Those studies lasted from 4 weeks to 6 months…results reported after 3 to 12 months. Of course you won’t see much reduction in CV disease in that short a time…!
4 Likes
I mean seriously, what data would you need to see to accept my argument?
I bet you’re still taking resveratrol too ![]()
A. I’m not taking resveratrol
B, It would take a much longer trial of fasting…and a much longer period of follow-up to convince me.
“Why Many People Stubbornly Refuse to Change Their Minds”
You would be a perfect example of that.
I use TRF because I evolved into it. I have never said that anyone should follow my example.
What it does for me is, it keeps my weight in stasis without calorie counting. Yes, maybe I am an N=1, but it makes my life easier and I like the way it makes me feel.
Eat 5 meals a day if that makes you happy.
2 Likes
Yeah, a 12 month follow period gives incredible actionable data on IF impact on cardiovascular disease. ![]()
“I just follow the data”. Yeah, that’s some convincing “data”…
Are you f-ing serious (serious question)?
Does this forum not have an ignore button to filter out worthless content?
2 Likes
Nope. Just skip over the comments/people you don’t agree with or don’t want to read.
2 Likes
Suggesting a Chocrane meta analysis and a Peter Attia video clip are ‘worthless’ is just silly. It does however highlight the considerable power of cognitive dissonance.
A longevity trial of resveratrol in humans has never been performed. I look at the best available research and am thoroughly unconvinced of its benefits. I then listen to expert opinion and they confirm my interpretation. Why is this any different? To take the opposite position is head spinningly bizarre.
Now, if you practice TRF because you ‘like it’ or it fits your lifestyle, crack on and good luck to you. Just don’t start claiming it will increase lifespan or induce autophagy.
And finally, I followed TRF for a couple of years after Martin Berkhan introduced the ‘lean gains’ idea to the fitness community. This was around 2011 so way before it became popular in the mainstream. I certainly lost weight but my cycling performance suffered…so I moved on.
OK guys - sometimes I think we just need to agree to disagree.
I can see very valid points on both sides of this argument. I think all the people here have made good points that really add to my understanding about the issues at hand. Ultimately we are all going to have slightly different criteria and weights on any given evidence we see, and have different risk/reward profiles we follow in deciding to use a given supplement, drug or therapeutic approach (like TRF or fasting).
Its entirely expected that we are not going to have the same opinion on some things - so please don’t let it bother you, don’t take it personally if someone else doesn’t share your valuing / weighting , etc. of any given piece of evidence.
I think our goal of maximizing our benefit from the interactions here is if we present the best evidence we think we have seen for a given topic/therapy, review and poke holes in the evidence that others present and have a civil discussion about how we interpret or evaluate all the evidence.
I view it a little bit like the college debate team efforts I used to participate. In discussion like these - a two round cycle of stating a case and presenting evidence, stating a counter case and presenting counter evidence, then a few backs and forth on the relative merits of the evidence - then let it go until new research comes up (and we know if will very soon) and we can reevaluate the issue.
As I’ve heard some state… strong options loosely held… and open for update, seems like a reasonable approach to all these discussions.
Ultimately that is all we can do - we present our “case” for a given issue, then every individual that visits here will need to evaluate and make their own decisions.
Given the state of knowledge in pretty much all the areas we cover on this site, reasonable people can disagree.
I’m all for healthy debates and discussions. But please don’t make things personal - focus on the data and research papers, and the issue at hand.
And, if people still disagree - which I expect to be the case in most situations because we all have our own biases from years of living and experiences - no problem - just let it go and move on to the next thread.
Thanks !
3 Likes
ok, I see where you are coming from. From the lens of high athletic/peak competitive performance, if in doing TRF, you loose muscle mass/strength, you will suffer. And your argument is, it’s virtually impossible to do TRF whilst maintaining muscle mass/strength AND maintain this peak. You appear younger and in a high competitive phase of your life, understood. I had a triathlete friend who went on mild CR/TRF, he lost weight (NO resistance exercise) and his run component significantly improved, but he felt his cycle diminished. He paid no attention to muscle mass; he feared growing lean muscle build would impact his running. He didn’t engineer the intervention. Again, PEAK performance was his only focus.
