got it !
…
got it !
…
Thanks, for the info. None of the other “flozins” have done anything. I seem to be stuck at ~100. Maybe it’s just age and/or rapamycin. I am going to try dapagliflozin and hope for similar results.
Hey… yeah, just trial and error. Did 6mg rapamycin for 1.5 years. Then, tried 8mg -12mg for a few months… and 36 mg for 7 months. High dose was bad on my biological markers
Dropped back to 6 mg last December 2022. Biological markers improved greatly.
So thinking alternating 6mg… 12 mg…every other dose.
Will have new biological marker tests on the new dosage soon. Will share.
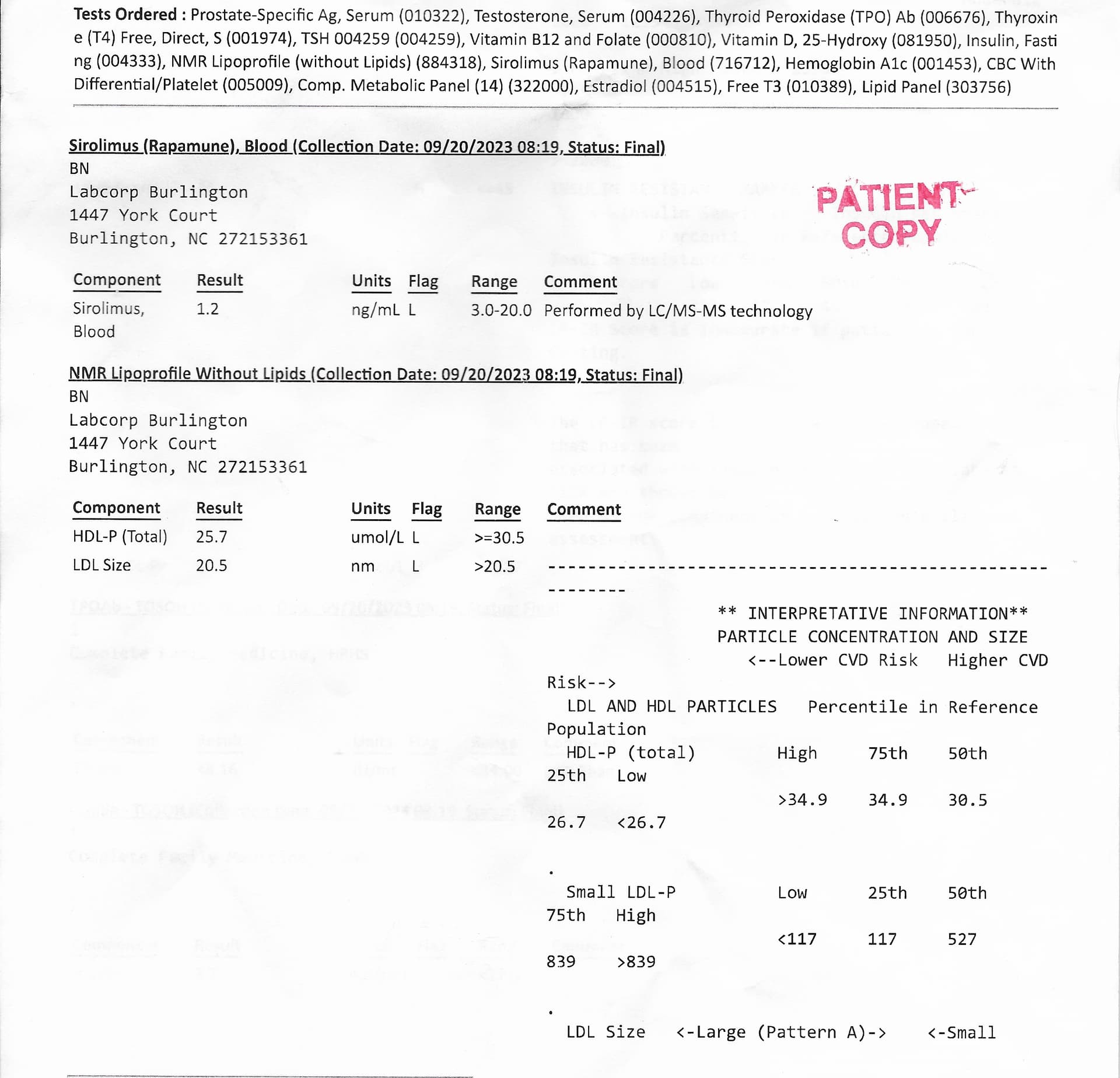
As promised here are my Labcorp results on sirolimus/rapamune - I take rapamune.
