Well, that could explain my statin intolerance
But now that I have Bempedoic Acid, there’s no reason to run back to Rosuvastatin. Thanks for the info though!
I have been taking rosuvastatin every other day (10 mg) and alternating it with 5mg ezetimibe. Yesterday Ivreached the point that all my muscles started hurting, especially in the legs. It’s the point when I have to discontinue statins and have a long break to heal. It happens every time when I try a statin. I already tried all of them. Cannot wait to hear how bemp acid going for you. May be I’ll be switching as well.
Try 2.5mg / day. I personally take Ezetimibe 5mg + rosuvastatin 2.5mg daily.
“the lowest dose of rosuvastatin that is marketed, 5 mg, reduces LDL-cholesterol by 45% on average, still more than initially necessary for many patients.
Not mentioned in the recent ATP3 guidelines4 is the fact that 2.5 mg and 1 mg of rosuvastatin reduce LDL-cholesterol by an average of 42% and 34%, respectively”
I was actually one of the members of the team that did the due diligence on rosuvastatin/crestor before we bought it off Shionogi….actually we may have done a swop for marketing rights, come to think about it.
Nice info. I’m already down to 5mg rosuvastatin EOD. And now Eze 10mg tabs I split in two. Pretty soon I’ll be a believer in shadows of molecules (homeopathy). …kidding. I’m am grateful for learning how to shrink my chemical load.
So far Bempedoic Acid has been great. We’ll see how that affects my cholesterol in about 3 months when I have a full checkup. I postponed my checkup so I could capture the effects of Bempedoic Acid as that is the most meaningful intervention I have introduced.
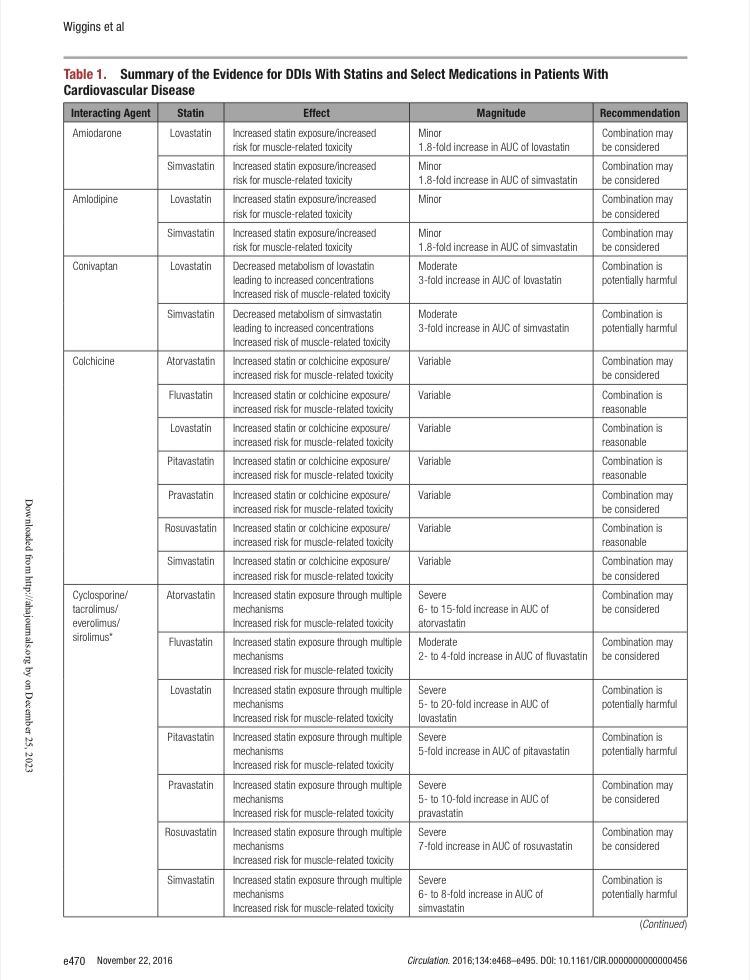
I’ve been taking 10mg Ezetimibe daily for months now with no negative effects at all. I do get some minor muscle aches from Atorvastatin but thankfully not enough to put me off taking it. That is very useful information about the massive increase in AUC with Rapamycin, especially since I’m on 80mg Atorvastatin daily. I might drop to 0 or 20mg on Rapa days going forward. I was dropping to 60mg if I took GFJ with the Rapa but that kind of multiplier is really quite scary.
I was taking Ezetemibe before but have stopped when I switched to Bempedoic Acid. I want to see the effects of BA on my cholesterol by itself. If it is still a problem, I will add Ezetemibe back in later.
The reason is because Ezetemibe may block the absorption of my Omega 3 supplements, and I want to find out if it does for me. So I am getting a baseline with BA first.
However, these established elevations are demonstrated with cyclosporin not necessarily with mTOR inhibitors with the latter having limited data available for them (as mentioned in that table asterisk).
There was a segment in this article about mTOR inhibitors, Which they recommended at the end to be treated the same way as cyclosporine but this seemed to be guided by the precautionary principle rather than strong evidence. The three studies they cited for their concern:
Once they switched from cyclo to siro while still taking mycophenolate with/without steroids (they had double the rate of myopathy but mostly asymptomatic elevation in creatine kinase and only in pravastatin not atorvastatin).
The second one was a case of rhabdomyolysis while taking fluvastatin when switching from cyclo to siro with the patient still being on Myco and steroids, But in the article, they acknowledged that this was possibly due to sepsis the patient had altered liver metabolism
In the third one, the patient developed severe rhabdomyolysis while taking siro + tacro + simvastatin, But he already experienced a liver rejection recently and renal dysfunction
The only study where they specifically and cleanly tested the pharmacodynamics interactions of concomitant statin and mTOR inhibitor administration in healthy people was done with everolimus (which is the closest one to sirolimus) and atorvastatin and pravastatin, And there was no statistically significant difference in either AUC or Cmax.
While the interactions need further detailed studies, There is no current evidence to indicate a relevant or clinically meaningful interaction of sirolimus (or everolimus) in healthy individuals.
While academically interesting. None of the above actually changes how statin should be monitored. Everyone should get a baseline CK (and LFTs) measurement before statin initiation and CK to be repeated if the patient experiences muscle aches/weakness (From what I know there is no compelling evidence to continually measure CK if the patient is asymptomatic with the statin)
Wow, that’s a relief! In light of that final study I shall continue to reduce Atorvastatin to 60mg on Rapa dosing days with grapefruit. I figured that I usually have the grapefruit around 8am, the Rapa around 10am and then the slightly reduced statin dose around 11pm. I figured most of the grapefruit effects would have dissipated in that time frame.
Very interesting to hear about the possible interaction of Ezetimibe and Omega 3. I have done a little digging and I could only find a couple of references to this (one was at Manitoba University and the server was down). It’s particularly annoying because it would appear that Ezetimibe has a very long half life which is extended further when used in combination with some statins (including Atorvastatin) so it doesn’t even appear possible to spread out the Omega 3 and Ezetimibe dosing to mitigate the interaction.