Im out on metformin since seeing peters pod showing the studies where manipulated…
If your worried you should take tricaprin and burdock root over a statin…
1 Like
Welcome to the forum, but gold standard randomized controlled trials and genetic studies suggests otherwise.
Statins are off patent and very inexpensive, there is no money to be made there. Mice do not die from ASCVD, while that is the number one killer in humans. So you can’t use mice studies to establish evidence for rapamycin and ASCVD and especially LDL cholesterol. There are excellent human trials for the latter.
It has been discussed at this topic, you can press summarize as it’s a very long thread:
Rapamycin and risk of cardiovascular disease
I suggest you read more about this topic. If that doesn’t interest you, find a good doctor instead.
1 Like
Really there arnt excellent human studies… And really evidence points that people fed ldl lowering drugs dont live longer…
Ive read that thread… Thru
1 Like
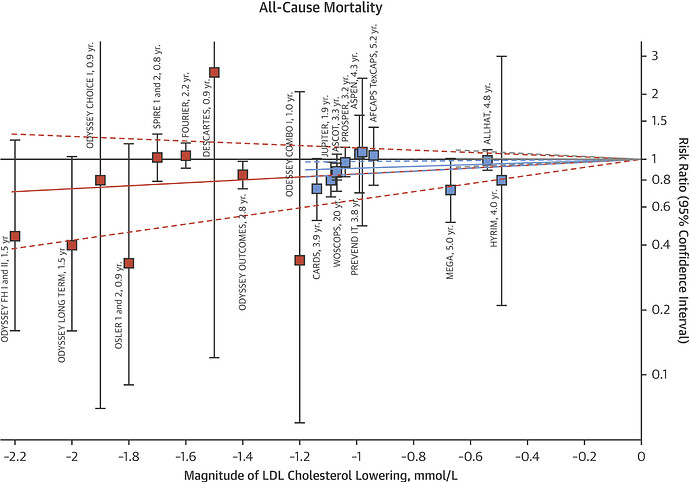
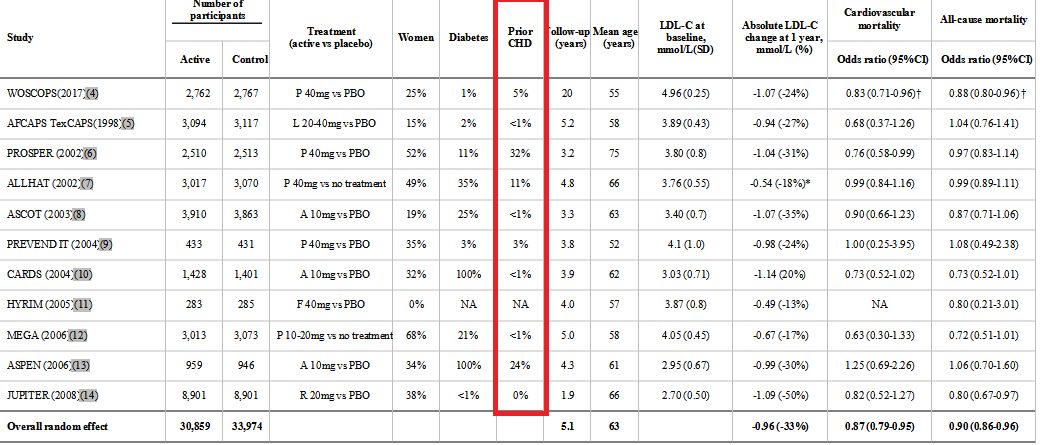
The evidence do show that people who take statins live longer, in that thread you can find a meta analysis of randomized controlled trials showing a reduction in all cause mortality, stratified for LDL lowering.
1 Like
Hi Chance welcome to the forum.
I don’t know if you have been reading the forum much before posting but i do encourage you to do so just so you know what has been discussed recently and more generally how we operate.
Since we are a medically oriented site and we don’t know other members medical situations indepth (and as most of us are not trained doctors or PHDs in biology… Though many of our contributors do/are). We have a policy of not telling other people what “they should do”…
Its also generally helpful to treat others here with the type of respect you would want to receive.
As many of the longevity researchers like to emphasize to me… Its best to come to the field with some significant humility. Biology is extremely complex, for all of us its an ongoing process of learning, and also testing, and trial and error.
We qive a lot of weight here to science and clinical studies…and ideally good data. And less to opinions without facts to back them up.
We had a discussion a few weeks ago about tricaprin. It is interesting early research but still really early.
See here Tricaprin supplementation appears to reverse a certain type of atherosclerosis
4 Likes
For me personally, this all comes down to my own risk/reward analysis based on the literature.
I personally am not happy walking around with raised ApoB. I am aware of the mechanisms by which rapa may attenuate its own ‘side effects’ through modulation of inflammation etc but I personally think the data are strong around the causal effect of ApoB/Non-HDL and atherosclerosis. ASCVD is probably my biggest risk of mortality - so avoiding this disease should be my primary concern if trying to extend lifespan.