Blood was drawn on Sept. 20, 2023 at 8:19 am my rapamune trough was 1.2 ng/mL considered low.
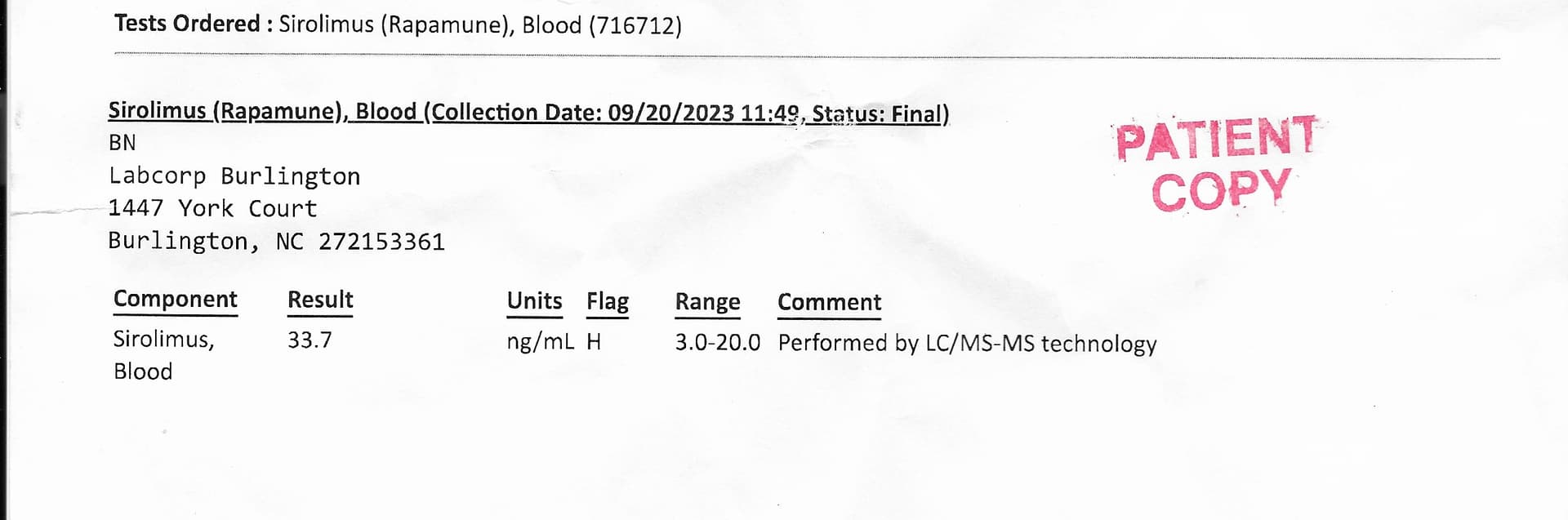
Blood drawn 11:49 am – 2 1/2 hours after a dose of 6 mg and juice with pulp of 1 Red Grapefruit about 5 fl. ounces. C-max 33.7 ng/mL much higher than I like.
I am consistently getting a 6x’s increase in my dose of 6mg and GFJ.
Definitely going back down to just 2mg and GFJ to get approx. 12 ng/mL I think this is my dose sweet spot.
