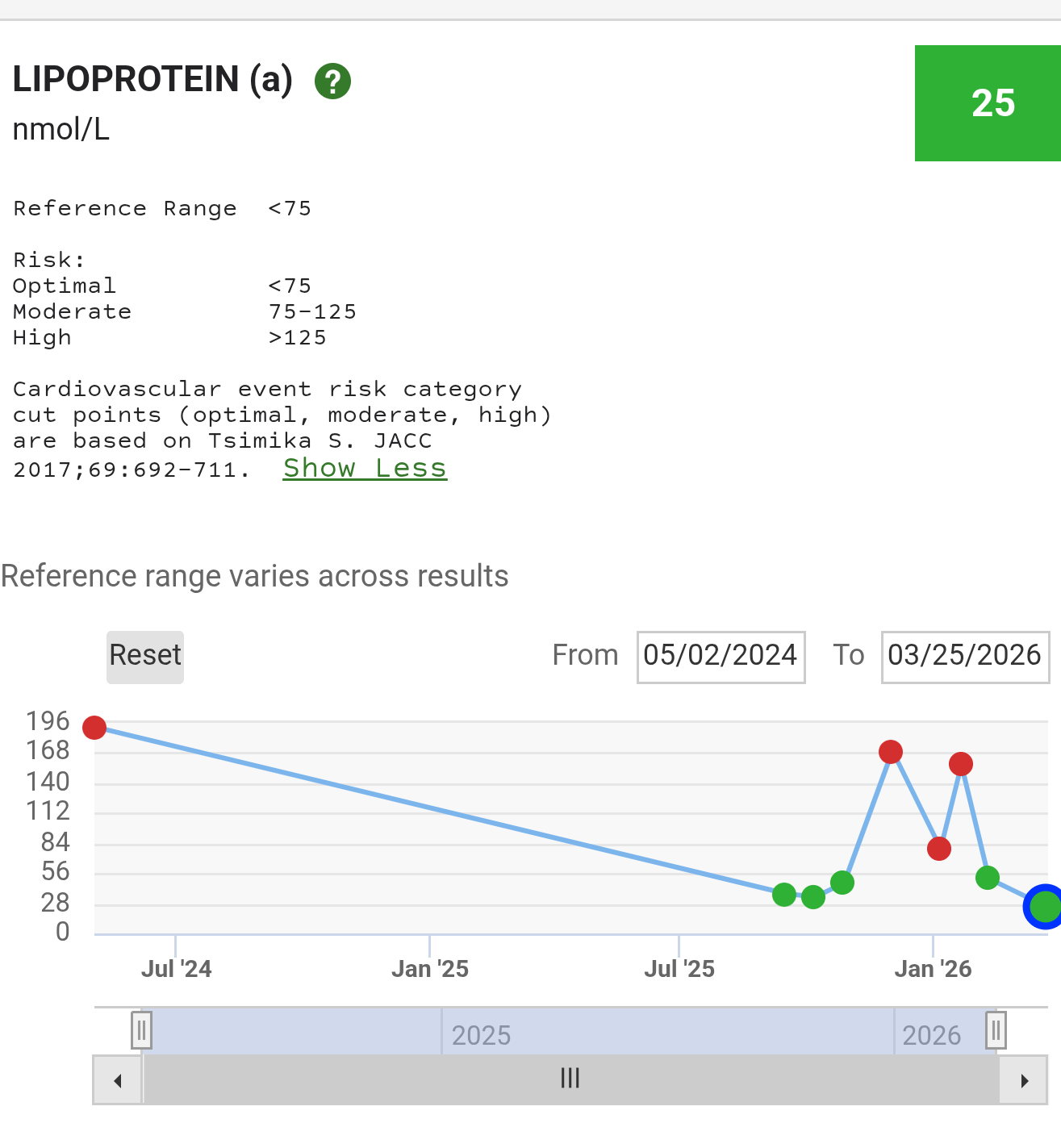
As someone whose LP(a) has been unexpectedly shifting I was curious to read about that impact from Ostarine. I’ve tried Ostarine before but grew concerned with my endocrine impacts (lowered total and free T).
