“For the sirolimus plus grapefruit juice study, sirolimus was administered alone in week 1 and with grapefruit juice starting in week 2, one day prior to sirolimus. Grapefruit juice (supplied by Florida Department of Citrus), 240 cc, was administered once daily without interruption. This dosing was based on research demonstrating that the half-life of intestinal enzyme inhibition of grapefruit juice is 12 hours(21) thus providing time for modulation prior to sirolimus dosing”
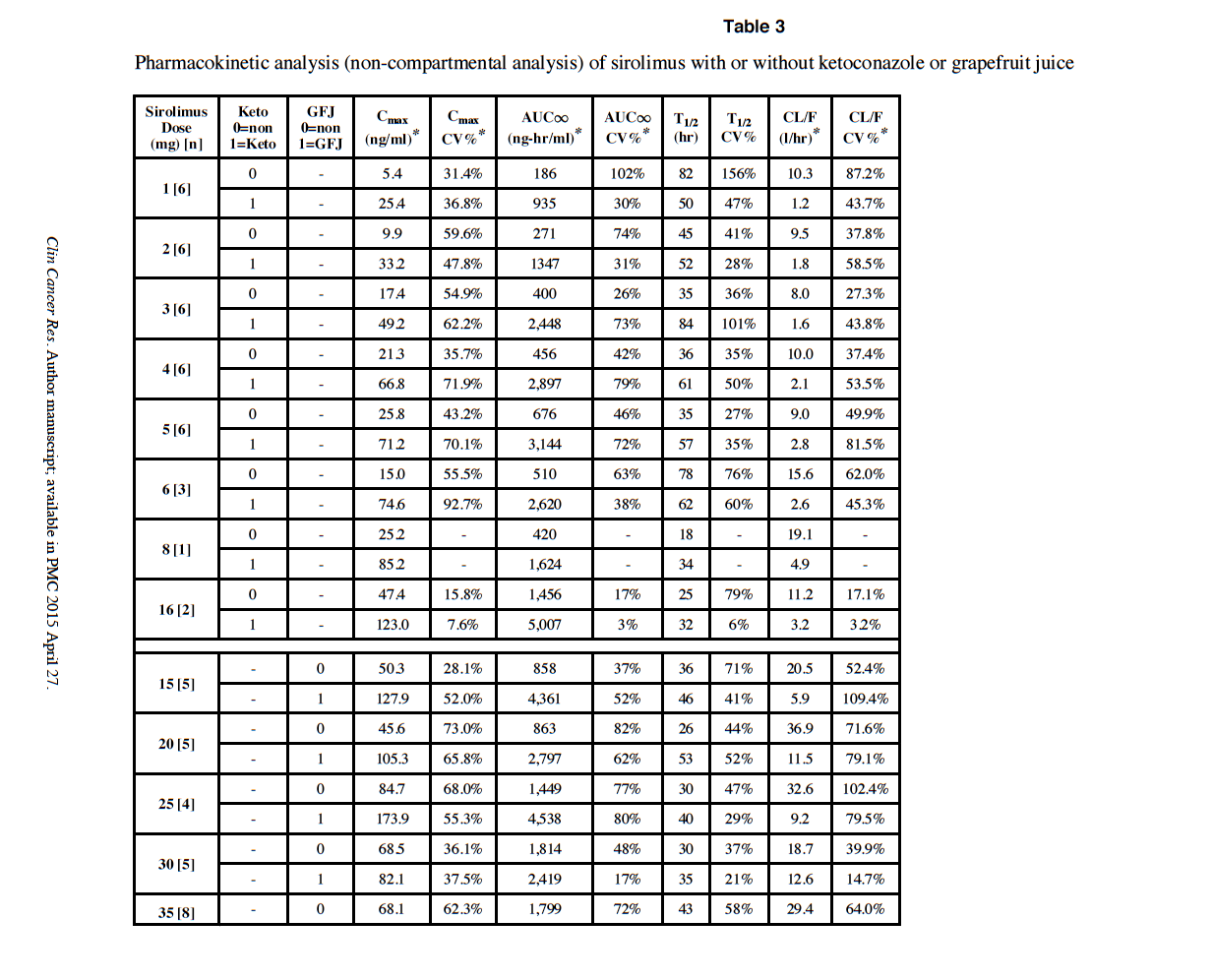
At 5mg with GFJ, Cmax in the study is around 70 ng/ml. As you can see, there are some Cmax over 100 ng/ml.
