I wouldn’t put too much stock in this until it is repeated and more carefully described. If you notice they don’t correlate dose or dosing interval with lines in the figure.
I assume “no rebound” is daily dosing and several subjects they did 4 hour dosing on and “rebound” is weekly dosing but we really don’t know. .Also, most subjects did not rebound within 7 days. That makes me think the higher doses were the “non rebounding” doses at 7 days because they still had high enough blood levels to suppress mTOR. Lower doses perhaps began to rebound as they hit about 7 days and the blood concentration of rapa dropped off. This would also make sense in light of they only looked at P70S6 kinase activity in sirolimus only subjects and not in the cohorts that took GFJ and keto. Supplemental Table 2 shows 40 subjects in the sirolimus only group, were these subjects (shown in Fig 2B) cherry picked or were they the only ones they did P70S6 kinase activity studies on? I count 9 total subjects in Figure 2B.
Whenever authors leave out the details like this it often is because the data doesn’t make sense and perhaps some randomly rebounded both high and low dose or because perhaps their assay for phosphorylation had high variability. We need error bars and more subjects per dosing group to make any sense of this. It really shouldn’t have gotten past review.
MTOR rebound seems it would only be highly detrimental to cancer patients. Remember that as we get older our MTOR operates at higher and higher levels naturally. We take Rapamycin to shut MTOR down so that our AMPK pathway can stimulate autophagy.
So, an MTOR rebound would have your MTOR system operating higher before lowering to a normal state. I can’t see how this is bad since you get the AMPK autophagy stimulation that you were unable to get before by taking Rapa.
@destrider. Good points. I’m not saying rebound is good or bad, just that we don’t really know what dosing intervals and levels it happens in. It seems some want to change dosing or dosing intervals to prevent it but the paper reporting it is vague and poorly describes the phenomenon. I’m not even sure it is real.
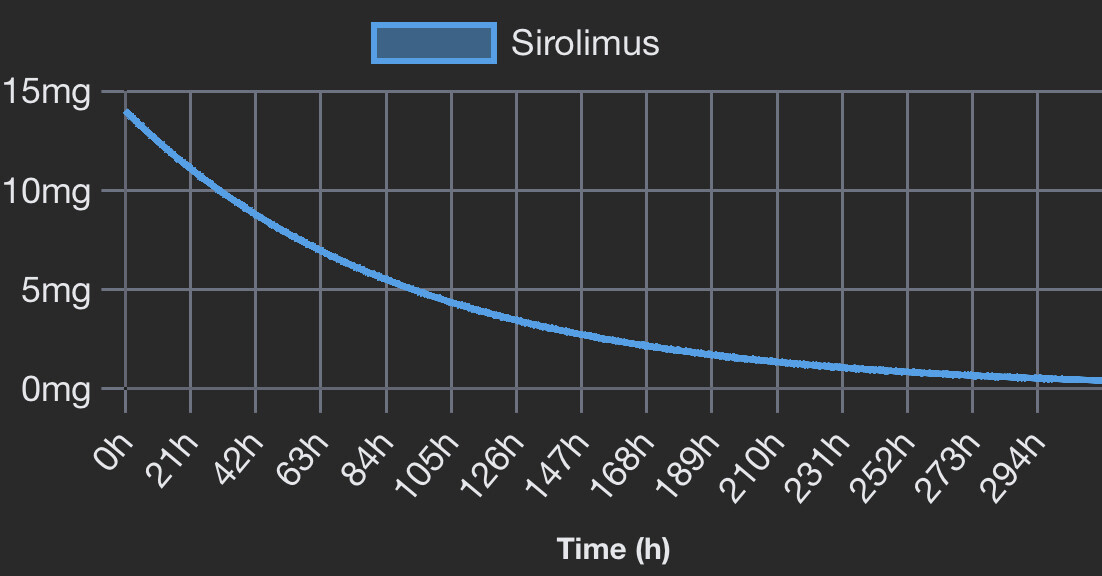
I have been taking 12mg once every two weeks.
My last measured neutrophils have become rather low so am taking a 4-6 week break.