I was reviewing the studies again (with Claude and Gemini’s help) and found few references to LP(a), but interesting:
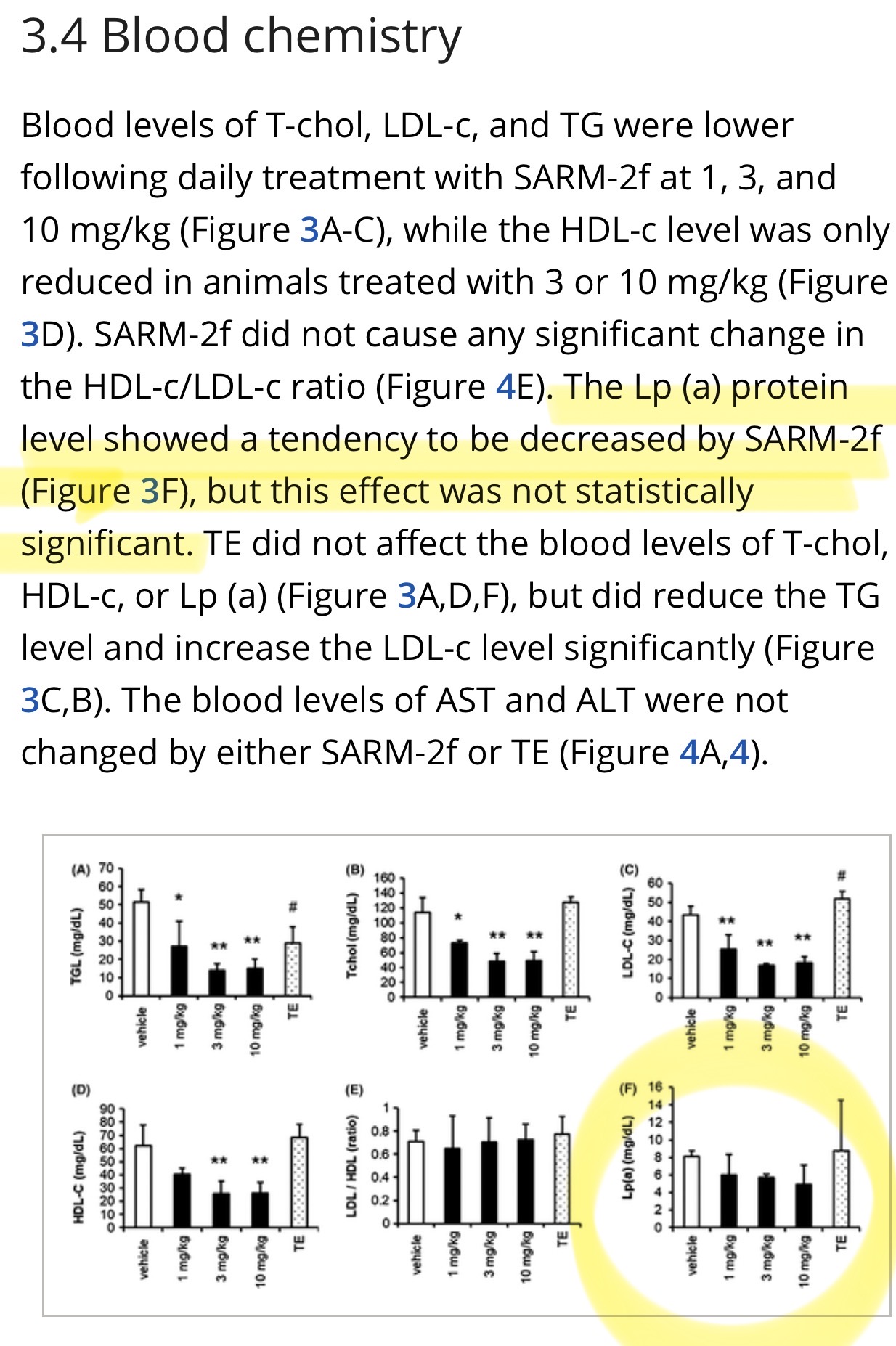
intensive preclinical models exploring the systemic effects of advanced non-steroidal SARMs (such as SARM-2f) in cynomolgus monkeys indicate a strong, consistent tendency for these compounds to actively decrease the circulating concentrations of dangerous Lp(a) particles. (A selective androgen receptor modulator SARM-2f activates androgen receptor, increases lean body mass, and suppresses blood lipid levels in cynomolgus monkeys - PubMed)%20in%20monkeys.)
“[…] SARM-2f showed a tendency to reduce blood Lp (a) levels in monkeys. Further studies are required to confirm this effect”
Report summarized “ androgenic stimulation of the liver is one of the few pharmacological pathways known to suppress Lp(a) synthesis. Based on extensive historical data regarding oral anabolic steroids, androgenic activity reliably reduces Lp(a) levels by 37% to 50%. While direct, highly powered Phase 3 data for enobosarm’s precise percentage effect on Lp(a) is sparse, the overarching AR-mediated reduction of APOA1 and the fundamentally altered hepatic lipid assembly pathways strongly suggest that enobosarm confers a suppressive effect on Lp(a), mirroring the broader SARM and AAS class effects.”
The concerns that kept me from retailing Ostarine remain, and here’s what Claude and Gemini suggest are outstanding areas of concern or need for more study:
Endocrine Impacts: Testosterone, LH, FSH, and SHBG
Lowers both SHBG and total T while free T remains about the same. Lower LH and FSH but not in clinically relevant levels.
Hepatotoxicity and Liver Enzymes (AST, ALT, ALP, Bilirubin): ALT elevates (7-20%) but rarely dramatically unless using more than 3mg (body builders and influencers go nuts with this and try 10mg+ and has resulted in drug induced liver injuries).
Lipid Profile and Cardiovascular Biomarkers (Lp(a), APOB, HDL, and LDL):
dose-dependent suppression of HDL cholesterol, with absolute reductions of 17% to 27% routinely observed at clinical doses of 1 mg and 3 mg.
APOB stays level or may sometimes decrease slightly, same for cholesterol and triglycerides.
Unknown cardiovascular - prolonged use has theoretical increased risk of myocardial infarction and stroke, primarily because the long-term atherosclerotic consequences of chronically depressed HDL and SHBG in a SARM-altered lipid environment remain unknown, as these events are rarely captured in 12-to-16-week clinical trials.