“There are striking similarities in the inflammatory responses observed in patients with heart conditions and those experiencing cognitive decline. This suggests that damage to one organ, like the heart, may trigger an immune response that affects another, such as the brain,” Testai said.
Testai noted evidence of other mechanisms involved. The blood biomarker beta-amyloid, which is associated with Alzheimer’s disease, has been detected in cardiac tissue, where it is associated with cardiac dysfunction. The presence of beta-amyloid in both the heart and brain suggest a deep connection between the two systems.
Buntanetap is a drug under investigation for AD and PD. It inhibits the production of neurotoxic proteins and has been shown to improve cognition in early AD patients (NCT05686044) and halt cognitive decline in PD patients (NCT05357989). Interestingly, last month, the company behind it filed three patents for combination therapies with dulaglutide and sildenafil @DrFraser!
Recent preclinical studies have demonstrated that when buntanetap is combined with a GLP-1 agonist (such as Trulicity) or PDE5 inhibitors (such as Viagra), cognitive function in Alzheimer’s mouse models improves to levels beyond those observed in healthy controls. With these compelling results demonstrating strong potential for cognition-enhancing combinations, Annovis further strengthens its intellectual property portfolio through the filing of the following patents:
Buntanetap + Trulicity (dulaglutide, a GLP-1 agonist).
Buntanetap + Viagra (sildenafil, a PDE5 inhibitor).
Buntanetap + Trulicity + Viagra.
