Liver problems only come from taking the slow release forms. If you take instant release, the liver gets plenty of time to recover between doses and there is no problem.
Instant release will burn. Start with 50’s and just keep taking them whenever you think of it. Pretty soon you can do 100’s…I don’t know if it’s worth it, but it does work. I have been taking Niacin instant release with Rapa for a couple years. My lipids look better than ever and I think it gives me more NAD which helps.
I have no certainty about statins or the risk of having higher LDL.
OK great thanks. I’m aware of the risks with niacin and agree the instant release minimises liver issues. I also wouldn’t take more than 200mg instant release per day in one dose which I pretty sure is unheard of for causing liver problems. I also know that tolerance to flushing builds up.
My concern was it interacting with rapa and causing insulin issues but you don’t seem to have any problems which is good to hear.
This is the study that got me interested in taking it ahead of other (far more expensive) B3s although the benefits weren’t as clear in healthy adults.
A friend and fellow longevity enthusiast, and PHD in biology out of Stanford University had this to say to me about niacin…
I’ve been a fan of Niacin for quite some time. So many great attributes, not the least of which is lowering cholesterol.
I can’t read the whole article, but I’ll assume that they use straight niacin. That being said, I still think the best bang for the buck is the amide version: Nacinamide (aka nicotinamide). I think this is the version that most readily supports levels of NAD.
William B. Parsons Jr. MD was involved in the trials in the US using niacin. The information from the person who did the actually work. This is is a consumer book with a plethora of references
This is a great study, and I had read a summary but did not realize that the result was for people with serious problems to begin with. I wish they would have given one of the controls the Niacin as well to see what happens.
I have found it to be very safe, but also hard to put up with the burn. Also the Enduracin is the one my doctor likes (and he is very knowledgeable about it) but he says don’t use it with a hot beverage such as coffee since the part that makes it slow release is like a wax and it will melt and instantly release. Just FYI. I’m sticking with IR.
No they did give it to healthy people too and there was clear benefit. I made the mistake in thinking otherwise when reading it first too. There was only muscle NAD+ benefit in the patients with mitochondrial myopathy but if you read on there were blood NAD+ increases and improvements in other markers with healthy people too. So it was a very positive outcome.
Yeah, I take a gram and a half every morning and it does very little now. If I take another gram in the afternoon, then the next day I feel nothing with the morning dose. I forget sometimes and then I get a little burn the next day. So it really works best to keep swallowing the stuff.
Not easy to accomplish this. I read a study where they gave people 3 or 4 grams and talked about the results and when I was building up my tolerance over maybe 4 months I kept saying “where did they get these people that can take 4 grams?”
It helps to take with food, and they say nsaids work too, though I never tried.
Been on 500mg of niacin and taking rapamycin since Nov 2021. The niacin dose definitely has an effect on my genetically higher lp(a). The flushing effect subsides faster and is less intense when taken regularly. Non-flushing niacin is ineffective.
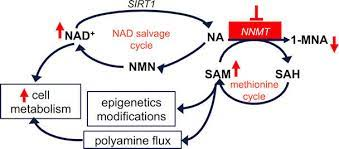
Neither NMN nor NR camps (or the much smaller megadosing niacin vitamin camps) have really discussed the NNMT side - it’s almost always omitted completely. The pilot cited only shows treating a deficiency may be beneficial.
I’m not certain about high-dose niacin necessarily being beneficial for “healthy” people to justify it outside of the indicated uses when an important part of NAD+ is consistently omitted - and we know the trials for atherosclerosis have been not particularly compelling at all. There are also possible known harms with high doses.
Literally, no prospective studies demonstrate Lp(a) lowering with niacin in patients with high Lp(a) is beneficial. Subgroup analyses of trials showed that niacin-mediated reductions in Lp(a) were not accompanied by improved clinical outcomes at all. So there isn’t any reason to use it for that AFAIK.
It reminds me of estrogen replacement therapy reducing Lp(a) levels, yet it is actually discouraged for the use of CVD risk reduction because of negative outcomes.
It’s more likely antisense oligonucleotides towards Lp(a) will pan out or PCSK9 inhibitors make much more sense IMO, but we’ll see.