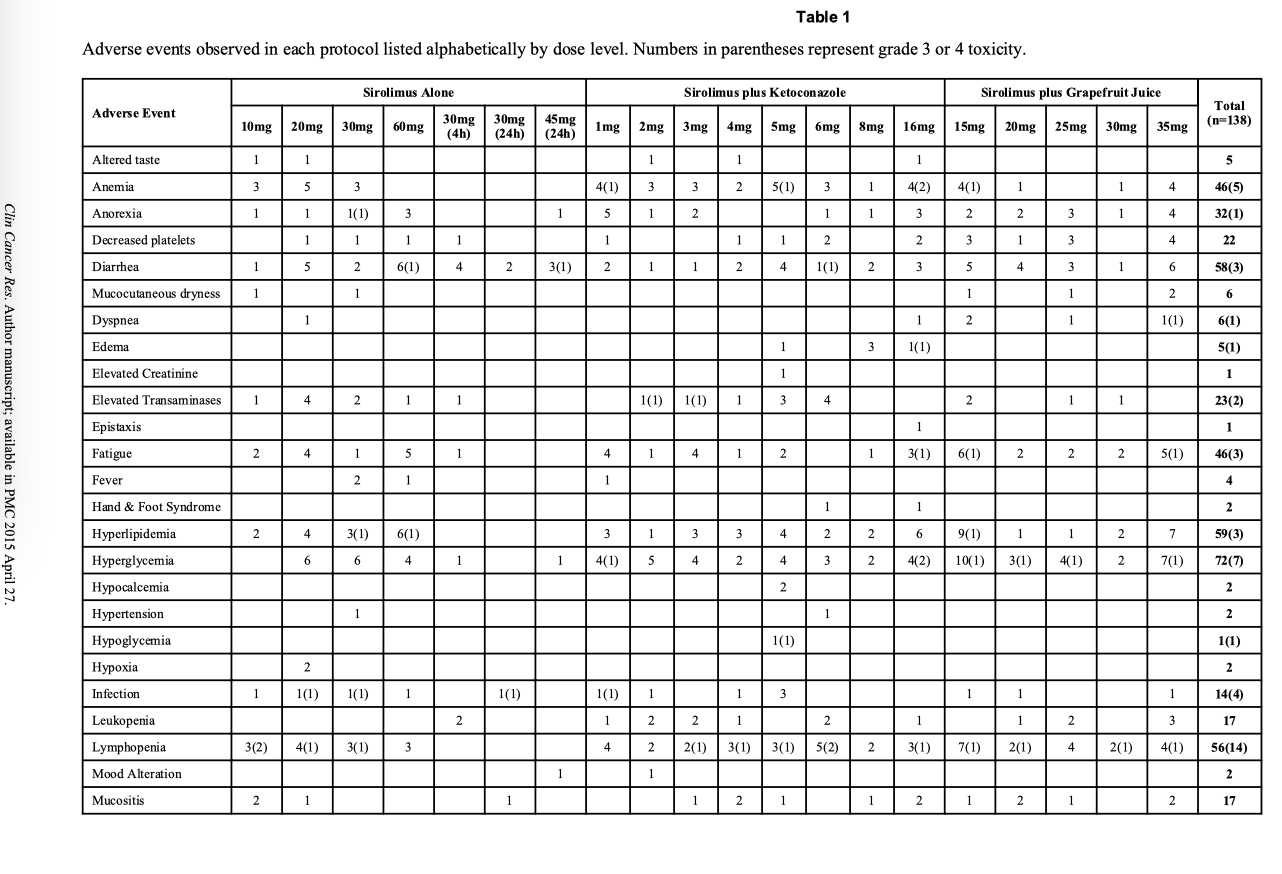
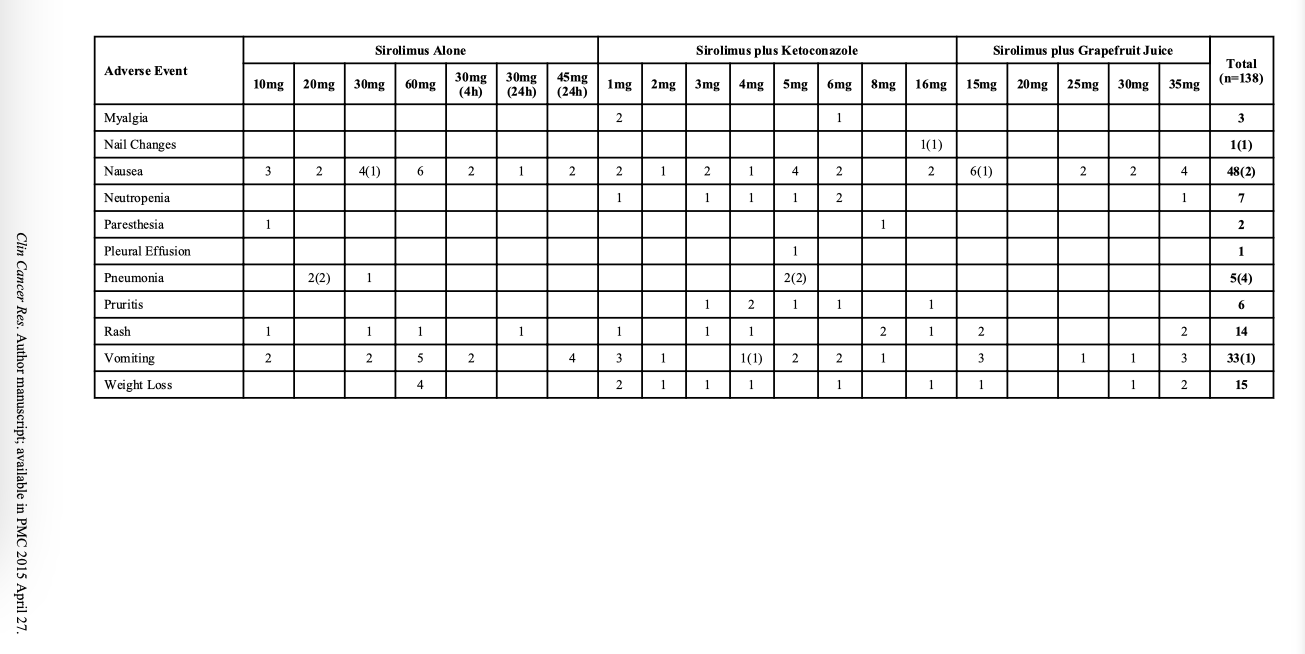
It’s the wild wild west for exploring the max without side effects. See Table 1 in the referenced study.
Yes, would be good to also get a trough measurement.
I am taking 12mg weekly with dual night before/morning of GFJ. But I’ve not fully vetted my Rapamycin current vendor.
I just got my new Rapamycin order, sending out for confirmation lab analysis, and