desert shores, test a “CAC (coronary calcium”?
I think this is also called a Fast CAT.
Several year ago my other half, they wanted to do an angiogram on her. She was in her mid 60’s. I was totally against it, I wanted a Fast CAT before. The physician would not recommend, Make a long story short I went shopping for the Cost without insurance pricing was anywhere from $150.00{yes $150.00, this was in Florida at a private owned radialogy center if I recall] to over $6,000.00 at at a local hospital.
Located a local (NY area)private radiology group , who would do the scan for $500.00 no insurances. Then found a physician to prescribe. Scan showed less than 9% CA. When this was brought back to the original physician who insisted on the angiogram, he was furious beyond furious, no angiogram was ever performed. Never to this day has she had an angiogram.
If this is the test you are wanting go shopping{cost, paying cash] for the test and then a physician to write the prescription.
Thanks for the info. I have had several cardiologists over the years because my primary physicians note my slightly abnormal EKGs that are due to the fact that I had rheumatic fever as a child. I have never met a cardiologist yet who didn’t want to do an angiogram and put in a stent in the process.
Thanks, Peter Attia is an excellent source of longevity info as is Dr. Brad Stanfield and Michael Lustgarten, Ph.D. (Michael is planning on living forever) If you haven’t already watched his Youtube videos he is an excellent source of probability factors and all-cause mortality risks as measured by epigenetic markers.
I have high Lp(a) and strong family history of heart disease, so I take a PCSK9 inhibitor and ezetimibe, also amla extract and citrus bergamot. I was on various statins for years but they aggravated musculoskeletal aches/pains. IMO the single most important, verifiable thing one can do medicinally to reduce future risk is to keep LDL particle number as low as possible. BTW crestor/rosuvastatin is the most potent statin and also isn’t metabolized by CYP 3A4, so it has no interaction with grapefruit or 3A4-metabolized drugs. Also, PCSK9 inhibitors can be a bit challenging to get covered by insurance. You’ll typically have to try/fail one or more statins, ezetimibe, etc first since they are generic and cheap.
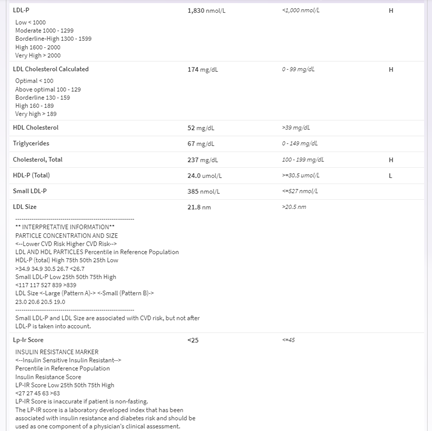
No, he just did the NMR lipoprofile. I think he wanted to make sure I dont have any risk factors and we can get a more in depth look at what is going on
Thanks, I will update when I get results back from my NMR, Lp(a). I do not have a family history of any heart disease so I am interested to see what is going on.
Any other things I should consider looking into?
So my CRP was 0.5, so that was good. But I just got my Lp(a) back and it was 169nmol/L, still waiting on NMR results. Any thoughts on how I should try to lower this? I know that Statins effect more LDL and ApoB but do not have any effects on Lp(a).
So my Lp(a) was 169 nmol/L in comparison to standard value of >75nmol/L, how high was yours? And do you have any advice on how I should try to lower it? My Crp was low (0.5) and still waiting on NMR lipoprofile results.
Wow yeah, that’s high Lp(a) for sure. I’m surprised you don’t have a family history with that level. PCSK9 inhibitors put a nice dent in it (maybe 30%), but it’s tricky to get them covered by insurance since they are only indicated for LDL not Lp(a). Review of literature I did a while back showed one study with plant based diet lowered it slightly, also a small review showing CoQ10 lowered it slightly, and one or two studies showing amla extract lowers it substantially. Unfortunately amla extracts available OTC are all over the place with what compounds are standardized, and it’s unknown which compounds in amla actually lower Lp(a), and of course quality concerns being unregulated. Pharmacological doses of niacin lowers Lp(a) but paradoxically does not reduce cardiovascular events (possibly via increasing insulin resistance), so I don’t touch it in that kind of dose. I take amla extract called TruCapros (and also PCSK9 inhibitor called Praluent, CoQ10 as ubiquinol and mainly plant-based diet) and most recent Lp(a) was 84 nmol/L, still high but down substantially. The real hope for Lp(a) lies with upcoming anti sense oligonucleotide drug currently in stage 2 clinical trials, lowers Lp(a) by 90%, can’t wait!
Yeah I read about the Anti Sense oligonucleotide and was excited about that as well. I have high LDL too so maybe they can give me the CSK9 inhibitor for the combo? From what I have read and understood apparently there is not much that can be done about this since its genetic which is weird because I do not have family history of cardiovascular problems( or any disease for the matter). I really am just concerned since I am young(24) and have a relatively healthy lifestyle, that I am not sure what else to really do at this point other than keep my other risk factors low and hopefully get on something to lower my LDL
You’d almost certainly have to try a statin first before they’ll consider allowing you on a PCSK9 inhibitor, since statins are cheap. My insurance required that my fasting LDL be over 100 despite use of maximal tolerated dose of statin+ezetimibe. Lp(a) is irrelevant in their calculations.
And yes, in the absence of specific Lp(a) inhibitor, the experts I’ve listened to recommend keeping LDL (preferably particle number as measure via NMR or indirectly via apoB) as low as possible via diet, supplements and pharmacotherapy as needed.
My Lp(a) has been up over 200 in the past, so clearly what I’ve been doing has been helping.
I’m getting lost in the units here. In metric, I believe Lp(a) is measured in mg/L, and many of the studies I’ve read are also in mg/L. I know conversion should be a quick google search, but this one is oddly impregnable. I’m at 113 mg/L, which seems to be ok.
Do you have a quick conversion guide for mg/L to nmol/L when it comes to Lp(a)?
“A Lp(a) plasma level of higher than about 300 mg/L seems to be a threshold for occurring of cardiovascular events. The combination of raised Lp(a) with arterial hypertension was found to be the most important cardiovascular risk factor. Lp(a) levels under 232 mg/L appeared to be a marker for good prognosis.”