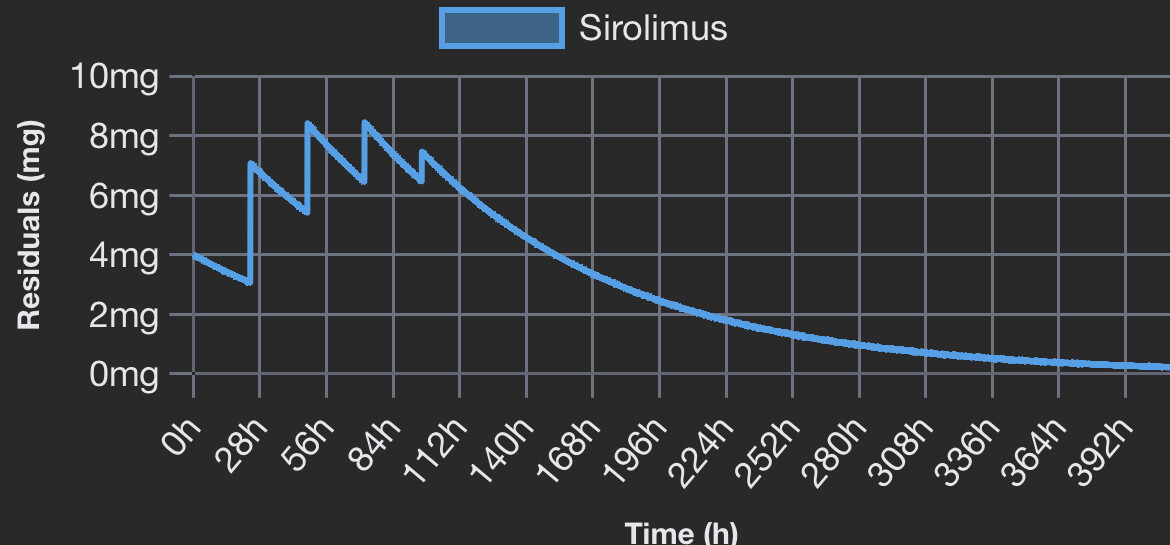
When I come back to it I’m going to try taking over 4 days 4mg, 3mg, 2mg & 1mg, again once every two weeks.
I have no idea if it will work at mitigating an mTOR rebound but I think it’s a good combination that keeps an element of the higher dose pulsing regimen.
Furthermore, if Rapa is a CR mimetic and autophagy is potentially more likely the longer one is doing CR then this could also be beneficial in that respect.
Maybe the important question is: what causes the rebound? Dose amount, duration of therapy? Both? My guess is that duration of exposure to Rapa is most important. Something I definitely don’t have a handle on yet,
Seems to me that since rapamycin extends the lifespan of all organisms tested so far, I have a hunch the rebound probably doesn’t affect the primary outcome–lifespan–very much in otherwise healthy subjects.
Glad to see the discussion ongoing with people reaching out to experts.
Many questions here for sure.
We know that rapamycin extends lifespan of all test organism thus far but to my knowledge it has always been at a daily dosing interval and surmise with no rebound.
I don’t think I have seen a paper with weekly dosing AND extension in life in test animals. What most of us targeting here is lifespan, not a response in immune response to a vaccine.
That being said, we don’t know if the rebound is bad in a setting of intermittent suppression. It is an unknown. But most us would surmise that prolonged elevated phosph-p70s6k from mTor stimulation is not optimal.
Secondly we don’t have a data set on “healthy” active people.
I wouldn’t be surprised if someone on this forum did not have the ability to test for phospho-p70s6k.
What I’d like to see is this study reproduced in healthy people and try to ascertain if there is a schedule that results in no rebound.
Characterization of the rebound would also prove to have utility. I doubt (hope) the rebound is permanent.
Lastly, ~ 50% had no rebound so Fortis Fortuna Adiuvat ¯_(ツ)_/¯
The Mannick study was targeting immunosenescence, the decline in immune function with age. So by improving vaccine response even after a two week break suggest there was a possible reversal of age?
My interpretation of the Mannick Study was that the response to the vaccine was improved with the intervention.
However, an improvement to a vaccine does not prove possible reversal in age.
We don’t have long term data with this schedule.
All we have on long term is with animals with a daily schedule.
But in a setting where the aforementioned data exists (rebound in humans); when our underlying assumption is suppression is optimal, it does make me pause.
I don’t see that much of a problem of daily dosing at 0.5 mg whole tablet, however none of the longevity experts or prominent people do daily dosing as far as I know, that’s why I am at least hesitant. If we could get one of those a comment on this information.
