My choice is 6-8 mg weekly. Seems to be working …
Consistent great biological age benefits at this dose.
7 Likes
Have decided to restart Rapamycin, after reading that powerful study on 1 mg/day for 4 months on humans. I quit Rapa because of side effects mainly lower lymphocytes, but maybe the lower dose, though chronic, will give less or no side effects than the higher peak of my weekly 3 mg dose.
The study showed no significant differences in leukocyte counts between treated and placebo, suggesting that the daily 1 mg was not immunosuppressive. Disappointingly, lymphocytes and NLR were apparently not measured.
4 Likes
Ok so it’s now March and I think I’m starting to notice slight immunosuppressive effects. I very rarely get sick but lately I’m catching all the sniffles — no major sickness or symptoms but things that wouldn’t touch me at all as they pass around the house are definitely taking their time with me too. At first it looked like just seasonal noise but now it’s clear that there’s a pattern. But it’s been three months and really I could push it if I wanted to but I don’t see any good reasons to.
So washout time for me. Followed by 6 mg/week for a good stretch TBD.
4 Likes
I haven’t been sick in a few years. Not since I have been taking Rapamycin
4 Likes
Hmm. Seems like there must be individual variation in reaction. FWIW, the Mannick study seemed to show that everolimus at a reasonable dose (5mg/1-week) results in enhanced immunity and fewer respiratory infections (at least viral). If the same holds for the extremely similar molecule of rapamycin, then one would expect fewer viral infections in general, but as you show, this is not true for everyone. As I very rarely get respiratory infections (no kids, ![]() ), I haven’t noticed the impact of rapa on this either way. You are doing the right thing in taking a break. Speaking just for myself, I’ve always been very cautious in making connections between a drug and some symptom, and even so, I’ve still managed to get it wrong recently (which I will describe one day in a post as a cautionary tale… where I wrongly ascribed arm and scapula pain to bempedoic acid, when in reality it was just a series of coincidences) - however others are likely more observant than me, so that may not be relevant to anyone else.
), I haven’t noticed the impact of rapa on this either way. You are doing the right thing in taking a break. Speaking just for myself, I’ve always been very cautious in making connections between a drug and some symptom, and even so, I’ve still managed to get it wrong recently (which I will describe one day in a post as a cautionary tale… where I wrongly ascribed arm and scapula pain to bempedoic acid, when in reality it was just a series of coincidences) - however others are likely more observant than me, so that may not be relevant to anyone else.
2 Likes
I was taking 1mg/day since early December.
1 Like
That seemed fine in the Mannick study protocol. LaraPo has more experience with this protocol. I’ll just point out that 1mg/day is a higher cumulative dose than most here use 6mg/1-week, because you end up with 7mg a week, and if you take no breaks, it’s possible you accumulate without a trough. Nothing wrong, just a different modality. I wonder if you wouldn’t have been happier with 6mg/1-week. YMMV.
2 Likes
I will be following Steve´s one mg/day with a break every fourth week.
1 Like
Anything to report on from your protocol?
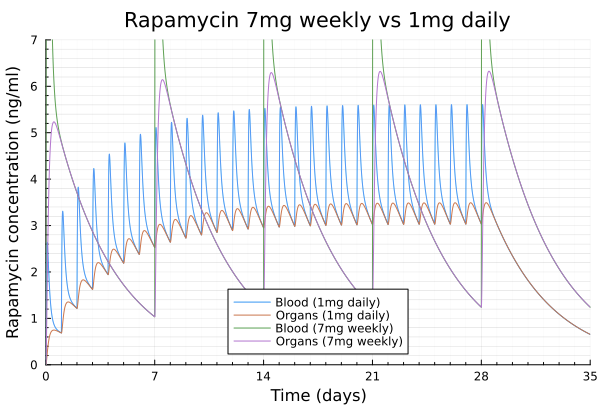
Here is a comparison of rapamycin 7mg weekly vs 1mg daily.
It takes around 10 days to reach 3ng/ml at 1mg/day.
Interestingly the 7mg/week (same weekly dose) also reaches the same 3ng/ml average but has half of the time way above or below that limit.
Basically people could do 1mg/day for 10 to whatever they want followed by a washout period to adjust the ratio of time spent around 3ng/ml.
BTW Note this has been done with the model fitted with my own blood concentration measurements so there will be some individual variability.
4 Likes
No issues, should be getting my annual blood panel done soon.
Everything is pretty normal ![]()
When taking 1mg daily, do you simply take it with your other supplements and drugs at the same time in the morning? I wonder about potential interactions, but also worry that daily use can have a negative impact on muscle gain.