But the vast majority of us in this forum are here for LONGEVITY. We are more highly motivated with extracting the benefits of some CR/TRF, BUT…not at the expense of maintaining muscle mass/strength/frailty (at least for me n=1) because muscle mass/strength IS associated with longevity (see below references).
So the conundrum.
So if weight loss is associated with the TRF regiment, it MUST come from body fat, and not at the expense of muscle mass/strength, thus, resistance exercise is critical to the protocol.
This is the CR/TRF risk with those not understanding the full scope of managing diet, fasting, weight, resistance exercise, and monitoring muscle/fat (DEXA). Note I did not include a peak athletic performance parameter…that is not our goal with longevity.
It’s completely obvious, humans don’t need to eat 3x/day or every day to survive…we have fat reserves, basal minimum glucose for brain and key organs, and ketogenic metabolism to maintain high level function. But the body will draw on reserves to maintain metabolism, there is NO doubt. It’s the “engineered” protocol of harnessing both TRF whilst maintaining muscle functionality that is absolutely critical for human (vs shrivelled and decimated CR mice for a longevity statistic). Going on TRF to become thin and FRAIL is not a recipe for longevity. You want to become LEANER, more MUSCULAR, and STRONGER. Frailty is absolutely a path to a shortened lifespan.
I continue to tweak diet on 24hr fasts, with very gradual weight loss, yet growing more muscle and strength with increasing resistance exercise, trading body fat for muscle. I am on pause re incremental fasting duration, whilst I explore Rapamycin and other interventions.
References:
Muscle mass index as a predictor of longevity in older adults (2014)
"In adjusted analyses, total mortality was significantly lower in the fourth quartile of muscle mass index compared with the first quartile: adjusted risk ratio 0.81 (95% confidence interval, 0.71-0.91) and adjusted hazard ratio 0.80 (95% confidence interval, 0.66-0.97).
Conclusions: This study demonstrates the survival predication ability of relative muscle mass and highlights the need to look beyond total body mass in assessing the health of older adults."
Strength, But Not Muscle Mass, Is Associated With Mortality in the Health, Aging and Body Composition Study Cohort (2006)
Conclusion: Low muscle mass did not explain the strong association of strength with mortality, demonstrating that muscle strength as a marker of muscle quality is more important than quantity in estimating mortality risk. Grip strength provided risk estimates similar to those of quadriceps strength.
Association between muscular strength and mortality in men: prospective cohort study
https://sci-hub.se/https://doi.org/10.1136/bmj.a439
“Conclusion: Muscular strength is inversely and independently associated with death from all causes and cancer in men, even after adjusting for cardiorespiratory fitness and other potential confounders.”
Associations of Muscle Mass and Strength with All-Cause Mortality among US Older Adults
Conclusions: Low muscle strength was independently associated with elevated risk of all-cause mortality, regardless of muscle mass, metabolic syndrome, sedentary time, or LTPA among US older adults, indicating the importance of muscle strength in predicting aging-related health outcomes in older adults.
Associations of muscle mass, strength, and quality with all-cause mortality in China: a population-based cohort study
Conclusion: Low muscle mass, grip strength, and arm muscle quality are all associated with short-term increased risks of mortality, indicating the importance of maintaining normal muscle mass, strength, and quality for general Chinese adults.
At a minimum, maintain strength, but I am going to hedge and give myself a reserve (lesser frailty too) and greater odds by skewing to both higher mass and strength. Getting to higher muscle mass will force an increase in strength by increasing reps load to failure, not just volume.
