I think I might be noticing more peach fuzz hairs filling in places where I thought I had bare skin. I recall hearing that some treatments, like topical minoxidil, only work if you still have thin hairs.
I am wondering if anybody else has had real hair loss reversal with rapamycin or if I am imagining it, and what else I could consider adding to my regimen if I want to give in to the temptation and dive deeper into the dark art of hair loss reversal. I am guessing finasteride or topical minoxidil, but I am sure there is deep knowledge in this crowd.
Of course I am also sure @RapAdmin will point me to three topics where this has been covered already.
If you’re truly concerned about your hair, you should go for dutasteride. Additionally, you should take tadalafil to help preserve your nocturnal erections and increase your T/E ratio.
It is believed that a chronic state of corporal oxygen desaturation or hypoxemia secondary to the loss of nocturnal erections is a fundamental pathophysiological cause of erectile dysfunction (ED).
One theory is that progressive erectile dysfunction occurs due to the loss of rapid eye movement (REM) nocturnal penile tumescence (NPT). Whereas men without ED will demonstrate erectile activity for as much as 60% of their sleep time, men with ED have been shown to lose NPT. This loss of NPT occurs with numerous pathologic processes. This is seen with aging and in disease states, such as diabetes, hypogonadism, and radical pelvic surgery (Karacan et al, 1978, 1989). A dramatic loss of NPT is seen after a radical prostatectomy, due to denervation or nerve damage (McCullough, 2001; Padma-Nathan et al, 2004). Penile shrinkage, muscular atrophy, and associated penile tissue apoptosis and fibrosis have been documented in the animal model and in humans after cavernous nerve damage (Klein et al, 1997; Fraiman et al, 1999; User et al, 2003; Schwartz et al, 2004). The chronically flaccid state theoretically results in a chronic state of penile hypoxia.
It has been reported that lack of sexual activity due to erectile dysfunction (ED) may be associated with testosterone (T) decline. To investigate whether the known changes in sex hormones associated with resumption of sexual activity are sustained in the long term. Primary endpoints were variations from baseline of steroid hormones: total T, free T (f T), and estradiol (E). Secondary endpoints were variations of erectile function domain scores at International Index of Erectile Function-5 (IIEF-5). In an open-label fashion, 20 patients (mean age 54.8 +/- 8.4 years) received tadalafil 10-20 mg on demand for 12 months. Exclusion criteria were those reported for phosphodiesterase inhibitors, including hypogonadism and hyperprolactinemia. Tadalafil assumption was safe and well tolerated (overall adverse effects in 15% of patients) and none discontinued medication. A significant decrease in E levels occurred at the end of the study (from 19.9 +/- 9.6 to 16.6 +/- 8.1 ng/dL, P = 0.042 vs. baseline), with parallel increase in the T:E ratio (26.3 +/- 15.3 to 32.6 +/- 17.7, P = 0.05), whereas no changes in T and f T serum levels were observed, respectively (411.4 +/- 131.4 to 434.2 +/- 177.1 ng/dL and 47.7 +/- 15.3 to 49.9 +/- 19.1 pmol/L, not significant). Interestingly, nonparametric subgroup analysis for related samples revealed that E decrease was detectable only in lean (N = 14) but not in obese (N = 6, body mass index > 27.5 kg/m2) subjects (17.8 +/- 10.1 vs. 13.5 +/- 6.8, P < 0.05). A net increase in IIEF-5 scores was observed at the endpoint (13.7 +/- 5.9 vs. 25.7 +/- 2.9, P < 0.0001). Sustained improvement in sexual function after 12 months of tadalafil administration is associated with increased T:E ratio mainly related to reduction of E levels. We hypothesize that androgen-estrogen cross-talk and possible inhibition of aromatase activity during chronic exposure to tadalafil might have a role in the regulation of erectile function.
Have been taking sirolimus 10 mg once weekly and also applying 0.2% cream topically daily for 5 years. That said, I haven’t noticed any new regrowth or change due to it. Besides sirolimus you may try proven medical approaches such as strong dht blocker like dutasteride or finasteride. You can take them orally, topically as a cream and as scalp mesotherapy. You will also need an agent to stimulate growth for which Minoxidil taken orally and topically is proven to be effective. Latanaprost can be combined with minoxidil to increase effectiveness and is a bit more effective on small fuzzy hair. Which brings me to a method to get these small fuzzy hair in the first place, which you can later strengthen with latanoprost and minoxidil and that is microneedling ( fraxel laser may also be worth investigating).Good luck and keep us informed of your progress.
We can’t be sure if dutasteride mesotherapy is effective since it’s based on some dubious Egyptian studies. If you’re planning to use oral minoxidil, you should also consider taking an ARB.
I would avoid oral dutasteride and finasteride due to the risk of post finasteride syndrome. The risk is small, but the condition is serious so IMO these drugs should not be approved for hair loss. Topical RU54881 does the same thing without this risk. It has held my hairline for about six years and is cheap from china. Micro-needling also works.
