Want to have a place for some newer info on rapamycin.
TLDR: * Rapamycin:
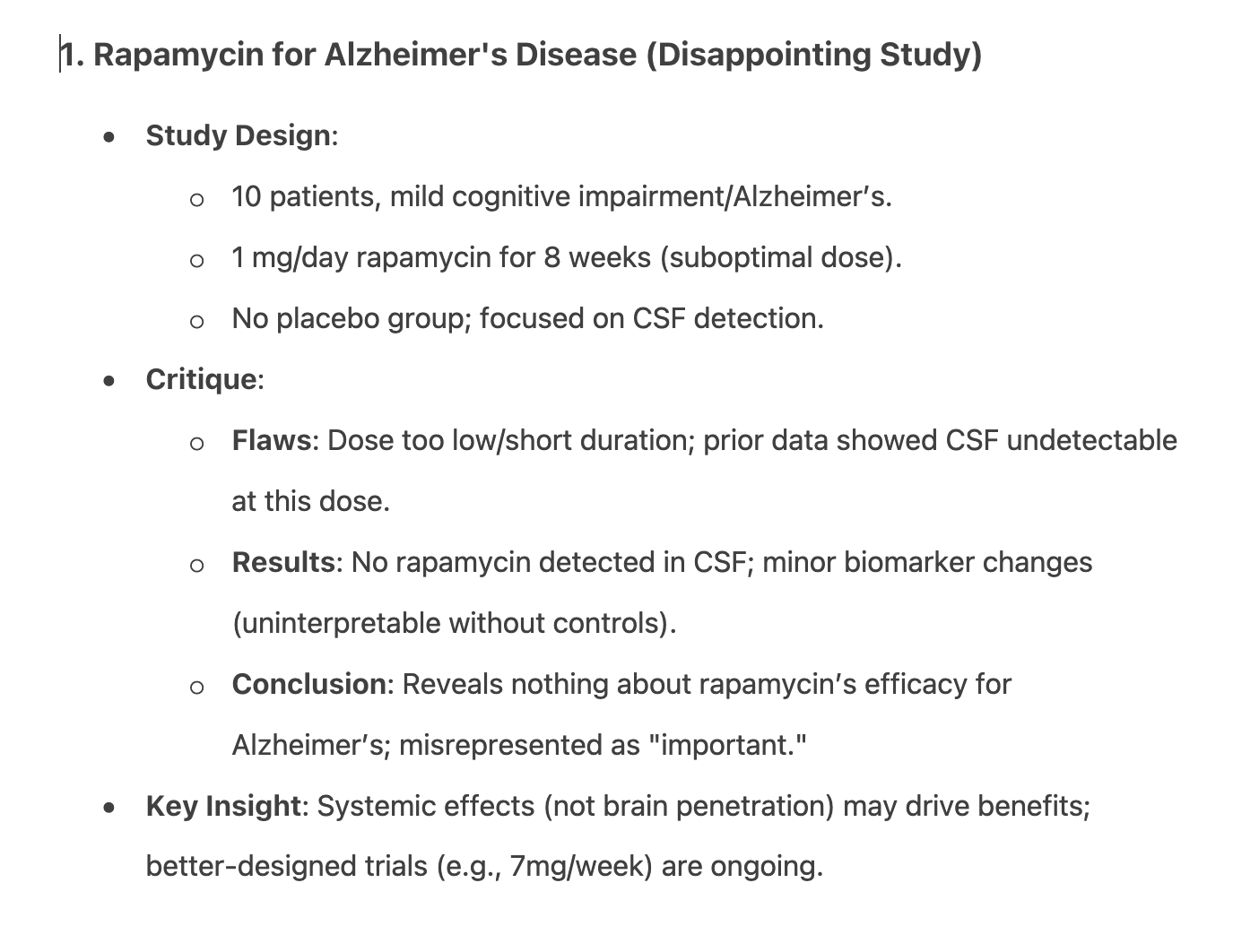
- Low-dose (1mg/day) Alzheimer’s trial was uninformative.