You know the 75 yr old phenoytype I’m referring to:


1 Like
Peter might be wrong here…
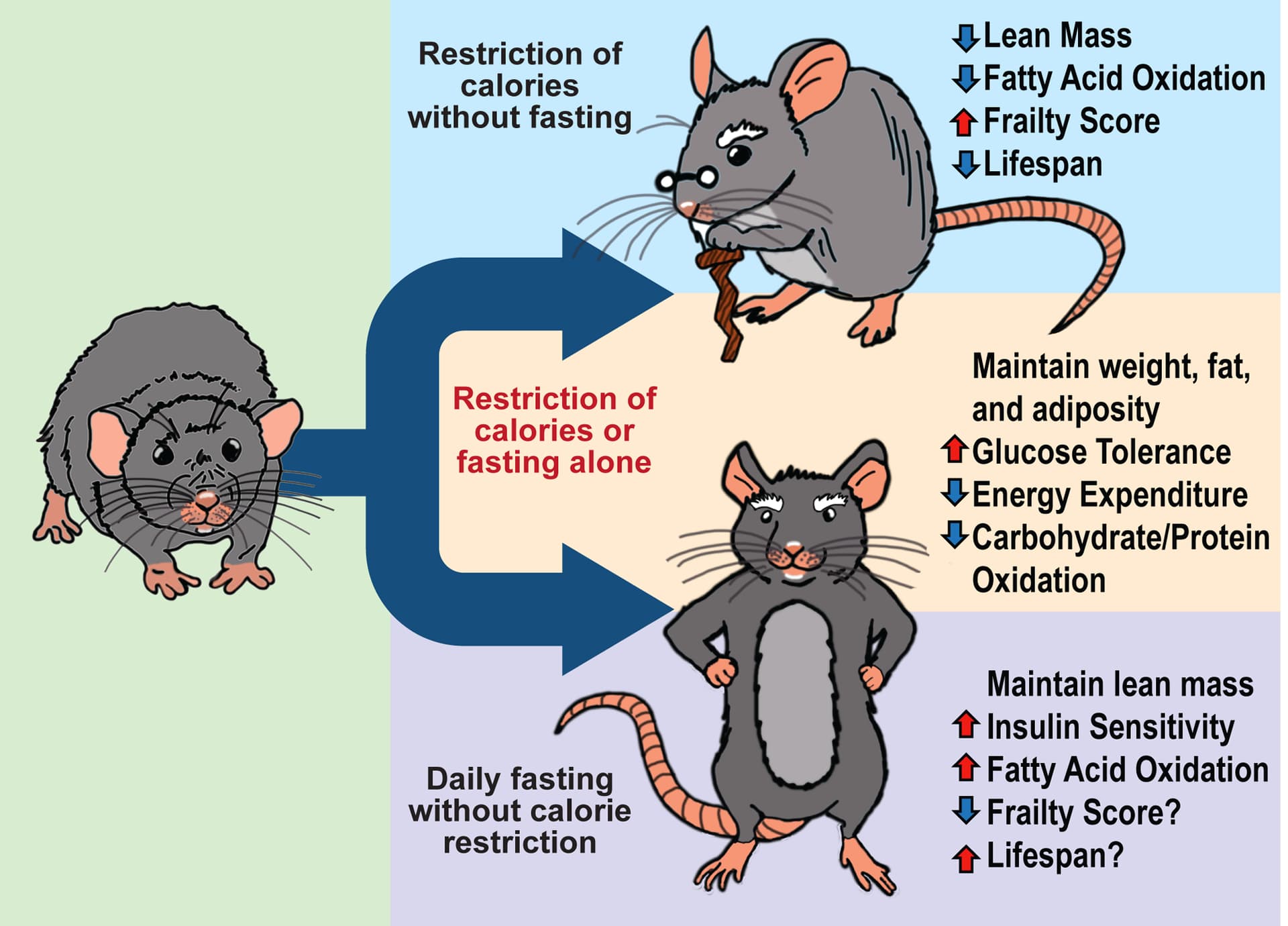
Fasting drives the metabolic, molecular, and geroprotective effects of a calorie restricted diet in mice (Lamming, 2018)
“Calorie restriction (CR) promotes healthy aging in diverse species. Recently, it has been shown that fasting for a portion of each day has metabolic benefits and promotes lifespan. These findings complicate the interpretation of rodent CR studies, in which animals typically eat only once per day and rapidly consume their food, which collaterally imposes fasting. Here, we show that a prolonged fast is necessary for key metabolic, molecular and geroprotective effects of a CR diet. Using a series of feeding regimens, we dissect the effects of calories and fasting, and proceed to demonstrate that fasting alone recapitulates many of the physiological and molecular effects of CR. Our results shed new light on how both when and how much we eat regulate metabolic health and longevity, and demonstrate that daily prolonged fasting, and not solely reduced calorie intake, is likely responsible for the metabolic and geroprotective benefits of a CR diet.”