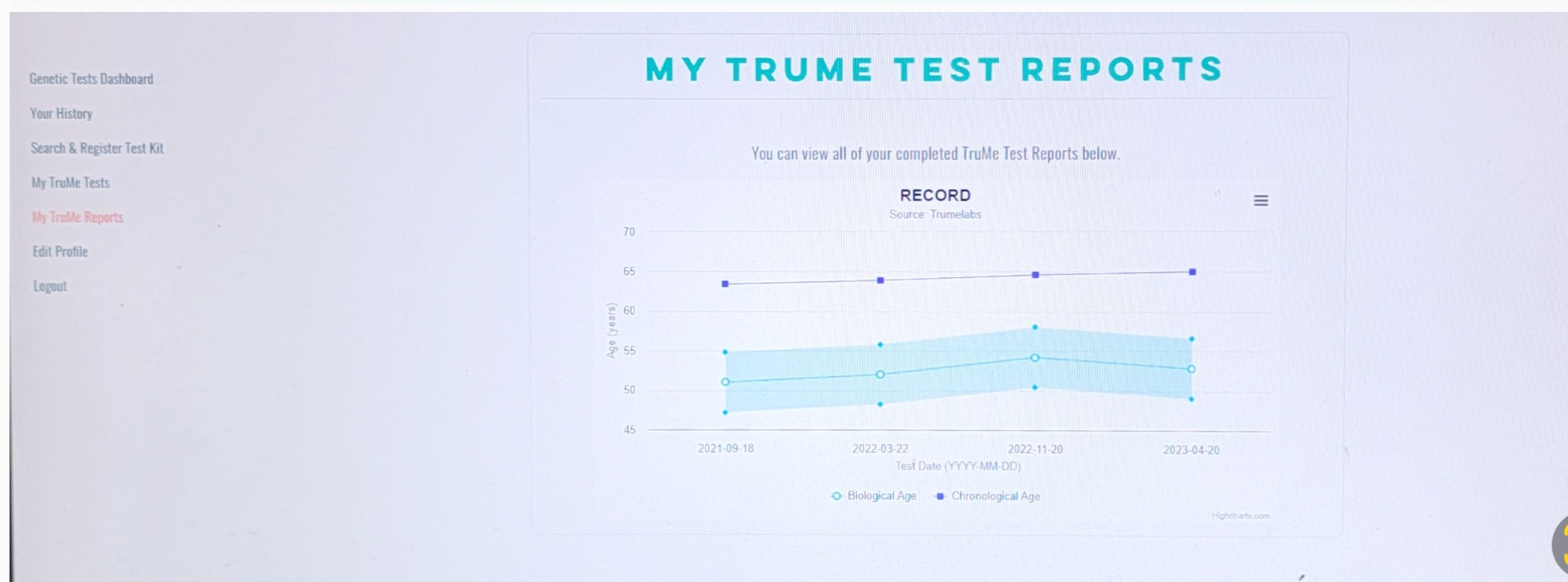
I am a firm believer that the higher dose of rapamune 30+ ng/mL actually blunts my biological benefits, as shown on my previous GlycanAge and TruMe tests.
Will have my latest GlycanAge and TruMe tests back in 3-4 weeks. Will post my 2 and a half years graphs of both.
Thanks for that detailed information. That’s Impressive. Two questions:
How are you calculating that you are getting a 6 x increase from your grapefruit juice? What is the standard you use?
How do you explain the 6x results? Is there something unusual you are doing in preparing the grapefruit? For example, do you eat the sections? Juice it? or peel and vitamix the pulp as I’ve been doing, (which adds a bit of the rind). How long do you wait after the gfj before taking the rapamycin
I can share my results with pfizer rapamune taken with water, 6 mg, tested some two hours later and my result was 14 ng/ml. I know that we absorb and metabolize rapamycin quite individually, but per this result @Agetron is probably getting the estimated around three fold absorption. When I got the test I wasn’t really planning on doing it, but I was at the clinic getting some other tests my doctor ordered and I jokingly asked if they do sirolimus test and they said yes and took another vial of my blood for that. I will do another more comprehensive test in few weeks, am planning to test without and with GFJ and second test with one of the pharmaceutical CYP3A inhibitors (itraconazole or ritonavir) and measure it at 24 and 48 hours to be able to better estimate half life and AUC per @Olafurpall suggestion in another topic a while ago. Cmax is not that important in my opinion, since higher Cmax might be needed to get to some tissues, but I am more oriented towards testing how long rapamycin is inhibiting mTOR… how long autophagy is stimulated.
Hey Chuck - How I come up with a 6x’s increase is:
My rapamycin trough (low point in my blood) with a blood test was at 1.2 ng/mL typically you want 1 or under before your next rapamycin dose. So basically the rapamycin has worked its way out of my system. Takes a week for low dose (5-6 mg) or maybe 10 days for a higher dose (10-12mg).
Next, I took a fresh Red Grapefruit (bought at Wal-Mart) - cut it into quarters and squeezed the slices into a bowl. Gives you about 5 fluid ounces of juices with some pulp. Used this juice to swallow 6mg rapamune (for me that is 3 pills 2mg each). waited 2 and half hours and retested my blood (a blood draw). That gave me my c-max/t-max top dose in my system. In my case 33 ng/mL… so just under 6’xs. Make sense?
It requires doing two blood tests the same day – first a trough. Then, take your rapamune dose and retest 2.5 hours later.