Therefore, I prefer to remain cautious about lipid modulation and prefer to keep them as low as possible.
If I can reduce/cycle/modify my rapa protocol in a way that keeps lipid numbers in optimal range then I am happy with that. I’m personally not open to starting a lifetime statin meds at 30 y/o. Not that I believe they’re inherently dangerous (IMO they have a good safety record if well tolerated) - but it just doesn’t sit well with me mentally (personal).
This is something I will figure out as I move through the process of having a washout period and titrating again through different dosages.
I am also opening up the possibility (to myself) of cycling rapa and taking some lipid lowering Rx during the cycle. If this was something I wanted to proceed with, I would be pushing hard to get PCSK9 inhibitor from my GP.
3 Likes
How much EVOO? It may be plant-based but it’s 100% lipid. There is potentially a lot of fat content in vegetarian diets. Also, do you know your family history? Hypercholestoremia is often heritable.
FWIW
If you have not seen/read, review the following posting.
1 Like
I eat less than 5% SFA per day as confirmed by Chronometer. I eat a balanced diet - high in MUFA and PUFA - low in SFA.
My lipids were normal pre rapa while eating the same diet as now. This is not diet induced - but Rapamycin induced. And this should not be too surprising given the data:
During sirolimus administration, mean total plasma cholesterol increased from 214 mg/dl to 322 mg/dl (+50%; range 25–92%); LDL-cholesterol levels followed a similar pattern. Mean triglyceride level rose from 227 to 432 mg/dl (+95%; range 9–254%). ApoB-100 concentration rose from 124 to 160 mg/dl (+28%; P < 0.05). ApoC-III level increased from 28.9 to 55.5 mg/dl, +92%; (P < 0.013). These lipid and apolipoprotein changes were found to be repeatable, reversible, and dose dependent.
So this is not in question. Still a surprise for me because my mindset is just too egotistical and I believed that I’m above all side effects. Clearly not! (Haha - joking btw).
3 Likes
I eat a very low SFA diet as well, but I’ve started with rosuvastatin three times a week, a very low dose of 1 mg/day can lower LDL by around 30% IIRC, low dose ezetimibe around 14% IIRC.
Rosuvastatin was associated with highly significant dose-dependent reductions in LDL cholesterol compared with placebo (p <0.001); decreases ranged from 34% (1 mg) to 65% (80 mg).
Rosuvastatin has a harder time crossing the BBB compared to other statins which might reduce possible long term speculative cognitive side effects. I started because I think it’s impossible to have a low enough LDL without it (below 5th percentile apoB, or nearing 30 mg/dl), especially with genetic variation (I am in the 94th percentile for LDL genetically).
I think low dose statin + ezetimibe probably will work well with rapa. Higher dose or PCSK9i required if LDL/apoB doesn’t decrease enough, obviously.
Any differentiation between ‘natural’ vs. unnatural medications/therapies has been sucked into a black hole for me personally. The ‘appeal to nature’ fallacy isn’t good, IMO.
2 Likes
Is a PSCK9 inhibitor superior to statins? Anyone have a good comparison of the risk reward between the two?
This literally the only study people point to, and the “benefits” dont really even pass stat error…
Look i do beleive if you have a bunch of people who are focused on there health… The low ldl group is obv, mostly vegetarians… Then you have a control pop of meat eaters… That are most likely sad diet that break the general num one rule. If you eat a high fat diet, you cant eat carbs/spike glucose. Sat fat and carbs dont mix. The sad dieters im sure also had high tri and apob
So basically you have a control group of vegetarians who are health conscious and then a control group of sad eaters who most likely eat junk food, smoke and dont excercise… And the ‘difference’ and this is the statin studies also are really not stat significant…
Arnt statins like 1 percent lol…
If you took keto or carnivore eaters, who prob have high ldl over 150 but low tri and low apob… And compare them to the healthy eaters, i believe will be obvious that they will live longer fuller lives, with more muscle mass and less inflamation. Dont alot here believe it is now obvious that carbs become sugar, spike glucose and cause disfunction in endo cells.
Totally seperate topic, but isnt it amazing what ucsd is doing with these hydogels… Im more excited about this then anything…
I wish i could seed invest in ventrixbio
That is false, the study I am referencing had a p-value of 0.009 which means it was statistically significant, much more than the typical 0.05 threshold.
It was also done in people without pre-existing cardiovascular disease.
Risk ratio for a 0.5 mmol/l lower LDL cholesterol: 0.95 (0.92–0.99); p = 0.009
Blue is the statin studies.
If you have a high LDL, you probably will have a high apoB, so that doesn’t make sense. But sure, apoB is a better measurement, and if you can keep apoB below 5th percentile for a long time you’re good.
1 Like
The clinic that ran my lipid panel got in touch and asked me if I want to take either ezetimibe or rosuvastatin. Told them I would go away and think about which option I want to choose.
