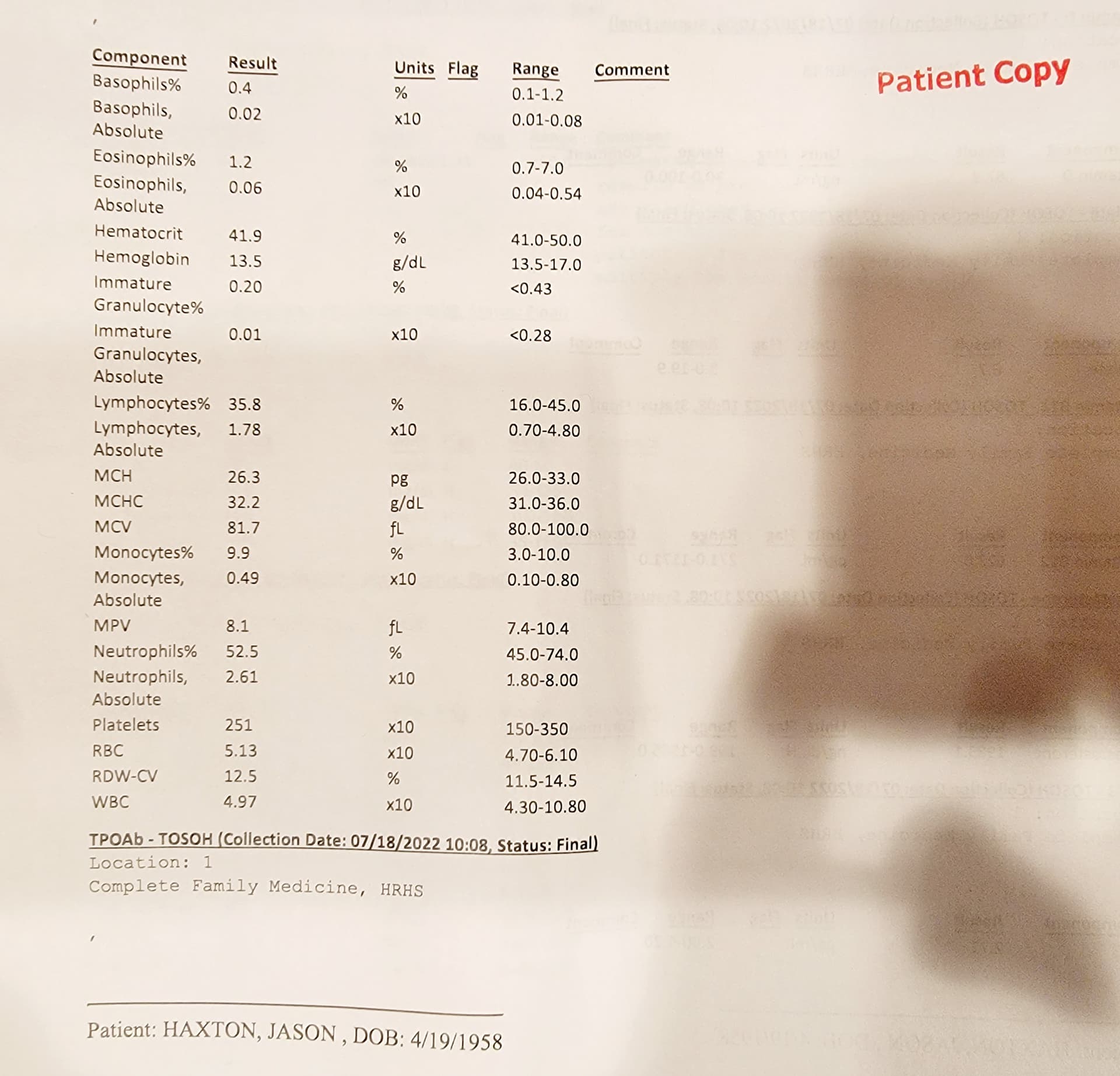
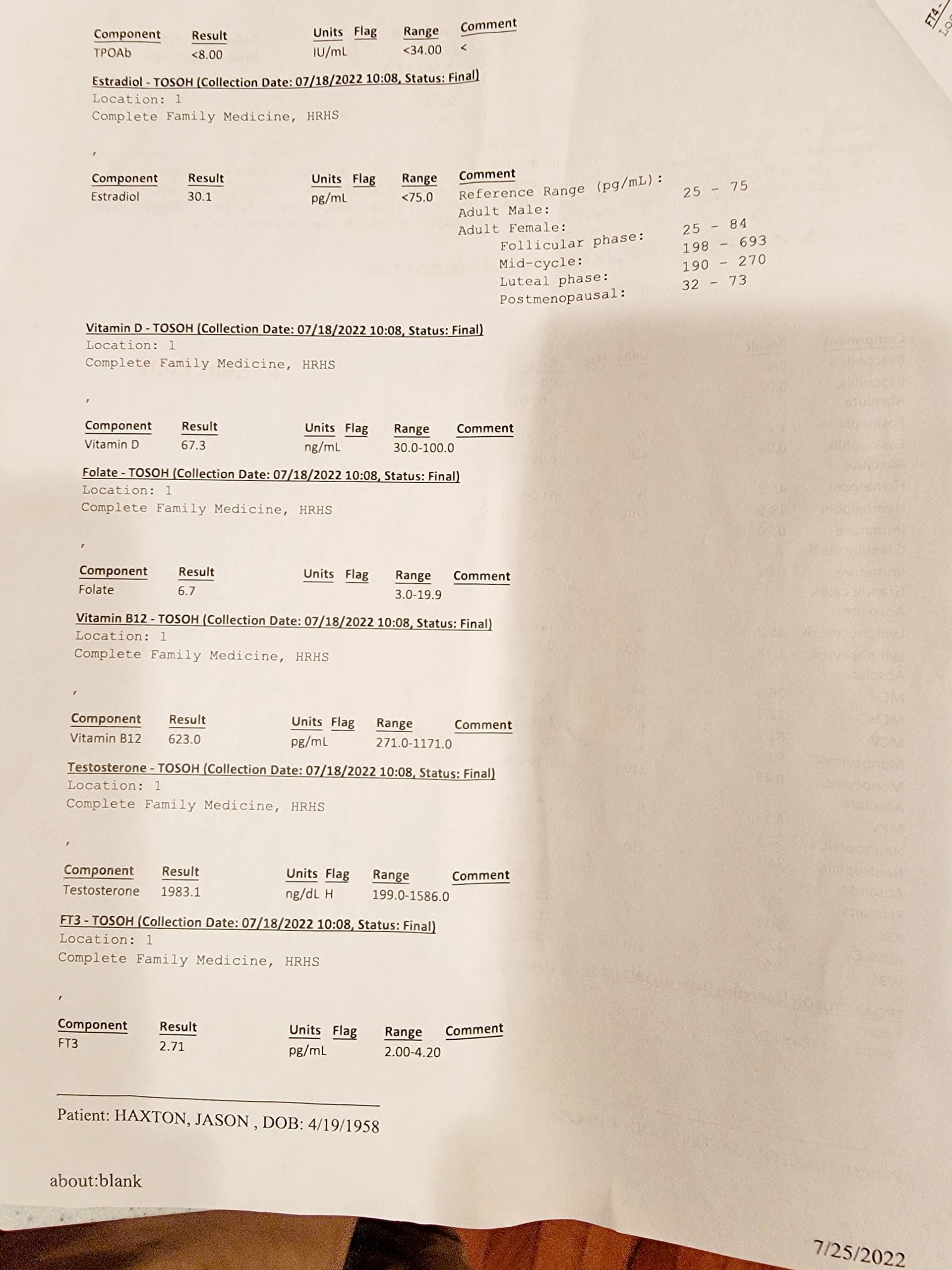
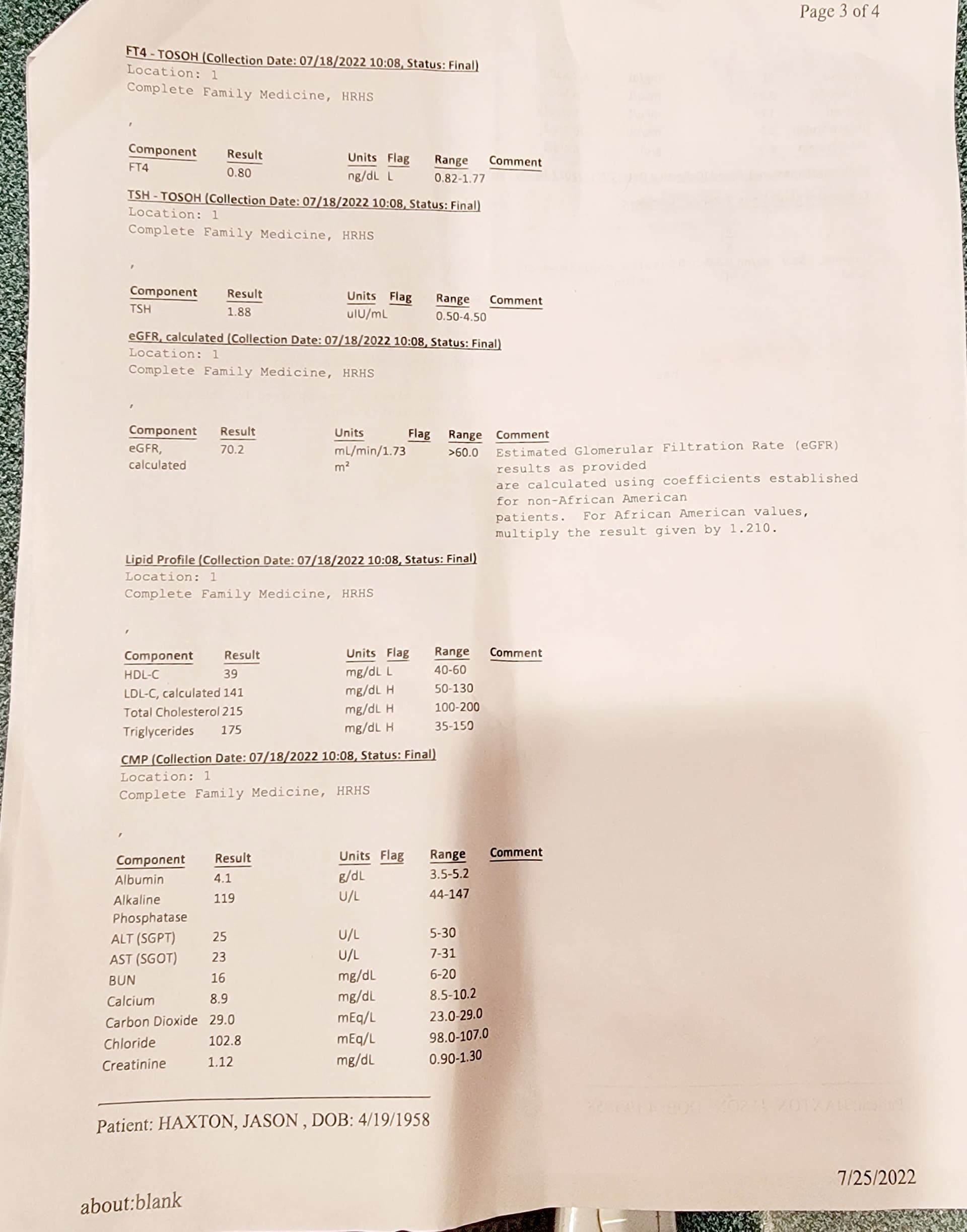
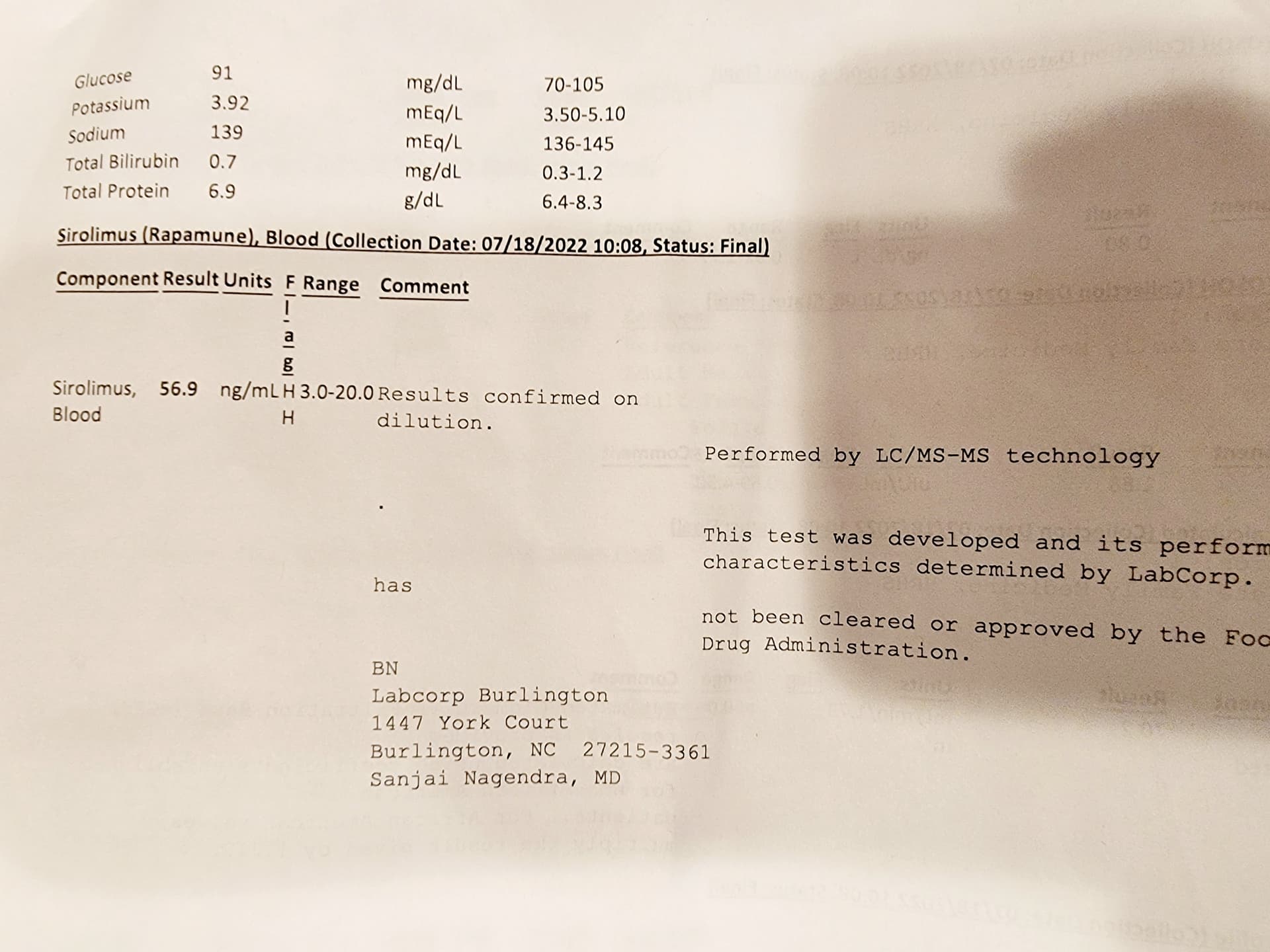
I am waiting for my results from a recent panel. I don’t see that you’ve gone offside in your CBC, especially anemia and WBC, Neutrophils, etc. Your fasting glucose looks fine, I don’t see hbA1c. People in clinical trials taking daily rapamycin doses (far higher than yours, trough levels 5ng/L+) will certainly indicate anemic and low WBC markers, but you’re not even close yet. Even your TG of 175, this is typically far higher. And apparently you feel fine, no real side effects, still exercising. And we