- I’ve done a site wide search and have not been able to find this discussed.
- I was reviewing “Phase 1 Studies of Sirolimus Alone or in Combination with Pharmacokinetic Modulators in Advance Cancer patients”
- https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4410974/pdf/nihms604208.pdf
- On page 14, there a figure that shows a rebound effect with Rapamycin.
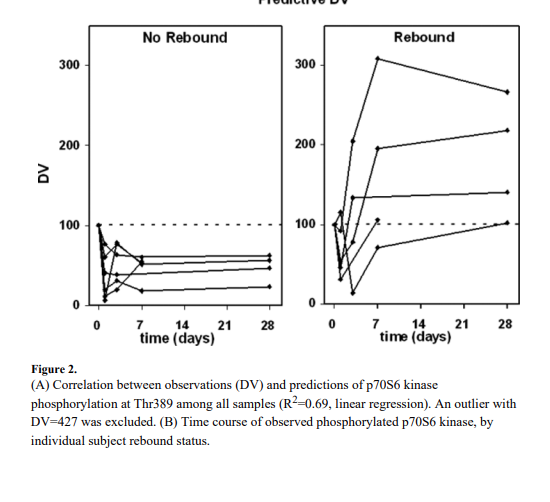
- According to the authors "paradoxically, in 6/12 subjects we observed a rebound effect on phospho-p70s6k where phorsphorylated protein levels exceeded baseline at later time points (including 28 days later)
- Unfortunately, they don’t state explicitly what dose resulted in the rebound, but they do add that “we determined rebound was driven by the concentration of sirolimus”
- What do you all make of this?
- 6/12 with rebound; with 3/12 with levels above baseline at 28 days?
- I realize these are small numbers and it is difficult to draw conclusions.
- As an aside, did anyone notice that Cmax for the GF baseline 15 mg was greater than the Cmax for the GF baseline 20 mg (prior GF intervention); I wonder if this is due to patient variability or small sample size.
3 Likes
This is a recent post by Mikhail Blagosklonny on the topic.
https://twitter.com/Blagosklonny/status/1710639122962956530
Here is my view
https://twitter.com/KristerKauppi/status/1710905055082066170
3 Likes
I understand that you try to view this trough positive optics, but in my view there is a 50% chance rapamycin supresses your mTOR and what is more disturbing that in other 50% it increases mTOR activity at the later point. From the text it is difficult to understand if the rebound was independent of continuing rapamycin therapy or it is observed after you stop rapamycin. But with some the rebound was observed quite soon after first dose.
1 Like
Weekly dosing in Mannick have had benefit on immunosenescence so it might not matter so much. Of course daily dosing was slightly better, and higher dosing was as well. My prior is against daily dosing for people who don’t do it for transplant reasons because almost no one does so.
1 Like
I think it’s important to take the dose in consideration. My guess is that high dose = high rebound effect. Low dose = low rebound effect.
I think this quite well aligned also with how other different biological process work. For example how insulin work. See image below
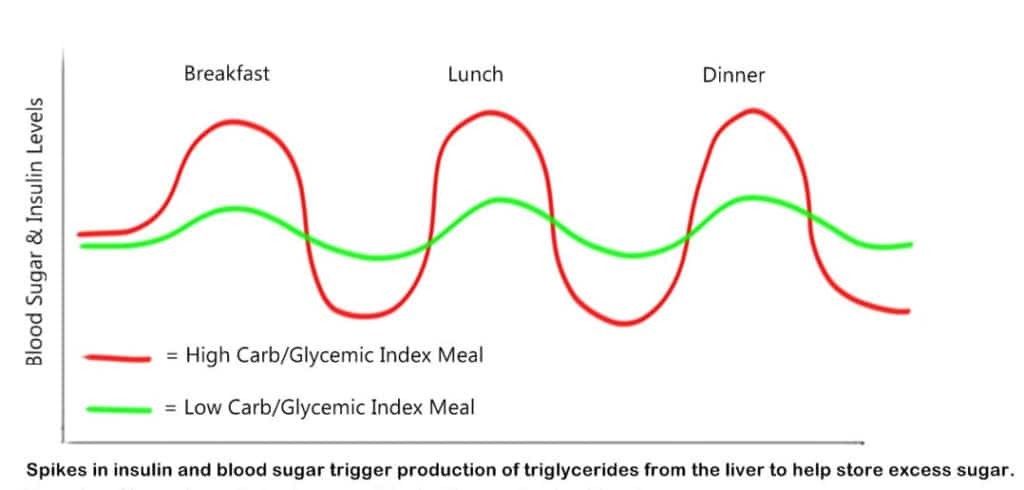
High insulin spikes = High rebound effect. Low insulin spikes = Low rebound effect. The reason why it is like this is probably because the body tries to achieve stability (homeostasis) this way is my guess.
1 Like
High doses had greater benefit in Mannick study on immunosenesence, so it probably doesn’t matter much?
What study was that and what is high dose according to you?
High dose for me is > 12 - 90 mg of Rapamycin but then it also depends on how often it is taken. But even if it is not taken so often I would classify > 20 mg as high. 90mg is very high.
It was the Mannick paper from 2014 with everolimus.
Graph A and B are just depending on how much previous exposure they have had to influenza, meaning B is lower exposure. It looks at response to vaccine (immunosenesence), basically building antibodies in response to it. The vaccine was given after a 2 week break suggesting improvements in immune system.