2 Likes
Yes I’ll switch to weekly after some brief washout. The subjects in the Mannick study were older males too. Their mtor was probably at a higher baseline and needed more aggressive dampening. I’m almost 40, 5 foot 3 in the shade, low growth phenotype, very low baseline inflammation. Might have gone past the sweet spot. It’s also possible my back to back sniffles were a coincidence I attributed to rapa but it’s unusual for me and why risk it? I will go back to daily dosing later this year for a few months or as long as I’m doing fine on it. Glucose never budged so I don’t think I was experiencing any meaningful mtorc2 suppression. Just starting suspecting some immunosuppression so time to switch it up.
4 Likes
Same…it’s quite extraordinary.
1 Like
Single-dose rapamycin increases brain glucose metabolism but reduces synaptic density in Long-Evans rats My thought is that [18F]SynVesT-1 imaging should probably be included in future human studies, if [18F]SynVesT-1 is cleared by FDA for human administration. The rapamycin dose was relatively high, 8mg/kg intraperitoneally, probably to achieve brain penetration.
4 Likes
This is discussed here: Extremely High Dose Rapamycin Boosts Brain Energy but Prunes Synapses In Vivo
Note: they used the equivalent to approx. 90mg dose of rapamycin in humans.
1 Like
I think getting sick or not depends on your exposure. If you take public transport or frequent hospitals and you take Rapamycin, you’ll probably be a lot sicker than if you stayed at home in isolation and take Rapamycin.
1 Like
Yeah, and it’s also massively dependent on what’s going on with the rest of the population. Like during Covid lockdowns, flu and everything went down, and when lockdowns ended they came back with a vengeance.
Definitely! When you see these results in studies, they are almost always reporting mean values. But if you have human subjects who aren’t clones, you’ll have a wide range of responses for almost anything. Like, I’ve seen strength training studies where people do a 12 week program with coaches, protein supplements, and end the 12 weeks weaker or having lost muscle, whereas some pile on the gains. There’s huge individual variation - probably larger than we’d like to believe IMO.
In the Mannick study (attached), figure 1 doesn’t even have error bars.
2014 - Mannick et al. - mTOR inhibition improves immune function in the elderly.pdf (322.7 KB)
Table 2 reports percentages of people who sero-converted, and the best immune-boosting benefit of Rapamycin was going from 16% in placebo up to 40% in Rapamycin. But that still means 60% of people taking Rapamycin didn’t hit the seroconversion target. And that was the best paired comparison. Others were 17% to 22%, 17% to 27% etc.
And looking at antibodies (Figure 2), they were reporting a 1.3-fold increase in the 5mg/w group. Statistically significant but hardly a massive change. But I’m sure there were a wide variety of responses.
2 Likes
I asked AI if there is a reason that 4 months was chose as the study length
Why was 4 months chosen as the duration for this study?
4 months was chosen as the treatment duration based on a calculated compromise between human immune cell kinetics, biomarker stabilization, and clinical trial safety protocols.
Longevity investigators utilize this specific timeline for several precise reasons:
1. T Cell Lifecycle and Population Turnover Dynamics
Human T cells are not static; their populations shift dynamically through naive, memory, and senescent states.
- Prior Consensus: A temporary, brief pulse of rapamycin (e.g., 2–4 weeks) might only alter the immediate activation status of existing circulating cells without fundamentally changing the baseline cellular makeup of the immune system.
- The 4-Month Rationale: Four months allows enough time for homeostatic peripheral expansion and turnover. This duration ensures that the investigators are measuring the markers (like p21 and p53) on a refreshed pool of immune cells that matured or persisted under continuous, low-dose mTOR inhibition, rather than cells that carried historical, unmitigated DNA damage from prior months [Confidence: High].
2. Kinetic Resolution of Senescence Biomarkers (p21 Suppression)
Unlike immediate upstream signaling elements—such as Phospho-S6, which downregulates within hours of taking rapamycin—downstream markers of cellular senescence do not shift instantly.
- Mechanism: The protein p21 is a stable, long-term mediator of cell-cycle arrest induced by chronic DNA double-strand breaks.
- The 4-Month Rationale: To definitively prove that rapamycin has an in vivo senomorphic and genoprotective effect rather than just temporarily masking inflammation, the trial needed a multi-month window. This allowed senescent T cells to naturally undergo clearance or experience a fundamental downregulation of their internal damage-response programming, creating a measurable, statistically significant delta between the active and placebo groups [Est. Probability: ~85%].
3. Safety Window for Capturing Adverse Off-Target Effects
From a clinical safety and trial design perspective, short durations (like 30 days) often fail to reveal the slow-onset metabolic and hematological side effects unique to chronic rapamycin administration.