Agree, but if after a week of 6mg or 10 days at 12mg you are at a trough of 1 or less you can be fairly confident that your MTOR inhibition is declining normally from your dose. So for me - that trough is an indication of clearing. I want my max numbers and bottom/trough to be in sync.
I still must be missing something. Sorry to be dense.
Are we saying that 6mg of rapamycin would ordinarily be expected to give you 6ng/ml in blood at Cmax?
So just so I’m clear in order to see if my rap dosing is optimal----on how to do this. I should get sirolimus labs two hours before my weekly rap dose, then two hours afterwards? Thanks for the clarification.
Yes— you can do your 1st blood draw anytime one week after your last dose.
Take your dose with Grapefruit Juice or not and retest blood I think between 2 or 2.5 hours after your dose is best.
My physician is very easy about setting up my blood draws. I might even do one more set of tests when I see him this week. The sirolimus blood test is taken in a lavender topped blood vial. Make sure they put it in the correct color or it will not get tested.
Are we saying that 6mg of rapamycin would ordinarily be expected to give you 6ng/ml in blood at Cmax?
That is would I would suppose.
Thanks. That clarifies the calculation.
But I dont know if that assumption is correct. If there is data somewhere to show the relationship between normal absorption of a given dose of rapamycin with the concentration in plasma at Cmax, that would certainly be something we need to know.
It is rather tricky - no straight answer on the internet - here is one from Mount Sinai that includes sirolimus - and seems to say 4-20 ng/mL is from a 4-22 dose. Almost one to one - if I am reading this right. 4ng/mL comes from 4mg dose.
Link:https://www.mountsinai.org/health-library/tests/therapeutic-drug-levels
With most medicines, you need a certain level of the drug in your blood to get the proper effect. Some medicines are harmful if the level rises too high and do not work if the levels are too low.
Monitoring the amount of the drug found in your blood allows your provider to make sure the drug levels are in the proper range.
Drug level testing is important in people taking drugs such as:
Testing may also be done to determine how well your body breaks down the drug or how it interacts with other drugs you need.
Following are some of the drugs that are commonly checked and the normal target levels:
Yes it is tricky. In the particular article you cited I read it is a target level expressed as either 4 to 20 ng/mL or as 4 to 22 nmol/L rather than results related to a particular dose.
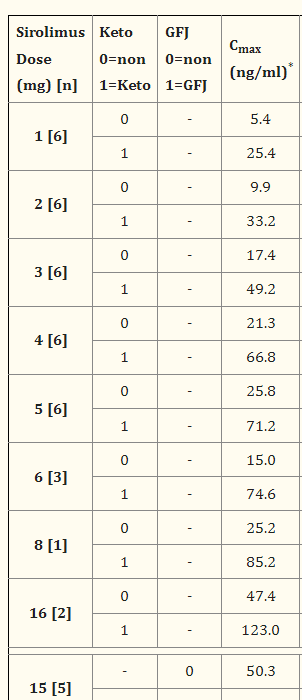
I might have found something here: Phase 1 Studies of Sirolimus Alone or in Combination with Pharmacokinetic Modulators in Advanced Cancer Patients - PMC
In one of their charts they show Cmax of 15 ng/ml for 6mg dose with no inhibitor.
So if I’m reading it correctly you are getting about 2x with simultaneous ingestion of 6mg rapa with 5 oz of gfj.
Hmmmm… how to read this?
The way I read it is:
At a dose of 6mg, with a sample size (n) of 3 patients, given neither ketoconazole nor GFJ, the Cmax was 15ng/ml. With keto, however, the Cmax was 74.6. That sounds reasonable since there is an expected 5 fold increase in absorption when given with keto.
This is admittedly a pretty small sample and with so much individual variability, I dont know how much credence you can give it.
Thanks for clarification… still don’t get how to get a handle on dosing with GFJ.
I do know that at 36 ng/mL amounts for 7 months… my biological age took a hit on glycans and Methylation. Lol
Look at that aging bump for 7 months at 36 ng/mL 6mg rapamycin and GFJ… reduced back to 6 mg … no GFJ… and 4 months later better biological age with two different tests.
Hi. I was just reading you have occasional problems with insomnia. High histamine foods can cause this in some people. Grapefruit is very high in histamine. Might be worth checking if you feel uncomfortable when trying to sleep after eating foods that are known to cause problems with histamine. An unknown histamine intolerance could also cause problems with stress and anxiety along with a load of other symptoms. Worth thinking about.
Very puzzling indeed!!