then will redo a blood Sirolimus experiment, both trough, and trying to capture the signal after GFJ/dose. Will post.
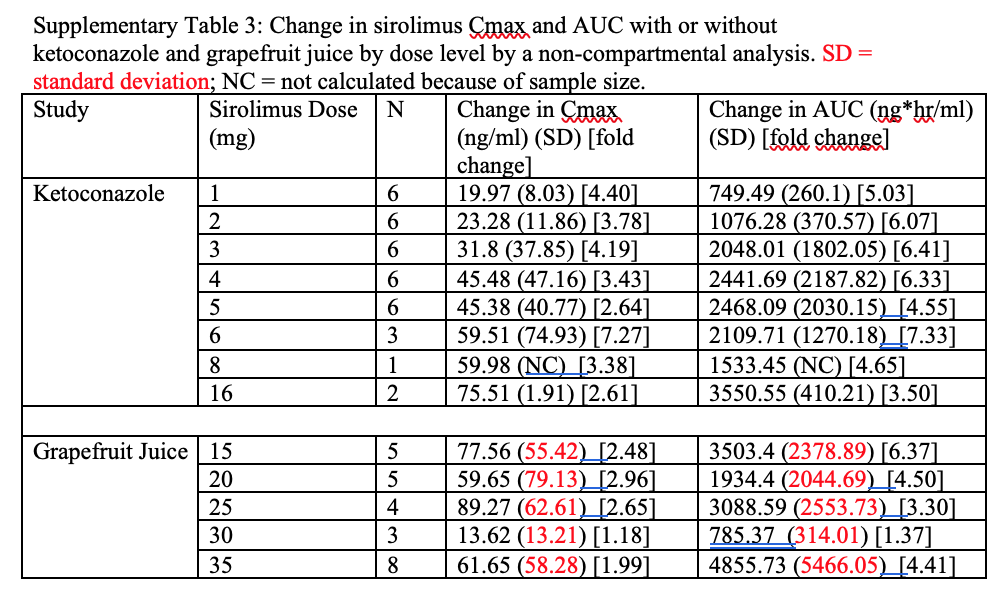
If I am reading this chart right, 5mg rapa + ketoconazole produced Cmax=71.2. The grapefruit was tested only with 15mg-35mg levels. The 15mg +GF produced Cmax = 127.9. My own 5mg + GF produced Cmax=17. So, yes, if you scale down their 15mg to my 5mg, my Cmax seems low.