- Off-Target Risks: The primary risk of daily human low-dose rapamycin is the gradual, passive inhibition of mTORC2 (which can drive insulin resistance, dyslipidemia, or mild leukopenia/neutropenia).
- The 4-Month Rationale: Four months is widely recognized in human experimental medicine as the “sweet spot.” It is long enough to confidently declare a protocol metabolically and immunologically safe if no adverse blood panel trends emerge, yet short enough to protect older volunteers from long-term toxicity if a negative trend does manifest [Confidence: High].
4. Historical Precedent in Immunosenescence Trials
The 4-month timeline aligns closely with pioneering clinical trials in the field of mTOR-targeted immunosenescence. Dr. Joan Mannick’s landmark 2014 and 2018 RAD001 (everolimus/rapamycin analog) trials utilized 6-week and 2-month dosing windows followed by washouts to test vaccine responses. By pushing this trial to 4 months of continuous usage, the research team sought to validate whether the immune-enhancing, genoprotective benefits could be sustained safely over a prolonged seasonal period without inducing systemic immunosuppression.
Rapamycin enhances resilience against DNA damage in the ageing immune system | Loren Kell
Loren Kell, the first Melon Scholar, presents her pioneering research on how rapamycin and mTOR inhibition enhance resilience against DNA damage in the ageing immune system. Drawing on four years of work spanning in-vitro assays and a clinical trial in older adults, Loren explains why immune ageing—driven by DNA damage, impaired T-cell function, and cellular senescence—is one of the greatest challenges in longevity science. She demonstrates how low-dose mTOR inhibitors reduce DNA lesions, suppress senescence markers, and improve immune cell survival, offering powerful insight into how these therapies could bolster vaccine responses, protect against genome instability disorders, mitigate radiation exposure, and even support human health in space.

I. Executive Summary
Immunosenescence, the progressive age-related decline of the immune system, compromises vaccine efficacy, diminishes resilience to novel pathogens, and elevates the incidence and severity of malignancies. A central driver of this phenotype is the accumulation of un-repaired genomic instability and double-strand DNA breaks within peripheral immune cells, particularly T-lymphocytes. This persistent genotoxic stress triggers the DNA damage response (DDR) pathway—characterized by the upregulation of gamma-H2AX, p53, p21, and p16—ultimately forcing healthy proliferating cells into a state of permanent cellular senescence. Senescent immune cells exhibit morphologic enlargement, metabolic disruption, and a pro-inflammatory secretory profile that compromises systemic tissue homeostasis.
Emerging research identifies a critical functional intersection between genotoxic stress and the mechanistic target of rapamycin (mTOR), an intracellular nutrient sensor that is chronically hyperactivated in aged and senescent immune lineages. While clinical evidence has established that low-dose mTOR inhibition can rejuvenate immune function and enhance vaccine responses in elderly populations, the underlying molecular mechanisms have historically remained obscure. Recent investigations clarify this relationship, demonstrating that high levels of DNA damage directly correlate with elevated mTOR signaling in human T-cells.
Experimental models utilizing human peripheral blood mononuclear cells (PBMCs) exposed to the radiomimetic agent zeocin demonstrate that first-generation mTOR inhibitors (rapamycin) and second-generation catalytic inhibitors (AZD8055) suppress DDR signaling and reduce the expression of downstream senescence effectors. Crucially, single-cell gel electrophoresis (comet assays) confirms that rapamycin treatment actively reduces the physical burden of nuclear DNA lesions rather than merely dampening checkpoint signaling. This genoprotective action translates to a threefold increase in cell survival following severe genotoxic insult.
Human clinical data validates these in vitro findings. A randomized, placebo-controlled trial evaluating a low-dose regimen of 1 mg daily of rapamycin over four months in an older cohort achieved steady-state blood concentrations of approximately 4 nM. Ex vivo analysis of these participants confirmed a simultaneous reduction in both mTOR hyperactivation and endogenous DNA damage markers, alongside significant suppression of the senescence marker p21 across multiple immune subsets. Consequently, targeted mTOR inhibition represents a viable therapeutic strategy to enhance genomic resilience, offering translational utility for physiological aging, clinical radiation exposure, spaceflight-induced genotoxicity, and congenital DNA repair deficiency syndromes.
II. Insight Bullets
- Definition of Immunosenescence: Characterized as the chronological aging and functional decline of the immune system, resulting in compromised adaptive and innate immunity.
- Clinical Manifestations of Immune Aging: Manifests clinically as decreased vaccine efficacy, reduced resilience against novel pathogens (such as SARS-CoV-2), and increased malignancy incidence and severity.
- Lineage-Specific Immune Dysfunctions: Aging drives distinct pathology across cell types, causing B-cells to fail in antibody production and inducing proliferative blocks and lineage leakage in T-cells.
