"That’s very low saturation, and based on your elevated other iron markers, appears you do have iron absorption issues. Do you have iron labs before Rapamycin? Have you checked for any wonky iron genes? Family history?
I am going to surmise it’s not do to Rapamycin, given discordance in markers."
I’m repeating my iron numbers below:
“My recent labs were all pretty good in terms of CBC, CMP, Lipids, Insulin. However, my ferritin was low (24 with range of 30 to 400); my TIBC was high (499 with range of 250-400); my UIBC was high (437 with range of 111-343); and my Iron Sat was low (12 with range of 15-55).” I did not give you my IRON reading. It was 62 in a range of 38-169.
Question. These numbers suggest to you I have iron storage I need to get rid of? If so, explain. Also, which of these numbers in the iron panel do you consider the most important to suggest one has enough iron but not too much?
To answer your question above, years ago, I did a battery of tests with a hematologist (given my Dad had a number of blood clotting disorders) and all were negative.
Taking a closer look, considering your very low TS and high TIBC, blood donations, and vegan like diet, appears you are iron deficient (look iron at definitions above)
Suggest you stop donating for now, take Vitamin C, consider iron supplement, rebuild your iron stores.
Review all this with your healthcare professional. I am not qualified to offer medical advice.
MAC. This is quite helpful. I know you are not a medical doctor so no worries there. Your reply helps me better understand the situation and thus better able to discuss with my PCP.
Thanks
I really like this article because it explains things that a layman can understand.
So, the main thought is iron is one of the primary causes of aging?
“It can be seen from all of the above that iron is a common theme in many if not most life-extension interventions.”
Yes, I have come to believe iron is implicated in many aging pathways. Beyond the physiological minimum (just above anemia), the excess is just harmful. And now we see the benefits of say phlebotomy and rejuvenating the proteome.
Iron has underlying support in other lifespan extending interventions. CR and low protein (say low animal protein) is essentially low heme iron. Eating less red meat is eating less heme iron. Vegan/vegetarian diet is low heme iron. Women generally liver longer vs men…less iron stores over a lifetime.
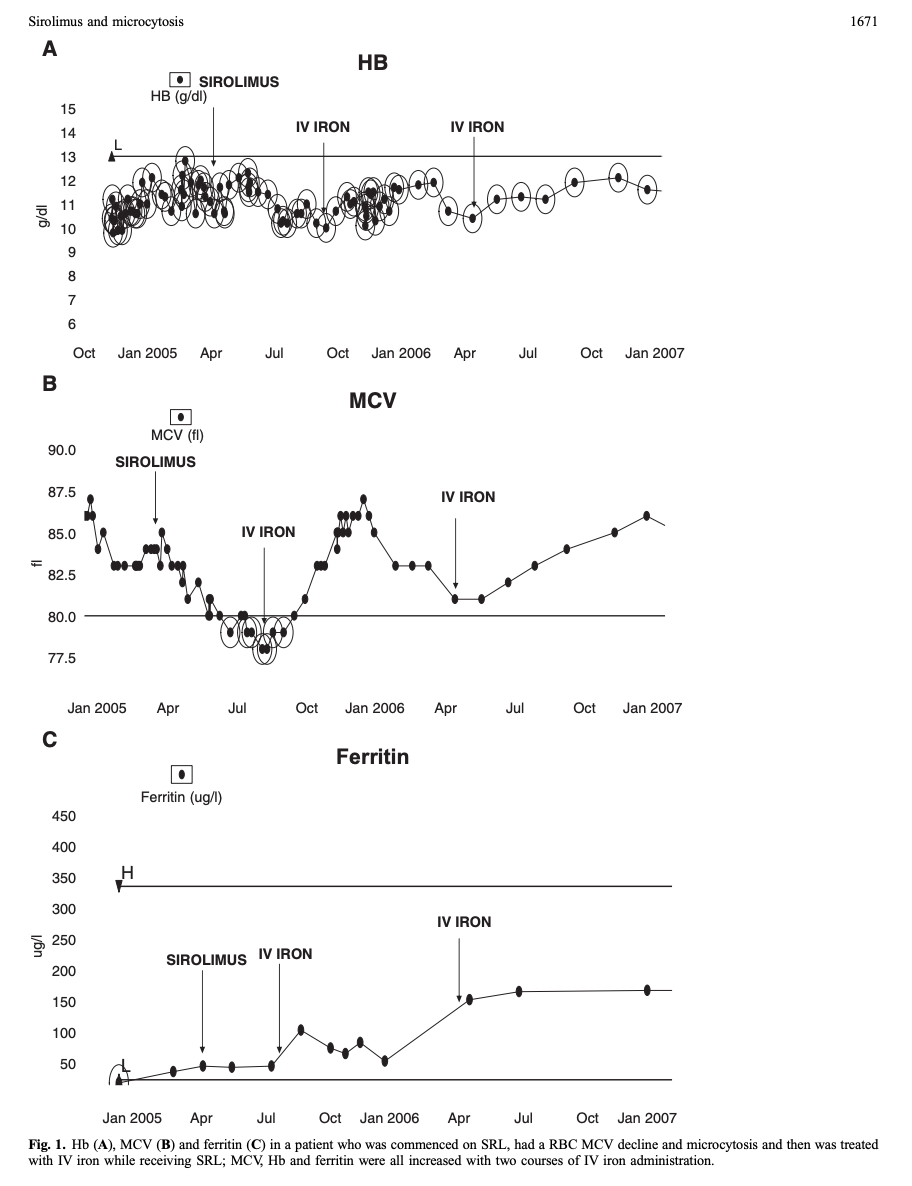
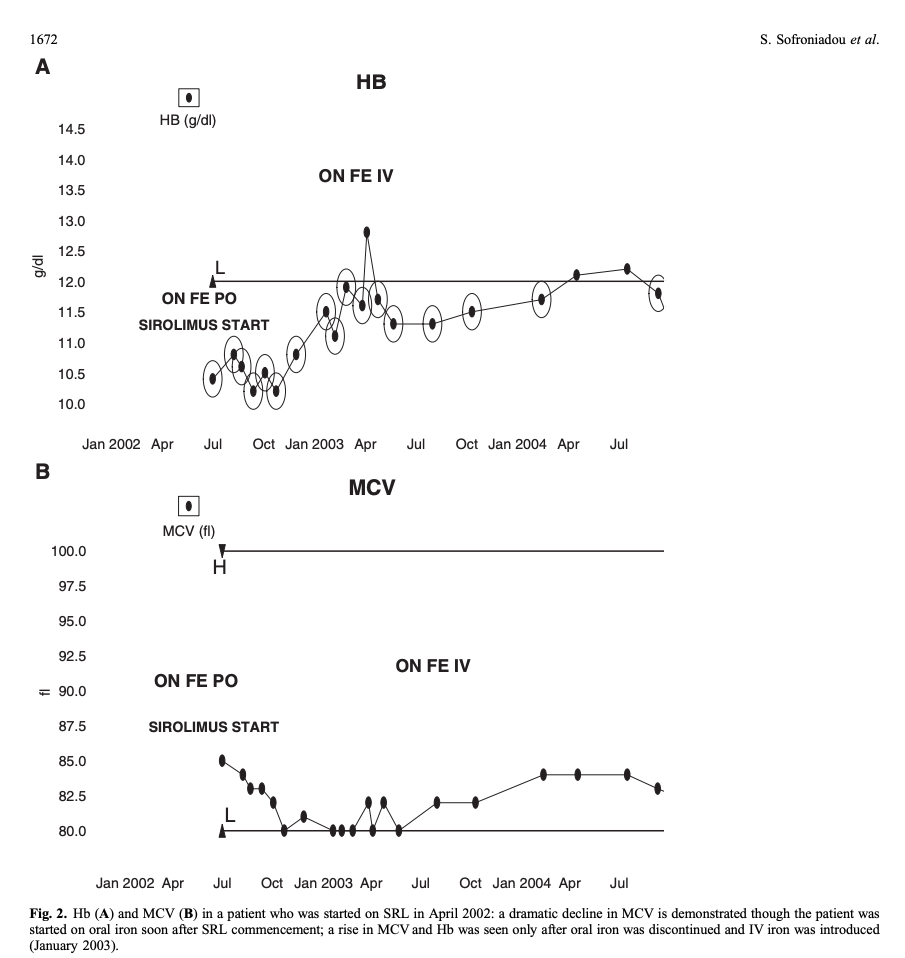
Here’s a little gem paper on Rapamycin, RBC MCV, and iron supplementation (2010).