But the question remains, is this a good therapeutic range?
Yes - we really have very little idea here (at least in any specific, measurable way). Nor do we know how large the dose / response variation might be between people. Its frustrating to have so many unknowns around rapamycin.
Define “therapeutic”? I am 57, I doubt any of these definitive answers will come in my lifetime.
My current n=1 philosophy is to push the outer range, without significant side effects or blood marker dysregulation, balanced against superior physical and cognitive capabilities.
I had one canker sore, and no noticeable side effects, or blood marker dysregulation as of yet.
Wild type mice only die of cancer…Rapamycin delays their death, but they still die of the same cancers.
How many people on this forum are doing advanced preventative cancer, CVD, or brain imaging scans as yet another reference marker?
But humans die of a great many other causes, CVD, cancer, neurodegenerative, diabetes and all the related organ complications.
With all my hacks, I am trying to address as many mortality pathways as possible…the goal should be to push out all cause mortality.
Assuming you’re taking Sirolimus tablets, your peak level blood draw may have been performed a couple hours early (see my previous post above), so your true peak level may in fact be higher than the result you got.
From the FDA drug insert for Rapamune tablets:
“After administration of Rapamune Tablets and a high-fat meal in 24 healthy volunteers, Cmax, tmax, and AUC showed increases of 65%, 32%, and 23%, respectively.”
Did anyone here attend the discussion with Matt Kaeberlein last week on the study, and was there any discussion around what we think we should be optimizing for in terms of dosing - Cmax, tmax, or AUC?
I think this is completely the right approach - we just need to be watching our bloodwork regularly (with a cost of about $70 per cycle its reasonable to do it every few months), and if things are fine there, and no bothersome side effects otherwise, slowly step it up.
I’ve found rapamycin to be surprisingly side effect free overall - I’ve taken doses as high as mid 30mg and really had no noticeable side effects (but need to track the blood work more closely).
Yes, I would love to hear Matt Kaeberlein’s thoughts on this topic.
In the ITP for the 42 PPM dose of sirolimus, male mice sirolimus blood concentration was 23 ng/mL (23% median lifespan extension, 8% max) & for females 80 ng/mL (26% median lifespan, 11% max)
Given that our personal weights are all different, I wonder if it might be helpful to also share our dosing protocols expressed as milligrams of sirolimus per kilogram (mg/kg).
Rapamycin was approved in 2006, and has been used safely for almost 20 yrs. There is even a small study paper on “acute Sirolimus overdose” cases, all without any serious permanent effects.
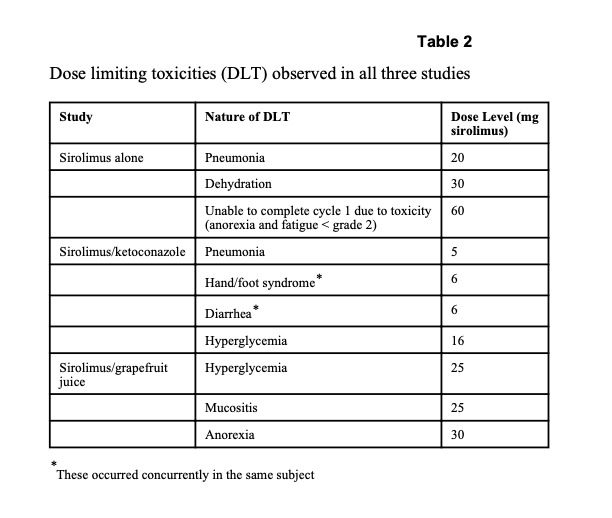
If we look at the GFJ/Ketoconazole/Rapamycin study side effects, in the Sirolimus alone or Sirolimus/GFJ combination, the DLT (dose limiting toxicities) are 20mg+ MIN. Most all of us are taking MUCH less than 20 mg/week.
With regular tracking of biomarkers, I think it’s relatively safe (my personal opinion, I am NOT a doctor, this is NOT medical advice) to explore pushing the envelope of weekly dose, everyone an n=1. I am under the care of a doctor in my journey.
I’ve extracted the side effects tables from the paper.
