Higher dose of Rapa, despite side effects to ensure impact on all tissues including CNS.
Lengthen dosing interval to allow resynthesis of mTORC2.
Fast after Rapa dose to avoid competing stimulation of mTORC1
Stop anabolic supplements around Rapa dose.
Reconsider need for senolytics as Rapa may do that.
Gonna look at process as:
Take Rapa to catabolize and then let body rebuild better.
this was an excellent summary. Very useful and important. BTW, anecdotally I had switched to 10mg+GFJ+EVOO and I felt amazing, so in a way I was ahead of this podcast. I doubt you’ll encounter any side effect of very high dose, since I had none when I switched from 5mgs to 10mg (at 5mg i almost always had either small infections or mouth sores). An infection on my left forearm that had lingered for about 4-5 weeks cleared literally the next day i did the 10mg dose, in its own no other remedy. But that is clearly one of your summary point above where the intermittent dosing is an immune rejuvinator.
I listened to the podcast on Rapamycin with Dr. Attia, Sabatini and Kaeberlein. It’s interesting and concerning that David Sabatini is reluctant to take Rapamycin. He decided to wait until 2026 when the Dog Progect is completed.
It’s also clear that nothing is certain about many aspects of longevity and Rapamycin yet.
so are you thinking of every 10 days or two weeks instead of weekly?
On a somewhat related topic, Dr. Blagosklonny recently tweeted that “he is winning” so that is very encouraging.
Not sure. Maybe every 2 weeks or even monthly? The only thing I’m sure of is that nobody know the right answer. I’m thinking brief periods of catabolism/autophagy followed by longer periods of repair.
Guys I saw many more takeaways to the interview. For anyone gulping at the 3 hour length, I recommend you watch it at 1.5-2x speed on YouTube that way you’ll gain at least 1-1.5 hours of life expectancy regardless of your rapamycin regimen
put more stock in life extension studies performed on organisms far removed from us in the evolutionary family tree: apparently the genetic mechanisms of lifespan extension are highly conserved across most species — I used to take results in rats or C. Elegans with a huge grain of salt. From now on I’ll just sprinkle a tiny bit.
the rapa probably isn’t getting to the central nervous system due to its extremely high lipophilia. In all likelihood, to get it across the blood brain barrier you need high continuous doses, every 8 hours for a few times, not letting the trough level get too low for a while. It almost needs to be pushed through. For older folks though who have an impaired blood brain barrier getting it up there might be naturally easier. Some food for thought there on how to schedule dosages.
more details on how mTORC2 gets inhibited. The thinking being that even mice who were fed rapa DAILY in the studies were technically on an intermittent pulsed dose because they only ate every so often. It wasn’t in their blood stream / intracellular fluid constantly. And it takes mTOR connecting to RAPTOR just once for mTORC2 to form. Once it’s formed rapa can’t inhibit it. It only directly inhibits mTORC1 (but also binds to mTOR so if it catches ALL free mTOR then there won’t be any possibility for mTORC2 to get formed, but this sounds like an extreme and unlikely scenario). My takeaway here is that even daily doses are probably fine, so long as there’s some washout periods intermittently to make sure all the rapa is eventually cleared.
they mention a study whose details they can’t recall on the spot but say they wish they could, re: mTOR hypomorphic alleles, to get to the tissue specific effects of mTOR inhibition. I found the study in question and it’s fascinating (https://www.sciencedirect.com/science/article/pii/S2211124713003926) These mice have genetic mutations that make them express less mTOR, about 25% of the mTOR of wild type phenotype controls. And… they have a much higher life expectancy and max lifespan than control. This would be almost the equivalent to getting rapamycin in their blood stream continually since they were embryos, basically no intermittent dosage even compared to daily feeding. It is SUPER interesting though because mTORC2 is proportionally lowered vs mTORC1 here, they’re both at ~25% normal values because their precursor mTOR is itself lowered by that much. And here we have a MUCH higher percentage of the lower mTOR mice DIE prematurely of infections compared to the controls. So that’s a fat tail distribution of life expectancy with many dying younger due to infections and yet many others dying of extreme old age. I’m not sure if they removed those early deaths from the averages of life expectancy so not sure if the tradeoff was worth it to the mice, statistically speaking. Maybe you can sort out the weeds of the data in the study and let me know. On the flip side of more frequent and severe infections, the lower mTOR mice significantly fewer tumors. Basically at some point if you have constant inhibition of mTOR and consequently of mTOR2, you’re likely much more immunologically vulnerable: immunomodulation slides into immuno suppression. Also super interesting that not ALL tissues get rejuvenated or aged slower with suppressed mTOR. Most did — in these mice — but bone degeneration happened FASTER and so did cataracts. I’m very keen on getting the story straight Re: bones as rapamycin seems to help fight osteoarthritis and osteoporosis based on my limited research but there may be a dose depended U shaped response or something trickier going on. I’ve noticed that the modality I’ve researched ad nauseam, PEMF, which has solid evidence as far as I’m concerned for promoting osteoblast activity, increases mTOR expression in the bones.
speaking of tricky tissue specific effects, there was a caution Re: sarcopenia because mice don’t develop sarcopenia like humans do. So just because rapa in mice doesn’t seem to accelerate sarcopenia in their old age it doesn’t mean we can take the corresponding result for granted in humans. On the one hand, we have @Agetron and others rocking their muscle building while on rapa. On the other hand, they ain’t that old so a note of caution there.