No, dutasteride doesn’t cross the BBB. You might experience sexual side effects, but taking tadalafil before you go to bed can prevent permanent changes (lack of nocturnal erections can lead to penile hypoxia).
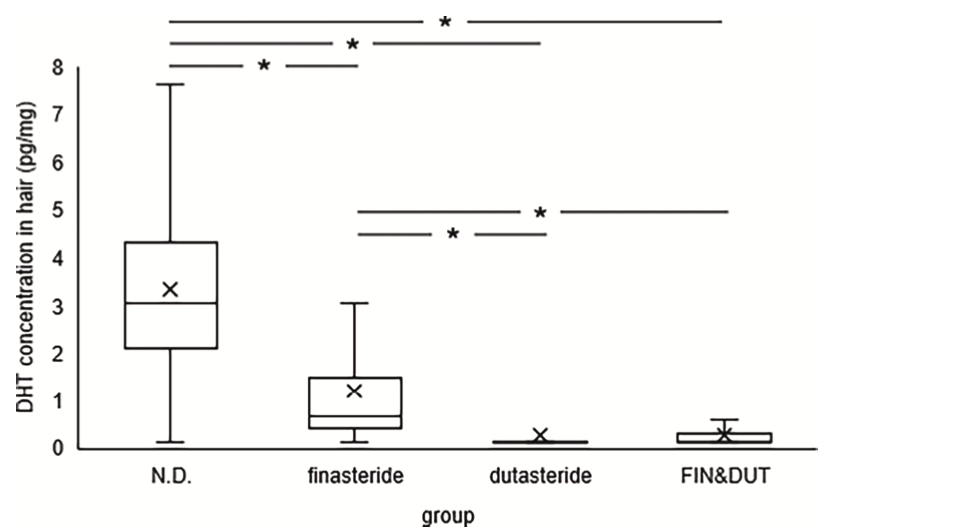
Dutasteride is the gold standard, and it stops hair loss in 98% of patients with AGA. Nothing can be compared to it.
It is unknown whether dutasteride crosses the BBB. And dutasteride can raise estrogen levels which can cause temporary ED in rare cases, but you would quickly detect that and either lower the frequency or quit the drug altogether.
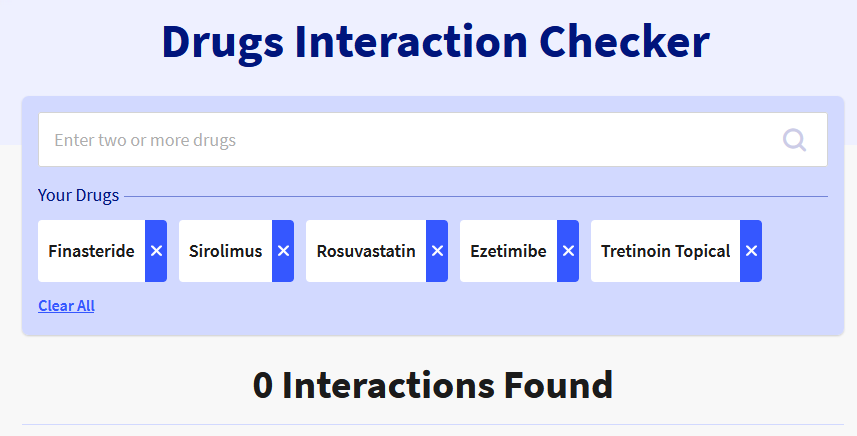
It seems like another complex situation to manage. It’s cool that there are these emerging DTC vertical care providers like Midi Health for menopause and all the different ADHD and men’s health providers. I even got a note about a GI DTC company called Oshi. The problem is that primary care is hopelessly broken in the United States, and none of these DTC companies are any good at coordinating. So you can get a rapamycin script from Ageless or Healthspan, but they aren’t writing scripts for managing your lipids and glucose. Then if you want to treat your hair loss, but you need an aromatase inhibitor and a PDE5i, it’s like – who is going to quarterback all that stuff? There is a ton of great information on this forum, and I’ve learned so much here, but I have some reservations about how far I want to go in managing all these different medicines based on Google and this forum when my PCP is busy worrying about everybody else on her panel with “real” problems.
“Sustained improvement in sexual function after 12 months of tadalafil administration is associated with increased T:E ratio mainly related to reduction of E levels. We hypothesize that androgen-estrogen cross-talk and possible inhibition of aromatase activity during chronic exposure to tadalafil “
Interesting effect of tadalafil—lower estrogen. I’m surprised
You will also find the benefits of a smaller prostate, which is something you’ll be very thankful for in your fifties, sixties and seventies.
I have been on finasteride since I was 32, so almost 34 years. My urologist says my prostate is amazing he can hardly find it. At 66 no issues in prostate… urine flow… or my nut load.
So you’ll keep your hair, you’ll have a better functioning prostate, sex and recently they discovered that finasteride seems to have an effect on cholesterol in one’s blood, so maybe slow down your arthrocleurosis, plaque in your heart and arteries.
{kind=link}