Thanks for the input. Lipid increase is my main concern with rapa usage and I plan on checking this summer at the 6-month mark. My lipids were excellent in December prior to my start, so hopefully there’s no or minimal impact. My diet and workout routine are extremely consistent which will help with the comparison.
Thanks for your input. I was sure I was immune to changes in lipids. I train 10 hours per week, walk 10k steps per day, eat 60g fibre per day, less than 5% of diet SFA, take 15g psyllium per day, etc etc etc. however, clearly there is no lifestyle that can overcome the lipid raising effects for me. However, I’m sure there are a few caveats:
-
I’m sure it’s dose dependent. Maybe my 3mg+GFJ+EVOO ends up being 18mg and that’s why such a sharp increase.
-
As with all things - it will be highly bio individual. No two individuals react exactly the same to an intervention. Maybe I’m just predisposed.
Either way, I will be interested to see your results so please keep us posted ![]()
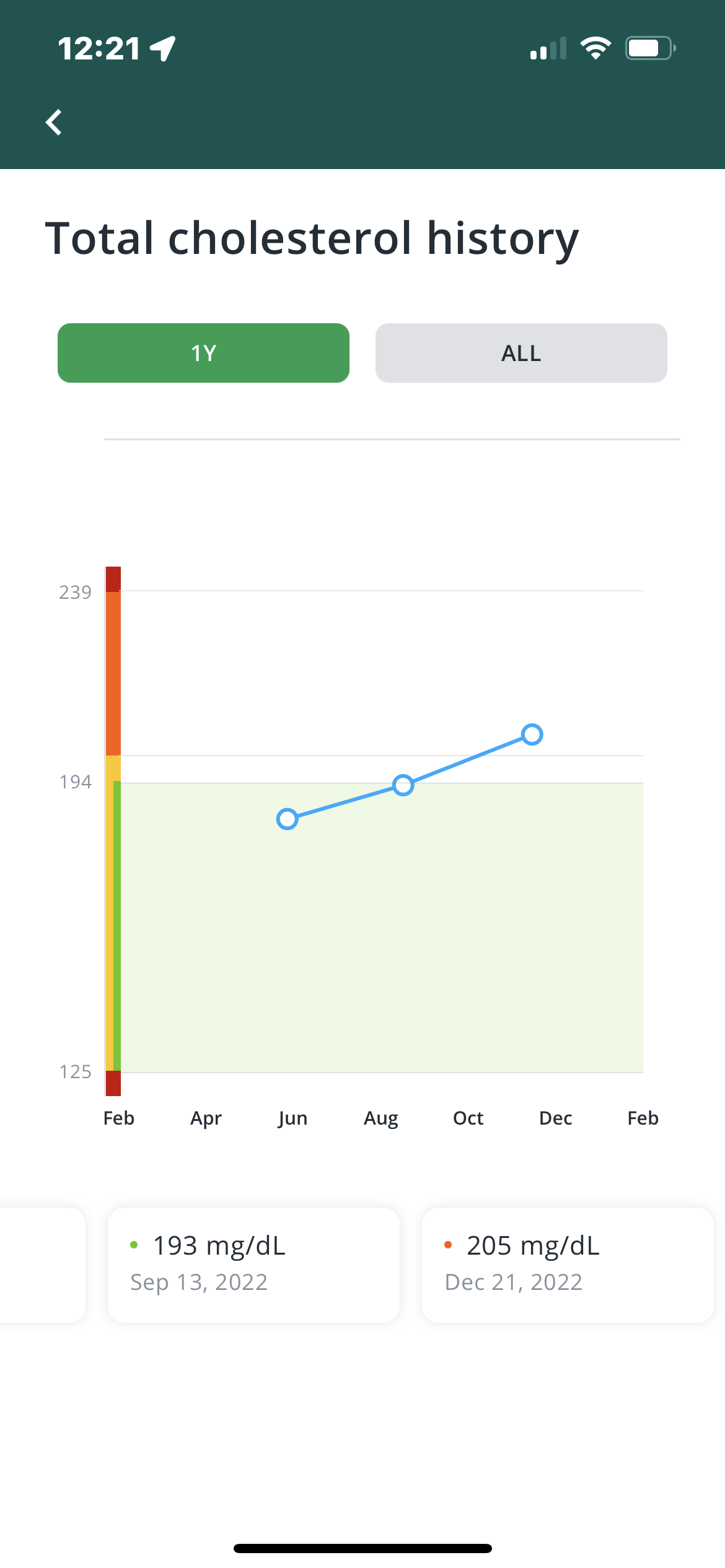
Obviously, there are lots of variables in our lives. My n of 1, is about a 20-30% increase in lipids across the board after being on Rapa.