Led me down an interesting train of thought. What’s the best medication to attenuate hypercholesterolemia induced by Rapamycin. My way of thinking (guessing ![]() ) would be that ezetimibe would probably be less potent since it works more on cholesterol absorption at the level of the intestine - where as rapa is upregulating the liberation of fatty acids - so more receptors (statin) would be more beneficial.
) would be that ezetimibe would probably be less potent since it works more on cholesterol absorption at the level of the intestine - where as rapa is upregulating the liberation of fatty acids - so more receptors (statin) would be more beneficial.
Any thoughts on this?
FWIW - I am getting the rosuvastatin (because I can) but not taking anything. I will test again in 1 month and get a new baseline after rapa washout before deciding the next steps. I prefer not to play polypharmacy honestly. Will probably just find a dose of rapa I can tolerate ultimately.
I keep hearing on doctor podcasts (while I am walking/working out, hence why I don’t have the basis research paper references — sorry about that) that while LDL levels have a correlation with CVD (and many might argue it is a lower order correlation, albeit highly studied) the “damaging” LDL is the many small LDL particles which is why LDLp (particle count) has a stronger and higher-order correlation to CVD than a basic LDL reading; the belief was that the larger LDL is “beneficial”, bringing energy and building LDL and cholesterol around the body. A low Triglyceride/LDL is supposedly correlated to lower LDLp, and suggests more “larger” LDL particles as a percentage which may not be the arterial-damaging LDL which we are worried about (and instead might be useful energy/building blocks LDL and cholesterol around the body), and why TG/LDL has a solid higher-order correlation to CVD (high TG yields more small LDL particles and thus higher LDLp). Lower TG/TC (or TG/LDL) seems to be correlated with lower inflammation in many cases. Again, just what I’ve been hearing consistently from doctor podcasts (if it’s critical I’ll try to find the references at some point).
So my questions are:
-
Does this make sense?
-
Assuming #1 is true if Rapamycin can raise LDL levels and lower inflammation, is it lowering TG levels as well, and thus could be thought of as improving metabolic function with a larger percentage of “healthy” lower-risk LDL? If so, should we be worked up about LDL?
And 3) Again assuming #1 is true, do statins lower LDL indiscriminately (i.e. the “beneficial” larger LDL with the “dangerous” smaller LDL) or just the smaller “inflammatory”LDL? Or is this known/measured?
Thanks for the understanding.
Has anyone else used lithium supplement to cancel Rapamycin’s effects on lipid metabolism ?
Proc Natl Acad Sci U S A. 2019 Oct 15; 116(42): 20817–20819.
https://www.pnas.org/doi/full/10.1073/pnas.1913212116
A triple drug combination targeting components of the nutrient-sensing network maximizes longevity
ABSTRACT
Increasing life expectancy is causing the prevalence of age-related diseases to rise, and there is an urgent need for new strategies to improve health at older ages. Reduced activity of insulin/insulin-like growth factor signaling (IIS) and mechanistic target of rapamycin (mTOR) nutrient-sensing signaling network can extend lifespan and improve health during aging in diverse organisms. However, the extensive feedback in this network and adverse side effects of inhibition imply that simultaneous targeting of specific effectors in the network may most effectively combat the effects of aging. We show that the mitogen-activated protein kinase kinase (MEK) inhibitor trametinib, the mTOR complex 1 (mTORC1) inhibitor rapamycin, and the glycogen synthase kinase-3 (GSK-3) inhibitor lithium act additively to increase longevity in Drosophila. Remarkably, the triple drug combination increased lifespan by 48%.
Furthermore, the combination of lithium with rapamycin cancelled the latter’s effects on lipid metabolism.
In conclusion, a polypharmacology approach of combining established, prolongevity drug inhibitors of specific nodes may be the most effective way to target the nutrient-sensing network to improve late-life health.
1 Like
That was discussed in the two threads below:
Take note of the post of Livin, quoted below:
Do not take trametinib for longevity purposes. I worked on synthetic lethal chemo combinations in cancer at a startup for years. We tested this compound and it is not a good idea. The Erk pathway is very important for most epithelial cells. Stick to low risk acarbose and rapamycin combinations and do not consider trametinib. If you have melanoma or another type of solid tumor type then you could consider trametinib. Just trying to prevent you from causing long term damage.
3 Likes
I’m having a non-HDL test in 2 days - and interested to see the results since I’ve been on a 4mg weekly dose for rapa for the last 3 months. Last time I got a high non-HDL while on rapa - but at that time I was also getting side effects, likely because the dosage was too high. Will report back with the results in 1 week.
But with this test upcoming, it got me thinking about reopening the discussion of raised lipids on rapa and the risk vs reward trade off. It’s still unclear in my mind, and I’m open to more viewpoints from anyone who hasn’t chimed in on this subject already? Is there any quality more-recent literature? It’s something I think about a lot and never feel definitive either way.
2 Likes
It’s dose dependent and apoB is more accurate causal marker of risk.
1 Like