“Our early data suggests a strong synergistic effect from combining these drugs, resulting in significant cognitive enhancement,” said Maria Maccecchini, Ph.D., Founder, President, and CEO of Annovis Bio. “The combination of buntanetap with Trulicity and Viagra not only has the potential to restore cognition to healthy levels, but also to improve it beyond normal, offering new hope in the fight against dementia. Since buntanetap has completed Phase 3 studies as a standalone treatment, and both Trulicity and Viagra are FDA-approved, these combinations are well-positioned for Phase 3 human trials.”
We don’t have the preclinical data (and it’s in mice…) but it’s noteworthy that they chose dulaglutide (instead of exenatide, liraglutide, lixisenatide or semaglutide) and sildenafil (instead of tadalafil).
That being said, their stock is down 51% YTD so it might just be a desperate move to attract attention…
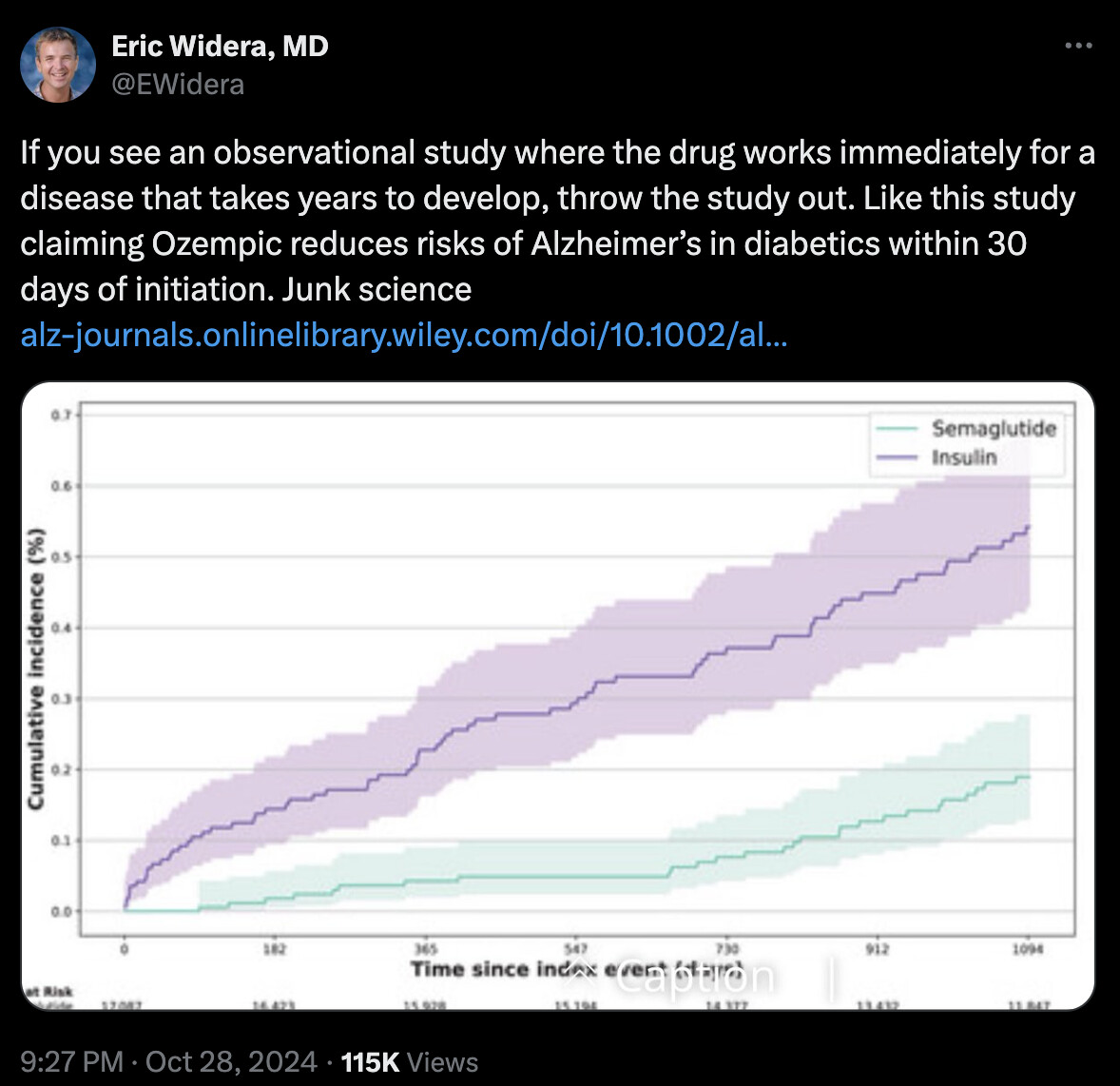
The separation between the curves begins within the first 30 days and continues to diverge, indicating the potential sustained benefits of semaglutide in delaying or slowing AD development.
[…]
Cumulative incidence curves began to diverge within 30 days and continued to separate thereafter, indicating semaglutide’s potential to delay or slow AD development with sustained effects.
I just think that this study is probably too good to be true. Thankfully, these catchy articles make the news and will push researchers to conduct RCTs on this.
Sorry, I meant people who are critiquing the paper/study
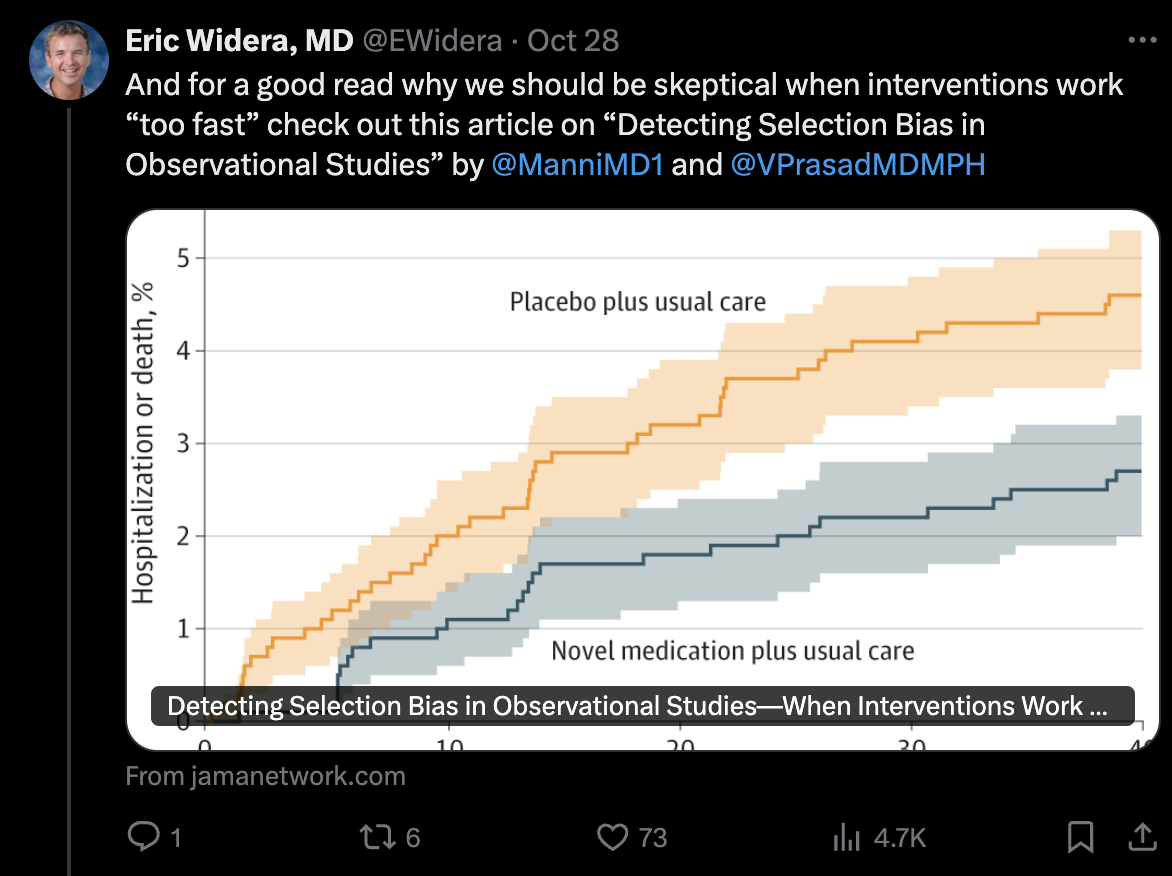
Are they explaining via mechanisms or logic why they think the data is not real / why changes should not be able to be seen in 30 days?