1 Like
Ok, so example of the problem with n of 1 studies. In addition to Rapa I was also trying an SGLT2 which can raise cholesterol. So, too many variables. Gonna stop the SGLT2.
My cholesterol has def increased since beginning Rapa (6 months in now - 8 mg a week).
My plan for the next blood test is to take a 3 week Rapa vacation then test to see if this has a positive impact….
For everolimus it seems the default standard of care for raised lipids is a statin. See this thread Everolimus instead of Sirolimus / Rapamycin? Anyone else trying? - #80 by RapAdmin
Taking a statin is a terrible idea. Why induce damage on your body if your purpose is trying to live longer. We dont even have hard evidence ldl, does more then carry energy through the body. Why does every major illness happen below an ldl of 100, why is low ldl a death sentance for the elderly? Why does the bell curve point to the longest life span with an ldl at 130.
Its obvious rapa extends life in every animal model that exists. Maybe ldl has to deal with a healing mechanism and big pharma statins arent your answer. Maybe the fact that rapa extends lifespan and raises your ldl means ldl is not the culprit? If you are basing all your info on cherry picked blue zone studies by a faudster who based his info on how his wife felt eating vegetarian, maybe rapa wont save you.
Let rapa do its thing and what ever you do dont take statins. Why take rapa just to destroy your kidneys and liver, taking statins at 30… Better hope the anti rejection organ tech comes soon… Look at the old guy always posting on here taking rapa wondering why his bio age is aging more rapidly… Wonder what he does that could offset the rapa… Statins… Duh
1 Like
Yeah, that does seem to be the case. I do still take Metformin but when I started taking Rapa dropped back to 500mg a day (instead of 1g that I used to take). Don’t know why I did this….anyway, after the last blood test, I’m back up to 1g. Hoping this might help a little….
https://www.ahajournals.org/doi/full/10.1161/ATVBAHA.120.315708
Im out on metformin since seeing peters pod showing the studies where manipulated…
If your worried you should take tricaprin and burdock root over a statin…
1 Like
Welcome to the forum, but gold standard randomized controlled trials and genetic studies suggests otherwise.
Statins are off patent and very inexpensive, there is no money to be made there. Mice do not die from ASCVD, while that is the number one killer in humans. So you can’t use mice studies to establish evidence for rapamycin and ASCVD and especially LDL cholesterol. There are excellent human trials for the latter.
It has been discussed at this topic, you can press summarize as it’s a very long thread:
Rapamycin and risk of cardiovascular disease
I suggest you read more about this topic. If that doesn’t interest you, find a good doctor instead.
1 Like
Really there arnt excellent human studies… And really evidence points that people fed ldl lowering drugs dont live longer…
Ive read that thread… Thru
1 Like
The evidence do show that people who take statins live longer, in that thread you can find a meta analysis of randomized controlled trials showing a reduction in all cause mortality, stratified for LDL lowering.
1 Like
Hi Chance welcome to the forum.
I don’t know if you have been reading the forum much before posting but i do encourage you to do so just so you know what has been discussed recently and more generally how we operate.
Since we are a medically oriented site and we don’t know other members medical situations indepth (and as most of us are not trained doctors or PHDs in biology… Though many of our contributors do/are). We have a policy of not telling other people what “they should do”…
Its also generally helpful to treat others here with the type of respect you would want to receive.