It would appear that for those crossing into significant RBC microcytosis* (in this paper, chronic Rapamycin dosing cancer patients), iron supplementation WILL reverse. But ONLY IV iron, NOT oral, indicative of some form of gastro/liver Fe dysregulation by Rapamycin.
*“The RBC MCV exhibited a significant gradual decline within 1 month after SRL commencement until the end of the observation period (24 months). During this interval, the mean MCV fell from 91.0 fl at time point −1 to 82.0 fl at time point 24”
Where I am at, my lab range for MCV is 80-98 fl.
"In conclusion, our results suggest that SRL-based immunosuppression cause early, profound and sustained RBC microcytosis that is reversed after drug discontinuation. This microcytosis is independent in time and degree from SRL-induced anaemia. The factors that correlate with MCV decline and microcytosis appearance are SRL levels and utilization of IV iron; the former having a negative impact and the latter a positive one. Both of these findings are novel ones. The fact that IV iron utilization was shown to be the only independent predictor of the MCV change despite the effect of SRL levels probably indicates a functional iron-deficient state induced by SRL. We feel that functional iron deficiency is the possible mechanism for SRL-induced microcytosis development probably reflecting the impact of SRL on hepcidin, but further ideally prospective studies are warranted to clarify the underlying pathogenetic pathways. Understanding the impact of mTOR on iron pathways may throw new light on this fascinating class of drugs, while also spare patients from invasive procedures to investigate ‘chronic iron loss states’.
I noted that runners (serious competitive runners) often have low iron and that its thought that they lose much of it through sweat. I spiked in serum iron due to the combo of eating liver, switching to an iron skillet, taking vitamin C, and stopping saunas with my gym closed for C19.
Luckily when i saw my blood panel results it was spring and i could start running again. My gym sauna opened again and I went for 40 minute sessions at 180 F degrees. These two factors combined with giving the skillet away and greatly reducing organ meats brought my iron waaay down.
I also donate blood now and try to keep TS around 20%
I got a hair tissue mineral analysis a couple years ago from evenbetternow.com . It says my copper is nearly in the low and iron is nearly in the high, the ratio they have as dangerous. Never really noticed it before since they were both in the acceptable range. I need to up my copper. Thanks guys.
Great that you found this so you could correct. There’s an independent researcher (not affiliated with any university or research lab) who, out of curiosity, went way down a rabbit hole on iron metabolism. He says he read about 3,000 papers to figure it out. His conclusion was the importance of primarily copper and secondarily retinol to allow for the healthy recycling of iron. Without copper excess iron will get stored in tissues.
To be honest I’m still learning/researching about copper. I may increase dose as my understanding of iron metabolism improves. Like any metabolic system its incredibly complex.
My serum copper is in a good range (by labcorp ranges) but I’m considering taking the “full monty” panel to get the full picture. If you scroll down a bit on this website it describes that panel along with their proposed optimal ranges: "Ideal" Values for Lab Tests - The Root Cause Protocol
I like to understand and therefore research how metabolic systems work in order to form an opinion about which medical advice (or standards) to believe. I believe a lot of standard medical care is wrong or antiquated or profit driven. However, a lot is right. Same is true for functional medicine, or integrative medicine. My goal is to wade through the firehose of information and form an opinion for myself.
Based on this study some would say hair tests are unreliable. I think the study says they are pretty consistent.
I spend thousands of dollars on soil tests for my farms and they tell me something. I once saw a talk from the ISU extension soil scientist who talked all about splitting tests and sending them to the same lab or to different labs and the different results. Also he would sample the soil, then turn around and sample again. Different results. Still, he thinks they tell you something objective about the soil and the results, while not exact and repeatable are somewhere in the ball park. And I think they are better than nothing. Nothing is what you have if you don’t give it a try.
When I got my hair test Uranium was way high and ditto with Zirconium. I puzzled about it and spent time on the internet and found out these results come from having a Radon problem. Bought a test and sure enough levels were pretty high. Raised 5 kids here and lived here 40 years.
My sodium was way high because I like salt, and potassium was pretty low. I got away from chips around then and started using potassium salt on food.
People scoff about the hair test. We have a couple doctors in the family (in laws) and they shake their heads, but I think this is useful stuff for $100.
Also my brother’s doc sent a split sample of his blood (for hba1c) to 2 different labs and got 4.8 at one and 5.5 at the other. My brother was steaming. Lol. I don’t think it means you stop testing, but now I see how Theranos got by with it for so long.