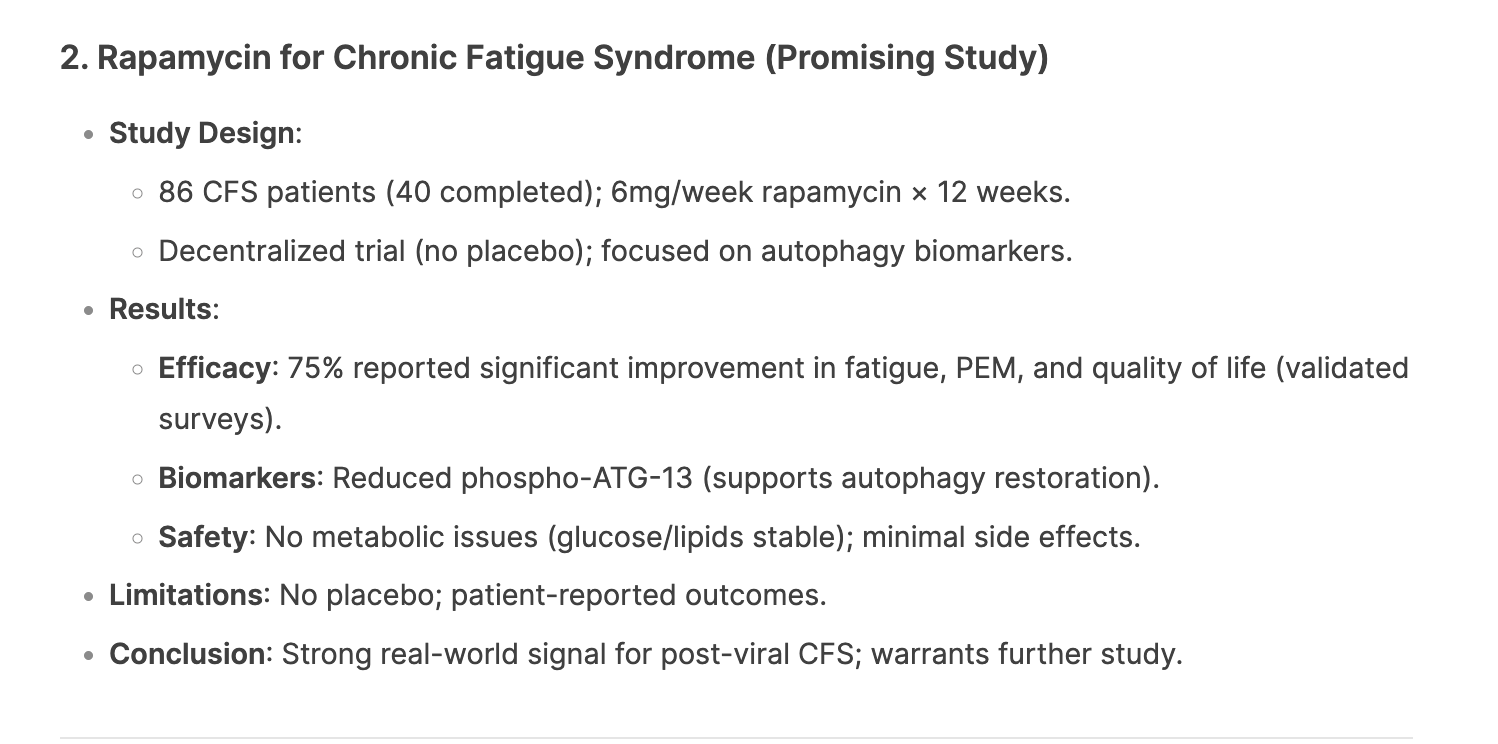
- 6mg/week shows promise for CFS (especially post-viral) with good safety.

Want to have a place for some newer info on rapamycin.
TLDR: * Rapamycin:
I’m freaking out. Peter Attia looks terrible in this video, which aired yesterday.
I don’t get it. Are you joking?
I think it’s just some lighting and camera angles that make creases, etc. look a little worse than normal. I wouldn’t have noticed if you didn’t point it out.
Why? Is PA a paragon of slow aging we are modeling ourselves after? Because I don’t. I’m suspicious of his diet views, massive protein intake promotion including processed meat and protein bars, his obsessively copious exercise and other things. I don’t think he looks younger than his calendar age (to my eyes), but looking younger is no guarantee of superior health or longevity. But he also doesn’t look way older than his age, to me. Seems a nonissue, but maybe I’m missing something.