Colestipol-niacin in coronary bypass patients isn’t equivalent to niacin monotherapy in “healthy” individuals and compliance with colestipol isn’t easy. We see similar effects with colestipol-statin if you dig the same older trials with better safety profiles on the statin.
I suggest you read all the high-dose niacin-related trials, many of them being combination therapies since all the niacin-only ones were flops for improving mortality - CDP, AIM-HIGH, HATS, FATS, and HPS-THRIVE (1 and 2) was enough for me to avoid high-dose niacin as when you go to the larger trials high dose niacin is rather unimpressive with slightly higher all-cause mortality in some and incredibly well-documented serious potential side effects.
There’s a pretty good reason why the medical community found high-dose niacin to be at the last resort therapy in very limited cases and most avoid it entirely. Megadosing vitamins generally have an overall poor track record in terms of increasing mortality slightly - which has been the case with high-dose niacin so far, so you better have really, really good evidence that any of the things you’ve cited actually matter. They’ve been unimpressive when put in context with similar scenarios and plenty of empirical data.
Why would you want to lower cholesterol? It’s been proven a thousand times over in research study after research study, that it’s a myth that elevated levels of LDL-c are dangerous or that it causes CVD. Yes, mainstream medical folks/doctors still subscribe to this myth, in part because it’s existed for so long and because of money (statins).
So I read up on those trials as you suggested. I think your conclusion from them is misguided. The only trials where niacin was shown to have no benefit was shown to have no benefit was when it was combined with statins (most recent trials). It was shown to have no extra benefit in other words. In trials where it was trialled alone, it was shown to have benefit. Including in the trials you yourself mentioned here. Here’s another from the 70s: Coronary drug project: experience with niacin. Coronary Drug Project Research Group - PubMed
From further reading I see that other B3s actually have similar effects on blood work despite initially not being thought to have. NAM, NR and NMN don’t come with the risks NA does as well. There are now multiple documented benefits from B3 supplementation from blood NAD+, to increased muscle mass and strength, reduced fat around organs, particularly the liver, and likely benefits for kidneys, something that is being further investigated in numerous ongoing trials because of promising results in preliminary ones. I think it’s mad not to take a B3 and have chosen NAM myself as it’s the cheapest and they all seem to confer the same benefit.
Having no additional benefit in the case of statins is a real issue. It’s hard not to gloss over it. It’s easy to assume that it’s just statin interaction when these add much larger trials to evaluate niacin.
As for the benefit on monotherapy - I suggest you repeat the potential benefit detected in the trials that is actually meaningful compared to alternatives. Blood NAD+ is not necessarily a meaningful marker. Regardless of the NR/NMN/other camp, I have found people gloss over a large part of the NAD cycle for how NNMT comes into play when describing the potential mechanism of NAD+ supplementation. Ignoring a big part of the biochemistry is an issue - it reeks of bias from the most influential proponents. You’re claiming potential benefits that don’t necessarily translate into real outcomes when mortality isn’t going down, but slightly up.
Did you check the side effects of the trials? Serious adverse events ie myopathy and worsened glucose control/new onset diabetes, infection, and bleeding.
Not to mention, niacin can increase the risk of gout and hyperuricemia. Elevations in LFTs are common - may lead to severe hepatotoxicity, jaundice, and fulminant hepatitis. “Protecting the liver” while potentially causing serious harm to the liver doesn’t seem to be particularly productive.
I’m not saying nobody should ever take high-dose niacin for any reason but it’s not looking particularly good in terms of efficacy or mortality. I’m saying for the average person, I don’t see the point of high-dose niacin when considering the potential for serious side effects generously using extended-release versions vs potential likely marginal benefits.
Even if I was in the small, highly specific patient population where one even would consider using it although somewhat shaky in the first place - I’d be very wary and look into highly specific forms ie Niaspan.
Yes, I recently started taking niacin and then nicotinomide and, not coincidentally, had a gout attack. The B3 products raise the blood’s uremic index, which can cause jagged crystals to form in the joints. B3 has been touted as a panacea, even for kidney disease. But if the kidneys are impaired and can’t remove all the uric acid from the blood, it will be deposited in the joints. Treatment may require a 10-day course in prednisone, followed by 20 days of low-dose colchicine, a gout medication that seems to work pretty well. A DPM said I should be able to run again.