have good evidence some of these perturbations will revert lower over time. You are in an incredibly envious position of zero CAC (this could be genetic, a freebie) and excellent health (this is all YOU, kudos!)
But will you live LONGER at this level?
Pushing mTOR2 a bit off it’s setpoint is arguably part of the lifespan extension of rapamycin (but it comes with side effects), this is well theorized in the literature, and definitely a central cancer mitigation axis. Glucose dysregulation is part of the mTOR2 signalling axis, your fasting glucose seems normal.
I’ve been exercising my normal daily routine throughout my current dosing protocol, no impact. I don’t have all my Sirolimus results back (waiting for trough), but my Cmax exploration numbers were VERY high with definite lipid/glucose/anemic dysregulation. No significant side effects, but need a longer duration to fully flush out.
Muscle protein synthesis has mTOR and rapamycin mTOR INDEPENDENT pathways…just keep doing your strength training, and use it as just another biomarker. It’s far too complex to think simply that rapamycin = growth arrest = muscle growth blunting. Per MB, “rapamycin potentiates strength training”! They never gave mice barbells and a resistance training routine. Don’t worry, you can always reduce rapamycin dose, and everything will revert back, this is well established after 20+ yrs of rapamycin studies.
You will have to make your own decision about increasing dose…do you subscribe to MB’s mantra of taking dose as high as you can tolerate? And do you want to explore translating the mice studies showing higher dose = higher lifespan extension? We are all here because of the mice, so are we going all-in with the literature, or holding back? The mice only died of cancer, so do we tinker with mTOR1 AND mTOR2, or just pop a few mg/week and live in wishful bliss? Is hormesis part of the lifespan effects of rapamycin? If you’re not dysregulated in some of the key indicative markers, you’re not moving the needle.