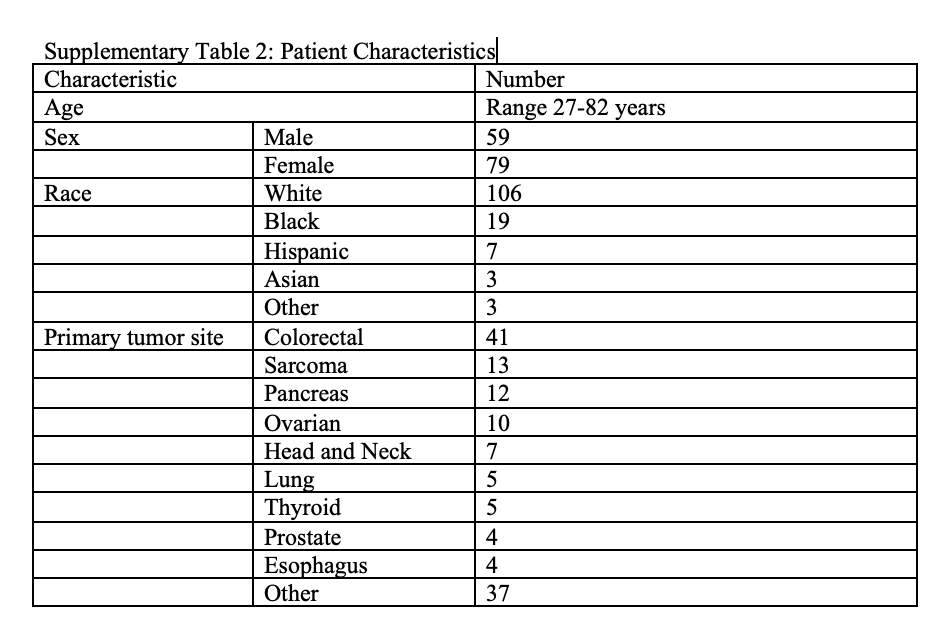
I dug into the supplementary tables for some additional insight.
They did not publish the specific ages of the population, other than 27-82 yo. A good mix of male vs. female. There was no commentary in the paper about pharmacokinetics and age (in case the doctors decided to try different dose by age), nor by sex, unlike many mice studies where there are major differences between sex. But the by-age dose targeting may have been severely confounded by cohort demographics, namely every person in this study had advanced malignancies cancer, mediating their dosing over any age consideration. Similar to other pharmacokinetic papers, there is a wide variation in response between persons.
The 2nd table shows the large variation inter-person, and between dosing levels, in change in Cmax and change in AUC over base Sirolimus alone, highlighting the unique n=1 response. My highlighting of SD In red.
Since I don’t see much, if any, trend in the “fold change” as the dosing levels change, I assume any correlation between fold-change and dosing levels is being swamped by interpersonal variation.
So, for me, at 5mg with GF and the resulting Cmax=17ng/mL, I am falling within a standard deviation of their GFJ at 15mg (Cmax and SD multiplied by 1/3 to 26 ± 18 to account for my lower dose).
Also, remember the grapefruit juice used in those studies was a special GF juice provided by the state of Florida researchers that specifically had high levels of the active ingredients that maximally inhibit CYP3A4. We have no idea how much of those active compounds are in standard store-bought GF juice and/or how much they vary from batch to batch, seasonally and/or between brands.
Most all of the pharmacokinetic studies I’ve read showed significant inter-person variability. Our individual n=1 responses are very complex, leading to intrinsic and fundamental differences in absorption between us, not explained in study replicability/reproducibility.
There are polymorphisms in the intestinal and liver enzymes, including CYP3A4, and others (CYP3A5, CYP2C8, and CYP2C19). There are polymorphisms in the mTOR genes! We all have different gastro/intestinal functionality.
Therefore, if we’re trying to reach certain Cmax/AUC/trough targets, we need to each do our own pharmacokinetic experimentation.
You could take an alternate, blast away approach, starting with high dose, and then dialing back when you reach discomfort/toxicity thresholds. Based on previous studies, these DLT (dose limiting toxicities) markers are noticeable, measurable & reversible.
Here are just a few references of polymorphism effects on pharmacokinetics.
Let’s not forget the variability in the Sirolimus in the pills you get. Since that is the first number in all these calculations it has a profound effect on all the number crunching that follows. Given the host of generic sources and the know problems in quality/quantity, a 1 mg pill could be 1 mg or maybe 0.5…or maybe 0.0.
Testing is expensive but could we set up a system where we join to have a system to share cost of testing across a variety of “preferred” vendors who we use and have good service and price. Publish that. Then do this again in 2 months (or on some continuing basis) so we have validated vendors. Not simple but given all the effort in trying to get to the best dose and other costs involved it seems worthwhile. That is my biggest question in rapamycin dosing…what’s in the pill.
Or maybe MK could share his testing results and the vendor and we can use that.