I did an O3 summary of the video above to save me having to watch it, but there is already a summary in this topic. I can post it if asked. (such as by liking this post).
Otherwise I will assume people consider it clutter.
As requested
(Filler words, repetitions and time‑stamps removed; sense preserved but phrasing occasionally tightened for readability.)
Intro – “Three Hot Longevity Papers”
Welcome to the Optispan podcast. Today I’ll discuss three recent papers that have been buzzing around the longevity world—two concerning rapamycin (my “vitamin R”) and one on taurine.
The study (“Rapamycin treatment for Alzheimer’s disease and related dementias: a pilot phase‑1 clinical trial”) enrolled ten people aged 55–85 with mild cognitive impairment or mild AD.
Why 1 mg/day? No rationale is given. Transplant patients take several mg/day; longevity self‑experimenters favor 4–10 mg once weekly to achieve high peaks then troughs below detection, which seems both safer and more effective.
Blood data from the same group’s earlier work show 1 mg/day only yields 4–8 ng/ml in serum. Even if 10 % crossed into CSF, that would be 0.4‑0.8 ng/ml—below the assay’s 1 ng/ml limit. Unsurprisingly, the study found no CSF rapamycin. An ALS trial that used ~2–4 mg/day likewise found none.
Side‑effects were minimal, but without a placebo we can’t know if rapamycin mattered. Three CSF biomarkers (p‑tau, GFAP, NfL) rose slightly yet significantly—but the between‑person variance dwarfed the change, and natural disease progression wasn’t controlled. The authors themselves state the outcomes “cannot be clearly interpreted.”
A better‑designed phase‑2a trial (“RAP‑AD”) will dose 7 mg weekly and include imaging, cognition and CSF levels; that should be far more informative. Importantly, rapamycin might not need to enter the brain directly; systemic mTOR inhibition could indirectly suppress brain mTOR activity.
Early human data in APOE‑ε4 carriers already hint at improved brain volume and perfusion with rapamycin.
A new pre‑print (“Low‑dose rapamycin alleviates clinical symptoms of fatigue and post‑exertional malaise via improved autophagy”) followed 86 ME‑CFS patients in a decentralized, uncontrolled study.
Results: 29/40 (~73 %) reported strong improvement in fatigue, post‑exertional malaise and orthostatic intolerance, with p‑values < 1 × 10⁻⁴. Post‑infectious cases (e.g., long‑COVID) improved the most. Lab chemistry showed no changes in HbA1c, fasting glucose or lipids, and adverse events were mild and transient.
Limitations: no placebo, self‑report, heterogeneous pharmacy formulations, three‑month duration. Yet molecular changes line up with symptom gains, suggesting a real effect. Author’s takeaway: if you have moderate–severe ME‑CFS, weekly rapamycin is worth discussing with your physician.
A Science paper reassessed whether circulating taurine declines with age. Using longitudinal cohorts of humans, monkeys and mice, the authors found no consistent age‑related drop, challenging the 2023 report that had spurred taurine‑supplement enthusiasm.
The new work does not test taurine supplementation’s ability to extend lifespan or healthspan, so it tells us nothing about taurine as an intervention. The press‑release comment that taurine’s efficacy “may be context‑dependent” is a truism: everything in biology is context‑dependent. Without the hard replication of the lifespan data, this feels like an expensive non‑answer.
Outro
Of today’s three papers, two (rapamycin‑AD and taurine) were disappointing; the ME‑CFS study, despite caveats, looks genuinely promising. Questions welcome—let me know where I’m wrong.