the dosage we’re taking on this forum is probably on the low end of the likely effective (or optimal range) according to the experts here. Their biggest concern Re: ongoing dog study is that they’re dosing way too low (the equivalent of 6-8g / week for average sized humans if we scale linearly based on body mass). Even so they’re seeing some positive noise so far.
the known rapalogs are BS molecules not in any way superior to rapamycin and purely fabricated for regulatory capture purposes, to reset the clock on the pharma patents.
rapa seems to work best at slowing down the cell cycle and seems to benefit the most those cells that reproduce slowly. Different effects in fast reproducing cells. That might explain why it seems to help female reproduction but hamper male reproduction (at least while actively being administered).
autophagy and lowered systemic inflammation seem to be the main pathways these two believe rapa is working its magic through. We have great biomarkers for inflammation but not for autophagy. Hint: other meds / modalities that lower sterile inflammation might lead to life extension benefits. I’m thinking of LDN off the top of my head.
a bunch more but I forget. Do yourself a favor and watch the whole thing at 1.5x speed.
A few interesting observations re: Dramamine, apparently an mTORC1-specific inhibitor, made the more interesting based on points 2 and 4 above:
I’m taking AKG too. My stack is one well diversified portfolio.
But you know what I mean, sarcopenia might not become a real issue for someone who’s in shape until he or she hits mid 70s or 80s. My dad is 72 and he seems to have experienced a decline this past few years that I didn’t see coming even 5 years ago.
I’m about 2/3 through it. I never watch podcasts (no patience/focus for sitting and watching) - I’ve been listening in my car. At 1.25 speed like I do for all podcasts.
Yeah, it’s interesting that David Sab still won’t (admit?) to taking it. However, Joan M is in that camp too.
Even though many aren’t a fan of David Sinclair, I think him stating that he now takes Rapamycin is HUGE news. I say this due to his reservations that he stated in the Lifespan podcast. For him to have changed his view is big!!!
Thanks for the comprehensive post @medaura! I haven’t made it the whole way through yet but also reflected on the above.
If I was to reconcile the mouse study regarding CNS and extrapolate that to humans, then maybe a two to three day dosing protocol of 4-6mg (??) might be necessary every 3-4 months (then a pause for 2 weeks). This would be interspersed with a ‘normal’ protocol of 5/6mg once weekly….
I should state that I’m purely speculating based on what I’ve heard on the podcast thus far and have no literature to back this up.
Also I couldn’t tell if during their talk they make any dose equivalency adjustments based on animal metabolism and the rate at which they break down rapa. I saw a very informative chart from @RapAdmin the other day, maybe he can post it here too, laying out some rules of thumb for metabolic rate adjustments.
I really enjoyed the interview and am glad I had the extra time to listen. I especially appreciated the simple analogy of rapa being more like a round volume dial rather than an on/off switch for TOR1.
When I first started taking rapamycin I started taking high doses based on some of my readings and Dr. Blagosklonny’s comments on dosing.
I actually took one 20mg dose of rapamycin with GFJ before and with, based on the knowledge that no one had ever died from an overdose, in order to get some into the brain.
I experienced some diarrhea with the dose so I titrated down. By the time I got to doses I could tolerate without side effects such as increased glucose levels and diarrhea, they were at levels unlikely to cross the blood-brain barrier.
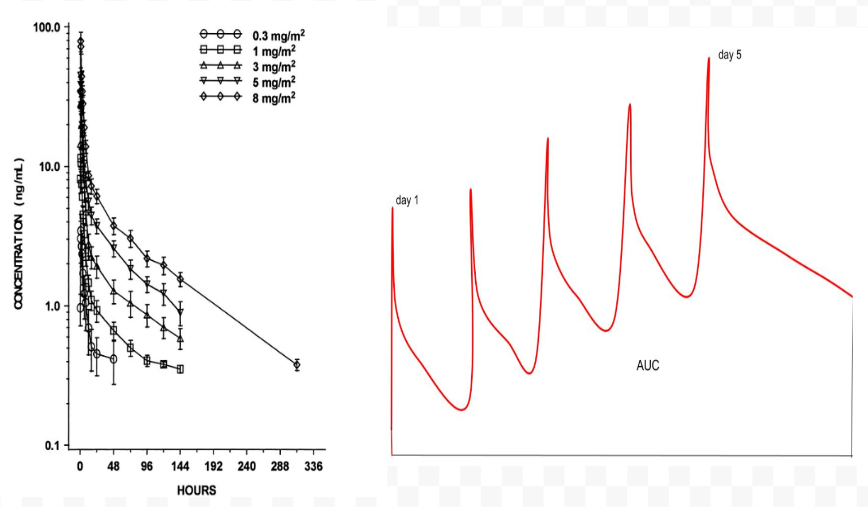
My current experiment is to take rapamycin daily for 5 days then 9 days off. I started with 1 mg daily. Now I am at 2 mg daily. So far I have felt no side effects such as diarrhea or sleep problems. I have not had any blood tests since I tried this protocol, but I will soon.
I don’t plan on taking rapamycin every 8 hrs.
“to get it across the blood brain barrier you need high continuous doses, every 8 hours for a few times, not letting the trough level get too low for a while. It almost needs to be pushed through. For older folks though who have an impaired blood brain barrier getting it up there might be naturally easier.”