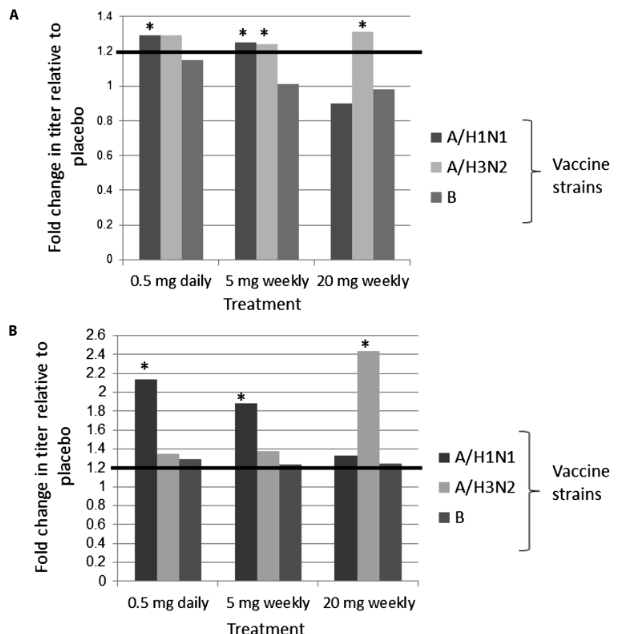
As you can see the higher 20 mg/weekly dose had a larger increase than 5 mg weekly and 0.5 mg daily, but it showed in the study to have more side effects. 0.5 mg daily was slightly better than 5 mg weekly and with a similar side effect profile. It is important to note it is not possible to split rapamune tablets as they have enteric coating, it will ruin the bioavailabilty.
1 Like
Ah, ok the 2014 study I forgot that the 20 mg had a bigger effect. Thanks for the reminder there but as you said it had higher side effects. One other thing here to take inconsideration is that this was on everolimus so 20mg is not the same as 20mg of rapamune. I don’t remember the translation here but probably more around 15mg or something like that. Do someone have a better estimate on the conversion?
Will not 15 mg weekly also have the risk of accumulating the blood levels of rapamycin?
1 Like
I understand your logic, it might be the right approach, but but I would want to be more sure about mTOR follows the same logic.
Cause if the rebound observed in the study was during rapamycin weekly regimen and not after cessation it might not be really good. As you want your mTOR below baseline, don’t you think?
Everolimus is actually more potent, so rapamycin would be dosed slightly higher, according to Mannick herself. But they are pretty equal.
I don’t know about accumulating blood levels, it reaches a limit I’m pretty much sure. But yes it would probably be high. I don’t advocate high doses.
@scta123 I fully agree more research is needed but I think it’s important to look at what doses the study use. If I understanded it right the doses that was used was 16 mg, 25 mg and 90 mg. So it is quite high doses if you compare it to what most people in the longevity community take. I take 6mg and if I would go up to 16 mg that would be a quite big jump up in dosing and I guess I would get more side effects from it.
One other thing probably also to have in mind is that the rebound effect can be good or bad depending on context. For a cancer patient its probably bad but for a healhty person who exercises it may be good. But more research is needed as I said.
@AnUser Interesting, I have always thought it was the other way around. If I remember it correctly in the Peter Attia podcast in which he interviewed Lloyd Klickstein they touched on the topic and said that Everolimus is a bit weaker than Rapamycin.
1 Like
In the last podcast where MK, PA and David Sabatini discuss rapalogs they basically say it is the same molecule, no conversion needed. Which would be in line with transition from sirolimus to everolimus in transplant patients which is usually 1:1.
2 Likes
Rapamycin and Everolimus have very different half lives. Rapamycin has a half life of 63 hours while Everolimus has a half life of 28 hours. That’s a pretty big difference.
I read the whole thing. It happened to half of the participants, not to the other half. The doses they were taking were also much larger, around 60mg a week or more if I recall. The only real side effects reported were high triglycerides, high cholesterol, and high glucose. I wish the authors had elucidated whether the incidence of these side effects was associated with long term mtor suppression, mtor rebound, or whether it’s random. Also remember these are people with incurable cancers. Their internal chemistry is far from normal.
12 Likes
Based on previous Blagosklony comments on rebound, I reduced my dosage to 2 mg every 4 days a couple months ago. But after this most recent tweet & article, I’ve decided to stop taking rapa until (if) we get convincing data. I have been taking taurine 3mgs a day for a couple weeks now based on Dr Green & I feel a strong positive effect. Unlike rapa which for me caused a few skin infections + some intestinal issues. I don’t think we know enough at this stage to put all our eggs in the rapa basket. (We probably don’t know enough about taurine either…)
5 Likes
what kind of strong positive effect? do you take 3mg of taurine all together? and at what time? with food? what are your other stacks? On Rapa, I tried 5mg weekly but I feel better on a daily low dose of 5 days a week.
1 Like
1 gram at a time on empty stomach. nothing else except b12 & vit d
1 Like
You are not alone. I too feel much better with 1 mg every other day. Even 3-4 mg a week was a difficult dose for me to tolerate. I suppose every metabolism is different.
3 Likes
I’m assuming you guys are misspeaking. With Taurine, you’re taking Grams not Milligrams.
3 Likes