- DNA Damage as a Primary Driver: Persistent accumulation of double-strand DNA breaks directly accelerates the onset of immunosenescence and drives systemic immune system decline.
- Mechanisms of Cellular Senescence Induction: Healthy, proliferating immune cells exposed to continuous genotoxic or environmental stressors cross a threshold into permanent cell-cycle arrest or apoptosis.
- Morphological Hallmarks of Senescence: Senescent cells undergo significant structural alterations, including marked physical enlargement visible during in vitro visualization.
- The DNA Damage Response (DDR) Cascade: Severe genotoxic stress activates a highly regulated signaling cascade mediated by checkpoint proteins to halt cellular division for repair.
- Gamma-H2AX as a Double-Strand Break Marker: Phosphorylated histone H2AX (gamma-H2AX) serves as a sensitive, quantifiable metric for tracking double-strand DNA breaks within single cells.
- Role of the p53/p21 Axis: Genotoxic pathways upregulate p53 and its downstream target p21 to enforce cell-cycle arrest, particularly in damage-induced senescent states.
- Oncogenic Protection Trade-off: Cellular senescence operates fundamentally as an evolutionary defense mechanism to halt the replication of cells harboring severe genomic mutations.
- Phenotypic Enrichment in Age-Expanded Subsets: Multi-parametric spectral flow cytometry proves that senescence markers selectively cluster within the specific immune subpopulations that expand most during human aging.
- mTOR as an Aging Nutrient Sensor: The mechanistic target of rapamycin (mTOR) coordinates cellular metabolism and exhibits pathological hyperactivation within senescent cell populations.
- Lineage-Specific mTOR Hyperactivation: Chronologically older cohorts display pronounced baseline elevations in mTOR activity (measured via phosphorylated S6 ribosomal protein) selectively inside T-lymphocytes.
- Historical Clinical Efficacy of mTOR Inhibition: Prior large-scale human clinical trials demonstrated that transient, low-dose mTOR inhibition safely enhances antibody and T-cell responses to influenza vaccination in elderly cohorts [Mannick et al. - Source unverified in live search].
- Preclinical Immunosenescent Rescues: Genetic mouse models deficient in immune DNA repair mechanisms recapitulate human immune aging, a phenotype partially reversed through rapamycin administration [Kell et al. - Source unverified in live search].
- Establishment of Human In Vitro Genotoxic Models: Human peripheral blood mononuclear cells (PBMCs) treated with zeocin or hydrogen peroxide provide a reliable model for inducing and studying double-strand DNA breaks.
- Correlation Between DNA Lesions and mTOR Activation: Single-cell fluorescence profiling reveals a direct, positive correlation between the magnitude of intracellular DNA damage and the degree of mTOR activation.
- Chemical Attenuation of DDR Markers: Co-treatment with rapamycin or the second-generation catalytic mTOR inhibitor AZD8055 suppresses the expression of gamma-H2AX, p53, and p21 following genotoxic insult.
- Verification via Single-Cell Gel Electrophoresis: Comet assays confirm that rapamycin actively prevents the physical formation or persistence of nuclear DNA lesions rather than simply blocking downstream protein phosphorylation.
- Profound Survival Advantages Under Genotoxic Stress: Human T-lymphocytes treated with rapamycin during severe zeocin exposure demonstrate a threefold increase in survival compared to untreated damaged controls.
- Translation to Low-Dose Human Protocols: A clinical trial using a daily low-dose regimen of 1 mg of rapamycin for four months successfully validated the physiological safety and tolerability of chronic mTOR inhibition in older populations [Atherton & Wilkinson - Source unverified in live search].
- Achievable Therapeutic Pharmacokinetic Windows: The 1 mg daily human dosing protocol achieves a steady-state blood concentration of 4 nM, directly corresponding to effective mechanistic concentrations identified in vitro.
- In Vivo Reduction of Endogenous Genotoxicity: Older human participants treated with low-dose rapamycin demonstrated a significant reduction in endogenous baseline DNA damage within circulating T-cells.
- Systemic In Vivo Downregulation of p21: Chronic low-dose rapamycin administration suppresses expression of the cell-cycle inhibitor and senescence marker p21 across multiple circulating immune lineages.
- The Concept of mTOR Inhibitors as Genoprotectors: These collective data establish a previously unrecognized classification for mTOR inhibitors as direct protectors of genomic integrity.
- Extrapolation to Pathologies of Genomic Instability: Genoprotective mTOR inhibition presents therapeutic potential for mitigating tissue destruction in clinical radiation oncology, cosmic radiation exposure during spaceflight, and orphan progeroid syndromes like Werner syndrome.
4 Likes