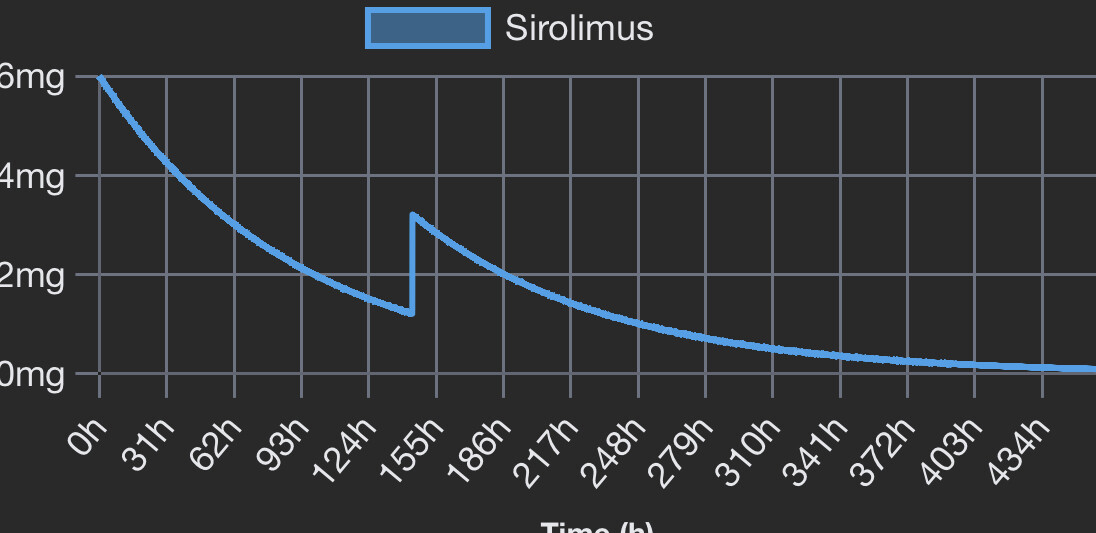
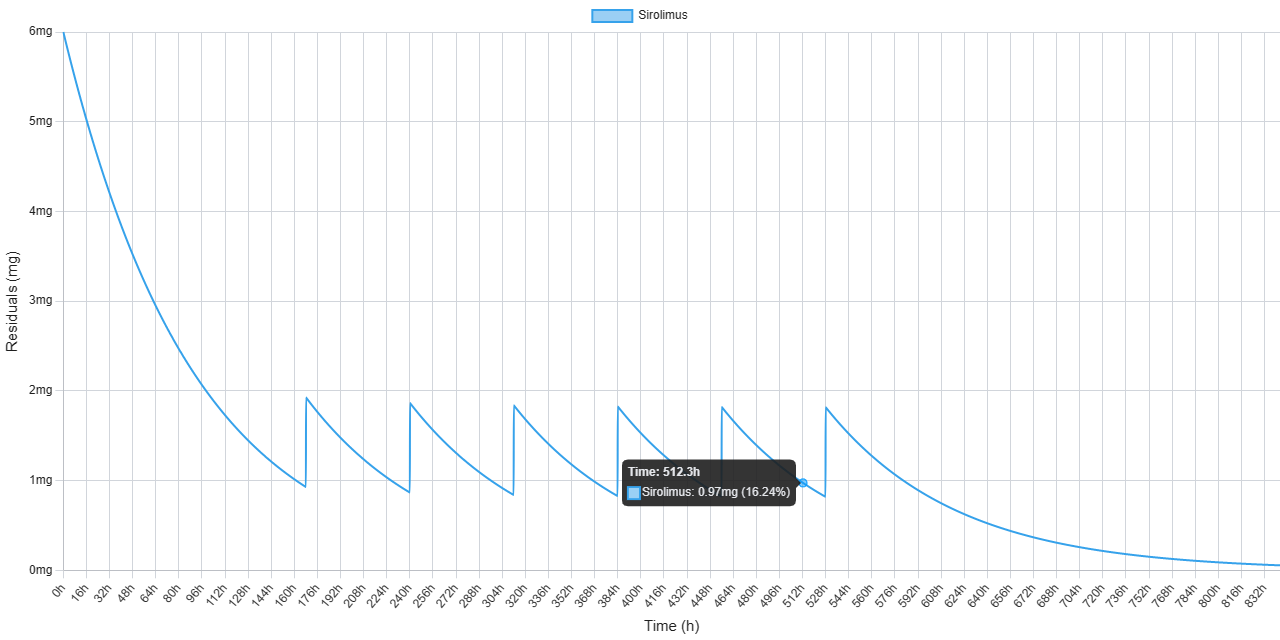
Thanks for a great calculator. @Leonard It makse it easy to see what I am considering. One potential low dose regimen I am playting with is: 6 mg once and then wait for one week and then every third day, take 1 mg.
@ Curious, I really don’t have a clue, but my gut feeling is that your regimen would hinder the rebound more efficiently than DeStriders regimen… he could be timing his second dose just perfectly, but I feel that earlier and over several days would be a safer rout, given how little we know at this point… but who knows both variants should at least be better than a single dose.
For anyone who trains a lot, and care about gains and recovery, one or to dosing might be more advantageous.