As many of the longevity researchers like to emphasize to me… Its best to come to the field with some significant humility. Biology is extremely complex, for all of us its an ongoing process of learning, and also testing, and trial and error.
We qive a lot of weight here to science and clinical studies…and ideally good data. And less to opinions without facts to back them up.
We had a discussion a few weeks ago about tricaprin. It is interesting early research but still really early.
See here Tricaprin supplementation appears to reverse a certain type of atherosclerosis
4 Likes
For me personally, this all comes down to my own risk/reward analysis based on the literature.
I personally am not happy walking around with raised ApoB. I am aware of the mechanisms by which rapa may attenuate its own ‘side effects’ through modulation of inflammation etc but I personally think the data are strong around the causal effect of ApoB/Non-HDL and atherosclerosis. ASCVD is probably my biggest risk of mortality - so avoiding this disease should be my primary concern if trying to extend lifespan.
Therefore, I prefer to remain cautious about lipid modulation and prefer to keep them as low as possible.
If I can reduce/cycle/modify my rapa protocol in a way that keeps lipid numbers in optimal range then I am happy with that. I’m personally not open to starting a lifetime statin meds at 30 y/o. Not that I believe they’re inherently dangerous (IMO they have a good safety record if well tolerated) - but it just doesn’t sit well with me mentally (personal).
This is something I will figure out as I move through the process of having a washout period and titrating again through different dosages.
I am also opening up the possibility (to myself) of cycling rapa and taking some lipid lowering Rx during the cycle. If this was something I wanted to proceed with, I would be pushing hard to get PCSK9 inhibitor from my GP.
3 Likes
How much EVOO? It may be plant-based but it’s 100% lipid. There is potentially a lot of fat content in vegetarian diets. Also, do you know your family history? Hypercholestoremia is often heritable.
FWIW
If you have not seen/read, review the following posting.
1 Like
I eat less than 5% SFA per day as confirmed by Chronometer. I eat a balanced diet - high in MUFA and PUFA - low in SFA.
My lipids were normal pre rapa while eating the same diet as now. This is not diet induced - but Rapamycin induced. And this should not be too surprising given the data:
During sirolimus administration, mean total plasma cholesterol increased from 214 mg/dl to 322 mg/dl (+50%; range 25–92%); LDL-cholesterol levels followed a similar pattern. Mean triglyceride level rose from 227 to 432 mg/dl (+95%; range 9–254%). ApoB-100 concentration rose from 124 to 160 mg/dl (+28%; P < 0.05). ApoC-III level increased from 28.9 to 55.5 mg/dl, +92%; (P < 0.013). These lipid and apolipoprotein changes were found to be repeatable, reversible, and dose dependent.
So this is not in question. Still a surprise for me because my mindset is just too egotistical and I believed that I’m above all side effects. Clearly not! (Haha - joking btw).
3 Likes
I eat a very low SFA diet as well, but I’ve started with rosuvastatin three times a week, a very low dose of 1 mg/day can lower LDL by around 30% IIRC, low dose ezetimibe around 14% IIRC.
Rosuvastatin was associated with highly significant dose-dependent reductions in LDL cholesterol compared with placebo (p <0.001); decreases ranged from 34% (1 mg) to 65% (80 mg).
Rosuvastatin has a harder time crossing the BBB compared to other statins which might reduce possible long term speculative cognitive side effects. I started because I think it’s impossible to have a low enough LDL without it (below 5th percentile apoB, or nearing 30 mg/dl), especially with genetic variation (I am in the 94th percentile for LDL genetically).
I think low dose statin + ezetimibe probably will work well with rapa. Higher dose or PCSK9i required if LDL/apoB doesn’t decrease enough, obviously.
Any differentiation between ‘natural’ vs. unnatural medications/therapies has been sucked into a black hole for me personally. The ‘appeal to nature’ fallacy isn’t good, IMO.
2 Likes
Is a PSCK9 inhibitor superior to statins? Anyone have a good comparison of the risk reward between the two?