I can’t find any website or indepth information on Torcept Therapeutics. Did you? It seems they purchased the IP of Mt. Tam Biotech (a spinout of the Buck Inst. I think, that failed). They don’t seem to be active as a business.
Later this month I will interview Brian Kennedy and I’m going through lots of information currently. In this interview (timestamp). He talks about Mount Tam Biotech and Torcept but it was 3 years ago. Maybe the company does not exists anymore.
Andrea Maier announced last year that they (including Brian Kennedy) will start a rapamycin trial this year. They have talked about if it will be a rapalog or rapamycin. I hope it will be rapamycin or both. I will dig little bit more to this topic in the interview. If you find anything please let me know.
Yes - I talked with Andrea and her team on a zoom call a number of months ago when they were still designing the protocol for their clinical trial. I think they may have started it by now. It was for rapamycin (no rapalogs I don’t think). I wanted to make sure they spoke with Anar and the team at Ageless RX so that they could learn from the PEARL experiences. We all need to learn from each other on this stuff.
Looking at the stock price graph, it started high and then went down a lot. Which means the market is pricing in something.
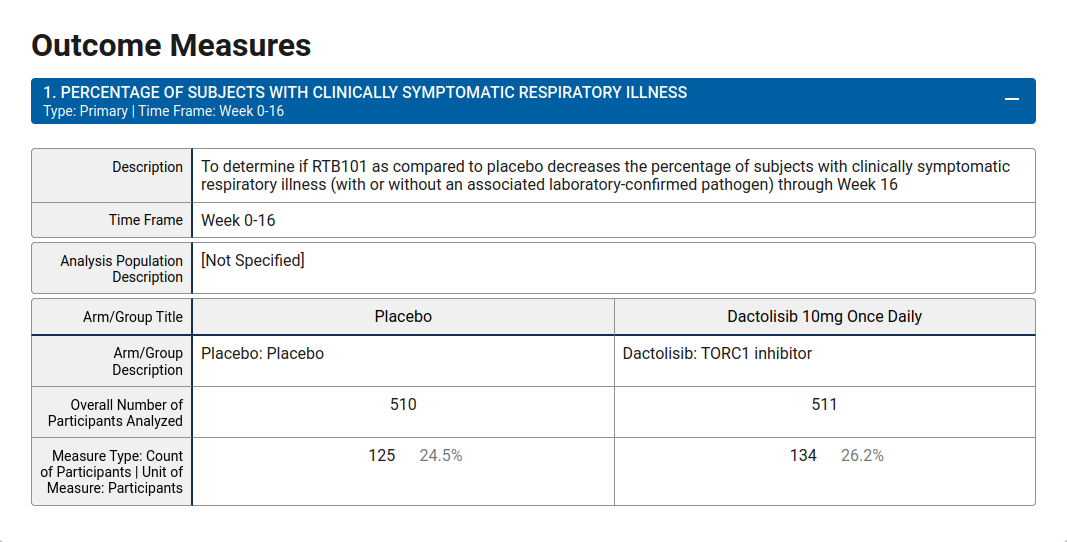
In 2019 the stock fell over 83% in one day, because RTB101 a TOR1c inhibitor didn’t decrease chance for infection.
This article is quite bearish on mTOR inhibitors, which I don’t agree with, but interesting for perspective.
Today’s news is just the latest reminder that biology is incredibly complex. The idea that taking a single drug and targeting a single protein in the human body can activate molecular pathways that protect humans against aging and age-related diseases is wishful thinking at best.
resTORbio has gone all-in on the mTOR hypothesis. The mTOR protein plays a role in telling the body to build new cells (when energy is abundant, such as after eating) or break down old cells and recycle their parts (when energy is low, such as during periods of fasting). There’s solid evidence suggesting that fasting and calorie restriction, which also happen to reduce the expression of mTOR, are two of the absolute best ways to reduce disease risk and prolong healthy lifespan. From the hara hachi bu practice in Japanese culture to a well-controlled study, spanning more than 30 year, of calorie restriction in rhesus monkeys, the results appear to hold up.
So inhibiting mTOR with a drug makes sense, right? Not necessarily.
The problem is that mTOR, as with many proteins, has multiple roles in the human body, and the observed effects from fasting or calorie restriction rely on a biochemical cascade far more complex than can be explained by mTOR alone. This is the classic “Can a biologist fix a radio?” thought experiment in action.
Now what
Investors are right to walk away from resTORbio. The company’s lead drug candidate, RTB101, is a TORC1 inhibitor. The idea of the failed phase 3 trial was to give it to adults over the age of 65 during flu season to see if they had a significantly reduced risk of developing respiratory illness. They didn’t. More importantly, there’s no reason to believe individuals given a TORC1 or TORC2 inhibitor alone, late in life and for a limited time, will lead to any meaningful clinical outcomes in other diseases being studied across the company’s pipeline.
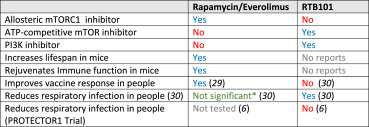
In the table below shows differences between the drugs.