For this group, the truly relevant study of fasting and TRF would be in humans (at various ages) who “do everything right” ie proper weight, low body fat, the right carbs, the right fats, sane protein intake, zone 2 exercise, strength train, etc. I would like to know the potential benefits to these people. I do believe Matt Kaeberlein and Peter Attia when they say that there are flaws in most studies and they do not prove what they purport to prove (for humans anyways). I do believe there is some benefit to to TRF and fasting as I believe Peter Attia still does it. I do believe that the benefits are less than the most vocal supporters of it believe. I don’t believe that the practices necessarily have a negative effect on muscle mass retention as I have practiced both throughout my 60’s and have not loss any muscle. The attached is a recent photo of me at 68.

We are certainly not going to be able to decide the issue here.
2 Likes
This has been an interesting discussion/debate. I am another N-of-1. I’ve been educating people about the importance of working to maintain muscle mass for a long time. Here is a link to my blog post: #1 Factor for Heathy Aging: Maintain Your Muscle Mass. Longevity Blog | Ross Pelton | The Natural Pharmacist
Since I started rapamycin about 9 months ago…and concurrently started doing a 16:8 IF protocol most days, I’ve lost about 15 pounds (mostly visible loss of visceral abdominal fat (ie. love handles). At the same time, I increased my dedication to do strength training 4 or 5 times a week. I"m lifting heavier weights now than I did/could a year ago. I’m not trying to bulk up, just trying to maintain a nice plateau of strength & body composition for myself as I approach my 80th birthday.
1 Like
What I got from the Cochrane review is simply very low to low certainty as to whether CR vs TRF is “better” in the short to medium term for the easy-to-measure metrics. What matters to me is does it demonstrably affect my labs more so when doing multiple crossovers TRF 16/8 at 10-6pm with mild CR vs mild CR. The evidence is very low for humans but if the labs are telling me it’s better with multiple crossovers - I don’t see a big issue for me personally. The risk is minimal and if it’s due to a placebo then so be it.
I’d say the same about rapamycin. The evidence is so low in humans that it is not even a weak recommendation
What we know with moderately high to high certainty about all diets is Mediterranean diet has the most evidence with moderate effect in humans. Everything else has low to very low certainty of evidence in humans. But that’s because more complex long term diet studies are absolutely difficult to fund, design and conduct properly
That’s basically expected for any review of diets - it does not disprove much. I don’t bother with a Cochrane review on any diets. I’ll also note that TRF highly depends on the methodology.
What this review says is:
-
TRF is not a particularly good weight loss tool as opposed to CR in the short or medium term. (Agree, never thought of it as one, if anything, I’m not trying to lose weight)
-
TRF in the short and medium term does not seem to have a large effect on insulin resistance as opposed to CR (Agree, this has been my experience too)
“We are uncertain about the effect of IF on glucose when compared to ad libitum feeding in the short term (MD -0.03 mmol/L, 95% CI -0.26 to 0.19; 95 participants; 3 studies; very-low-certainty of evidence) and when compared to CER in the short term: MD -0.02 mmol/L, 95% CI -0.16 to 0.12; 582 participants; 9 studies; very low-certainty; medium term: MD 0.01, 95% CI -0.10 to 0.11; 279 participants; 4 studies; low-certainty evidence).”
Will never know…at least until someone starts collecting mortality data down the road, and does some type of retrospective study.
But I’m holistic about multiple beneficial, stackable pathways and motivated…will throw everything at extending all cause mortality. THERE IS NO DO OVER
I’ll take that at 68!!
