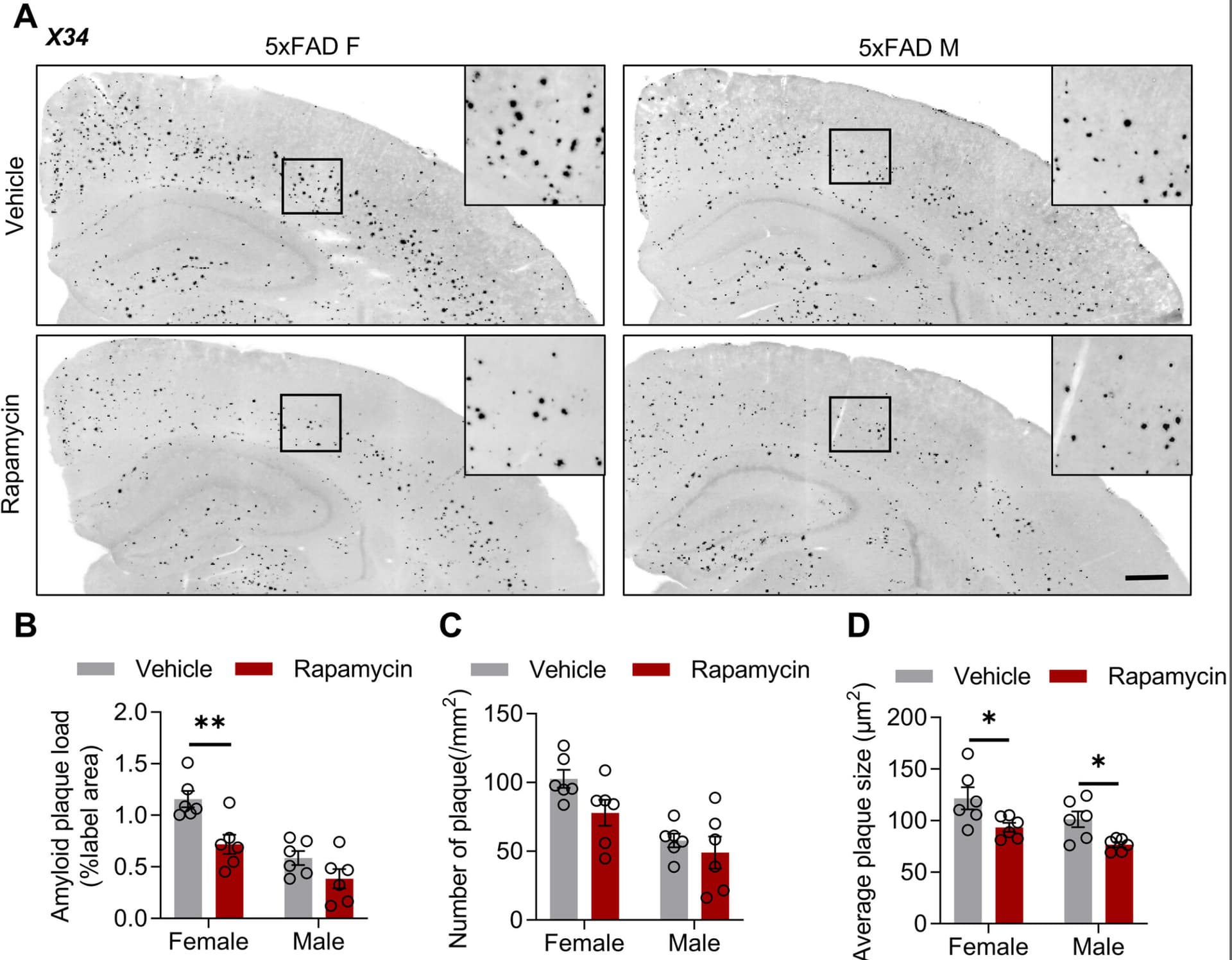
Rapamycin treatment exacerbates amyloid plaque load and decreases the number of CD11c⁺ microglia in the brains of 5xFAD mice.
Rapamycin treatment decreases central immunoproteasome content and activity in 5xFAD mice.
Rapamycin alters peripheral immune cell populations, including granulocytes and splenic lymphocytes.
Sex-stratified analyses reveal immune differences but no sex-specific rapamycin effects.
Results support a stage-dependent TREM2–mTOR–DAM axis in amyloid pathology.
Summary: The mammalian target of rapamycin (mTOR) is involved in immune regulation and in the metabolism of β-amyloid (Aβ) and tau peptides in Alzheimer’s disease (AD). In this study, we investigated the effects of the mTOR inhibitor, rapamycin, on central and peripheral immune profiles, proteasome activity, Aβ pathology, and spontaneous exploratory activity and place recognition in the 5xFAD mouse model of amyloid pathology. Using flow cytometry, we found that rapamycin induced changes in immune cell numbers and phenotypes in 5xFAD mice, notably a significant decrease of CD11c+ microglia in cortex and hippocampus of 5xFAD mice. This was associated with increased Aβ plaque load. Concomitantly, we observed a decrease in immunoproteasome content and activity. In peripheral blood, rapamycin treatment resulted in higher percentages of granulocytes, whereas splenic T lymphocytes were reduced. No changes in the open field and modified Y-maze tests were observed following rapamycin treatment in wild-type and 5xFAD mice. Our results reveal detrimental effects of rapamycin on amyloid plaque accumulation and CD11c+ disease-associated microglial subsets in cortex and hippocampus of 5xFAD mice, which is an important finding given two ongoing phase 2 clinical studies of rapamycin treatment in AD.
“Finally, we assessed spontaneous exploratory activity in the open field and place recognition after 30 min in the Y-maze in rapamycin-treated 5xFAD mice at 5 months of age.“
Any chance of finding this aspect of the publication? It’s paywalled.
When rapamycin enthusiasts invoke the ITP results, a common retort is to point out that mice tend to die overwhelmingly of cancer, and the other big killers in humans, CVD and dementias like AD are not spontaneously found in rodents. Therefore if rapamycin is highly effective against cancer, but ineffective against CVD and AD, the great results in ITP may be much less impressive in humans.
Be that as it may, if rapa works against cancer, but is neutral (ineffective) against other major killers, that’s still a win. But things would certainly change if rapa was not merely neutral in AD, but actively detrimental. If this was shown in humans, it might give one pause. But this is in mice. Mice specifically engineered to express features of AD. Not ideal.
Even assuming this result could translate to humans, two points. One, these mice overexpress amyloid production. Is this relevant to someone who doesn’t have any underlying AD pathology and doesn’t therefore overexpress amyloid production? Sure, rapa boosts amyloid production, but does that boosting need for there to be AD pathology present to begin with? Of course, a not insignificant percentage of people may have AD pathology, at least in early stages. But that brings us to point two - high burden of amyloid plaques/tangles are an ambiguous feature of AD. It is certainly present in diagnosed AD, but its mere presence does not by itself assure an AD diagnosis; here far more decisive is tau pathology. I’d be much more interested in the impact of rapamycin on tau expression. Separately and by the by, when the heck are we going to have the marmoset study ready for full peer review? It would be nice to find out if rapa has any impact on NDDs in marmosets. Also while dogs don’t get AD, they do get dementias, so results there might also be of interest. Ultimately of course, we should be able to observe this in humans, including transplant patients.
Reduced Prevalence of Dementia in Patients Prescribed Tacrolimus, Sirolimus, or Cyclosporine