In the context of translational geroscience, it is important to explicitly note that the PROTECTOR1 trial was not a test of the geroscience hypothesis. Unlike rapamycin, there is no data indicating that RTB101 increases lifespan or delays aging in pre-clinical animal models and, as mentioned above, RTB101 is not a specific mTORC1 inhibitor (Table 1). In contrast, the positive results from the resTORbio phase 2 trials with everolimus [29,30] are more directly translatable from preclinical data. While those results are consistent with the geroscience hypothesis, they are not definitive at this point. It seems likely that rapamycin or everolimus can improve immune function in the elderly, but it is uncertain whether efficacy will ever be sufficiently evaluated for FDA approval, due to the prohibitive cost of bringing an off-patent drug (or soon to be in the case of everolimus) through the regulatory process.
AT-20494 is a member of a novel class of rapamycin analogs (often called rapalogs) discovered by Navitor scientists, and it will be the first fully-selective inhibitor of mTORC1 to be studied in humans. Preclinical studies of AT-20494 have shown that it reduces the burden of cysts and kidney volume in mice carrying mutations in the PKD1 gene, and also reduces signatures of fibrosis and inflammation upon chronic administration.
Tom Hughes, president and chief executive officer of Navitor Pharmaceuticals LLC commented: “We are thrilled that the potential value and substantially differentiated profile of Anakuria’s mTORC1 inhibitor program can be explored with Janssen. With decades of experience in developing, manufacturing and commercializing innovative therapies for patients suffering from a broad range of diseases and conditions, Janssen is ideally positioned to rapidly advance our program in the clinic.
There are hundreds of different rapalogs out there so these new rapalogs are most likely nothing to start self-experimenting with. Cost will be high in the beginning but after the the patent is not valid anymore the cost will go down.
Yes, it’s because of the patent. Otherwise the pharma companies would not have an interest in investing huge amount of money to get them approved. So they need return on investment. If the investors don’t get return on investment they will invest money in other areas instead. That is how the system works.
One the thing we could do as a community is to develop our own rapalog and put in our money in this project but my feeling is that the interest in doing so seems quite low. What are other ways to solve this development of a longevity faster and keep the price at similar levels as Rapamycin today? Any thoughts? If we look at the development of Rapamycin it goes very slow forward. We have not got one single clinical study human study published yet. The good thing is that things have started to move forward but the studies are quite small. Even the PEARL trial is not so big but it’s better than nothing.
This issue isn’t the “development of our own rapalog” - the issue is the $40 Million+ needed for the large human clinical trial. We don’t even need to develop a new rapalog, we have rapamycin already with great preliminary small mammal data, but nobody is interested (so far) in funding the clinical trial…
At some point I would hope that perhaps a government that has a national healthcare system would be motivated to roll the dice for the small investment in a good rapamycin clinical trial, as such a country (e.g. Canada, UK, Japan, etc.) would save $10s of Billions in healthcare costs over the next decade…
To develop a new rapalog can be interesting if we could increase efficiency and lower potential side effects but I agree that there are other things to invest in the Rapamycin research field currently that could be interesting in the moment. But I have a feeling there is not a big interest to do it. I don’t know if it’s because there is no interesting trial to study on. We have for example Brad Stanfields trial which is currently in the funding phase. It’s not that much money which needs to be collected.
The PEARL trial was a great success which was crowdfunded with over 200%. I wonder if we as a community could set up an interesting clinical trial which searches for an answer in an area of big interest. This is to take control a little bit around our destiny instead of just waiting for other people to roll the snowball. What do you guys think about that? Maybe that could increase the interest in funding a rapamycin trial?
Funding for aging will not occur from US Government until/unless “aging” is classified as a disease that is treatable.
If you have not already reviewed, review in detail the older interview Attis with Nir Barzilai , I think it is the one from January 7, 2019
#35 – Nir Barzilai, M.D.: How to tame aging
Barzilai explained in details what he is trying to do is NIA to classify “aging” as a disease that is treatable to open federal research money.
And Barzilai should know he has the experience in drug development and approves .
And you will not going to like this part of what I post.
If you think that Stanfields “trial” is going to produce anything for moving forward, it will produce bupkis, the only thing it will produce is some money for the people performing the “trial”.
As I have stated/posted before in my view Stanfields is a grifter/schnorrer.
But the thing I mean is that we all in the longevity community have money. We should not wait and rely on the NIA to fund trials and we should not wait for researchers/physicians to create trials. We should start acting in the community and move things forward. You say that Stanfields trial is not good. Let’s put up a trial which we believe is a great one and fund it with our own money. I don’t understand what we are waiting for? Let’s create our destiny and start rolling this snowball forward.
Some here have messed with brushing their teeth with rapapaste. Though maybe it’s expected to act through the gums, idk. Is there any trial related to this?
Seems like making rapapaste and placebopaste would be easy and relattively cheap. Enroll a 100 rapa, 100 placebo, maybe 100 doing what they always do.
")