The devil is in the details. Can you provide more specifics re TRF interventions? You know, diet macros, calories, fasting duration, exercise, weight loss amount, etc
Did you ever do extended multi-day fasts (electrolytes) only? That’s sort of the broad basis of this TRF thread.
I have always controlled my weight and body fat level very well going back to age 13 when I started strength training. Since age 60 I have generally eaten during a 10 hour window each day. I continue this mostly as it is convenient and I find it a good way to keep my weight under control. I am not sure if it provides any special benefits compared to proper eating during a larger window each day. My diet is approximately 40% carb, 40% fat and 20% protein. All good fats (a lot of olive oil), virtually all low glycemic carbs and protein ranges from 100 to 120 grams, an average 110 grams of protein a day.
I have been heavily influenced by Peter Attia. I have aimed for a 3 day fast quarterly for each of the last 3 years and have actually completed 8 of them. I don’t believe they have had any lasting effect on my level of muscle mass (or body fat level for that matter). I have been concerned about loss of muscle and each time consumed powdered amino acids and a quantity of protein as soon as the 3 days were up. If I were more convinced about the benefits of longer fasts I would likely have less trouble doing them. There are a number of things I would do differently if I were convinced they it would be beneficial.
I am not sure if this has had an effect but I should say I have done a great deal of strength training more or less consistently since age 13 (51 of the 55 years – a few slip ups in my 20’s and 30’s). In my 30’s, 40’s and 50’s I did about 4 hours of strength training and 1 hour of cardio per week. In my 60’s I have stressed zone 2 training and cardio doing about 4 hours a week of cardio and less strength training, about 2 hours a week. Pretty much the same muscle mass has been there since my 30’s. It neither increases nor decreases. (It does look different though LOL).
1 Like
Cochrane meta anlyses are not worthless, but much as I like watching Peter Attia videos, Peter’s videos are just his current opinion and not scientific research by any stretch of the imagination. He may be a genius but is certainly no authority on the myriad of subjects his videos cover. So, while I respect Cochrane metadata, don’t spout Peter Attia’s Youtube videos as a scientific fact.
1 Like
Apparently Maveric78 pushed one of your buttons. Well you have pushed one of mine. There are very few scientific facts in any of this. There is a huge amount of conflicting information. I therefore seek the opinions of “experts”. If Peter Attia does not fit your definition of expert, Matt Kaeberlein should by virtue of his position at Washington University. Kaeberlein doubts the value of these dietary protocols. Actually Peter Attia, by virtue of being named co-chair of biotech SPAC probably does meet the definition of expert in the field. Those two and three or four other experts are what I rely upon for information as I do not have the ability to analyze what Cochrane meta analyses or most of the studies out there are truly proving, what the potential flaws in the studies are, and why they do not support the claims made by the authors. Furthermore, I am in no position to deal with the many conflicts between scientific studies. I rely on the opinions of others to help me form my own opinion.
1 Like
" I rely on the opinions of others to help me form my own opinion."
As do I. I guess it just comes down to whose opinions you want to listen to.
The field is littered with “expert” opinions of many famous researchers, including Nobel prize winners whose studies have proved to be flawed, especially when venturing outside of the area of their initial expertise. My life experience is that is good to question the so-called experts of the moment.
I am not trying to force my opinions on anyone else in this forum. My, opinions are just my opinions, I have never put myself forth as an expert on any of the topics we discuss here.
So, as I told Maveric, I don’t care if you eat 5 meals a day, one meal a day, or starve yourself fasting. I have only put forth the reasons I have chosen to do TRF. If you don’t like those reasons, that’s your prerogative.
I apologize. Actually I was just venting my personal frustrations. I wish there was more concrete information. Actually, I have some doubts as to whether I am accomplishing much of anything. Almost all women in the previous generation in my family made it to their late 80’s. Almost all men to their early 90’s. This without much of anything in the way of dietary or exercise interventions. Would they have lived appreciably longer with excellent diets and exercise regimes? Maybe. Maybe not.