| Study | What was done | Key findings | Host’s verdict |
|---|---|---|---|
| Rapamycin 1 mg/day in AD | n = 10, open‑label, 8 weeks; looked for CSF drug & biomarkers | No CSF rapamycin; small biomarker shifts of uncertain meaning | “Very unimportant”— dose too low, duration too short, no placebo |
| Rapamycin 6 mg weekly in ME‑CFS | n = 86 (40 completers), decentralized, 3 months | ~73 % reported marked clinical improvement; supportive autophagy markers; minimal side‑effects | Potentially game‑changing for post‑infectious ME‑CFS; deserves larger RCT |
| Taurine biomarker study | Longitudinal measurement in humans, monkeys, mice | Taurine levels do not reliably fall with age | Technically solid but addresses a low‑value question; says nothing about supplementation benefits |
The host’s skepticism is warranted. A phase‑1 pilot can sacrifice statistical power for safety data, but dose and endpoint must still be justifiable. Here:
However, the study is not entirely useless: it re‑confirms safety at low daily dosing in cognitively impaired elders and sets the stage (via IRB groundwork) for the higher‑dose weekly RAP‑AD trial now underway. (ResearchGate, Scholars @ UT Health San Antonio)
Strengths the host notes—and I agree—include:
But some caveats deserve sharper emphasis:
Still, given the dire therapeutic vacuum in ME‑CFS, even an imperfect open‑label signal is valuable and justifies a rapid, well‑powered RCT. (PubMed, ResearchGate)
Here the host may undervalue negative results. Demonstrating no longitudinal decline undermines the narrative that falling taurine drives aging; that matters if taurine’s advocates invoke deficiency as rationale. Yet I share the criticism that the study stops short: lifespan or functional read‑outs in mice (easy and inexpensive by comparison) would have answered the pressing question of intervention efficacy. The opportunity cost—allocating primate resources to descriptive plasma work rather than a replication of the 2023 supplementation experiment—feels high. (Science, National Institutes of Health (NIH), PubMed)
For clinicians and patients: weekly rapamycin remains investigational but is showing a favorable safety‑signal and potential in post‑viral fatigue; taurine’s longevity benefits remain speculative until supplementation outcomes are replicated.
He looks age appropriate to me. He definitely doesn’t look terrible.
We must be looking at two different videos, because on this one he looks really good and toned. He has a tendency to look a bit swollen, like puffed eyes and face (not as bad as Sinclair though) but in this one he looks really healthy and good. Plus, the dude is over 50, what do you think he’ll look the same as he did in is 20’s.
![]() David Sinclair’s Longevity Supplements: NMN, Resveratrol, Quercetin! #aging #nmn
David Sinclair’s Longevity Supplements: NMN, Resveratrol, Quercetin! #aging #nmn
I also think he looks fine. I think he obviously started glp1s and lost the 10lbs he said he wanted to lose. So, while I think he still looks good, yeah, it will age your face a bit.
And as I learned from my idol, Barbara Walters, when you get older, you have to choose your ass or your face. I was definitely cuter with an extra 10! My brother hates how my face looks now, but I said, but my tush is better ![]()
The worst is when you lose weight/fat if it comes from the certain areas in the face like under eyes and nasolabial fold area, which ages people so much. This is more common in older people but I have seen it happen to younger people in their 20’s with unfortunate genetics.
He’s 52 … submit it to Novos face age and see what it says (if anyone has the time) … Face age seems as good as other markers of age. Maybe a bit too much IGF-1 going on here with all the protein. Could just be lighting.
Apparently there is some truth to this, as there are several sites that guess/predict your age from a photo.
Personally, I don’t think it is very accurate—too many variables like sun exposure, smoking, etc., etc.—but then neither is the Levine age test nor many other age tests now available.
Well - consistent with my usual approach, if the data favors me, I’ll go with it. Novos face age was very kind to me, so I’ll believe in it full heartedly and not go with anything else that might score me worse.
I often use face aging apps for tracking general tendency in health changing and aging. They do catch little details like puffiness or discoloration. I don’t think they are accurate in determining age but for general changes in connection with aging they are useful. My recent picture was evaluated by age.toolpie.com as 26 and I’m 70. Of course I don’t look 26. Novos evaluations though are more realistic imo.
Well that’s about his age. ![]()
That is his age! So he looks his age, not older at all.
The problem imo is that most ppl don’t have realistic expectations about natural aging. We all are brainwashed by celebrities augmented looks and often perceive makeup free or fillers free faces as old or sick. Look at some comments about Pamela Anderson makeup free face. She really looks wonderful but most see it as “horrible”. Artificial is quickly replacing natural and it becomes a norm.