I could easily see there being real mechanist reasons for the data making sense already one month in
For example
Say there are two groups of mechanisms at play
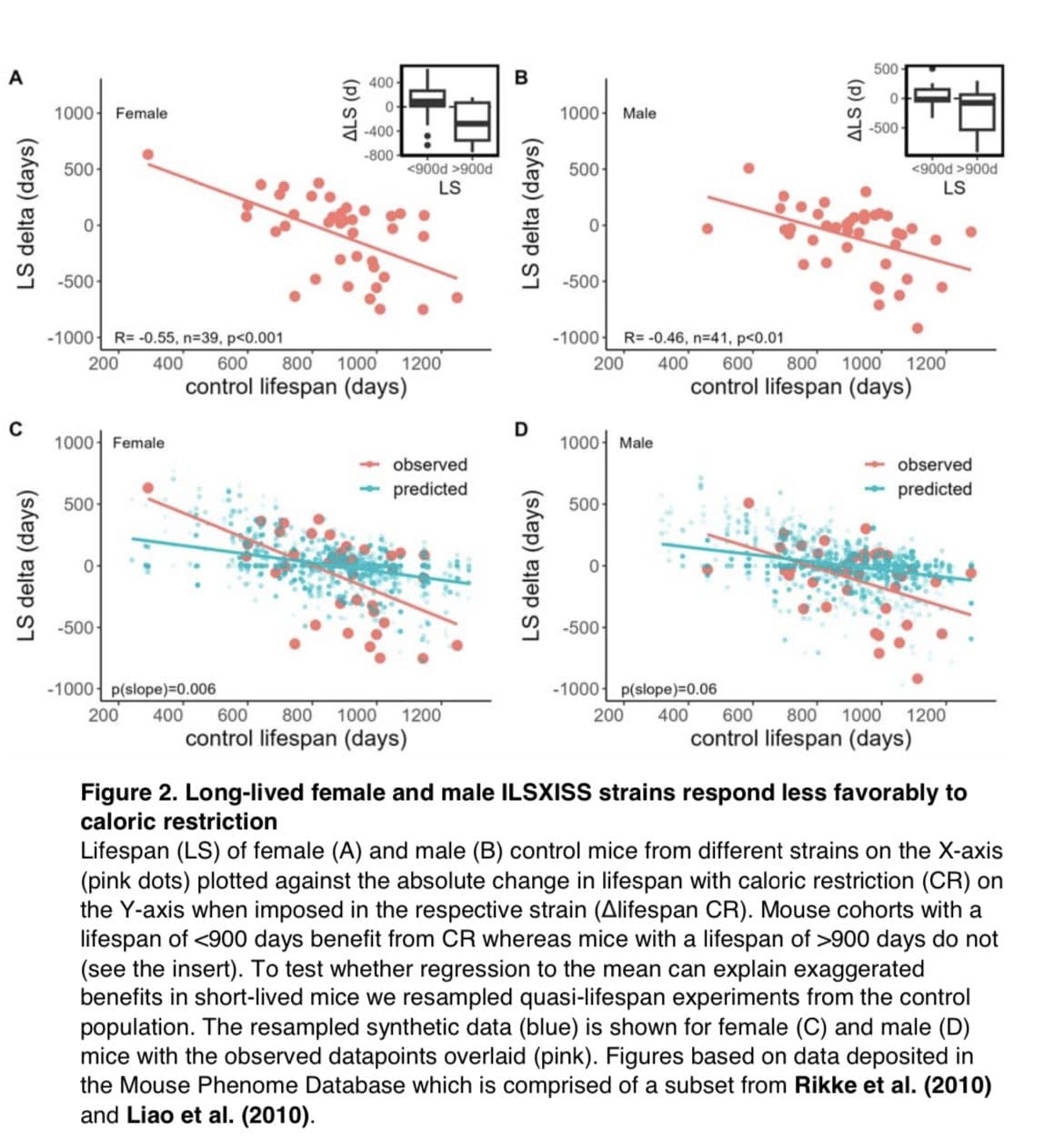
Early on GLP-s are decreasing inflammation, helping the brain balance and use more ketones, increasing brain insulin sensitivity and overall improve the metabolic condition of the brain (and overall organisms that the brain has as its environment). That could easily impact the things on the Y-axes on the graphs above.
Then over time above mechanisms continue (and compound) and perhaps a whole additional group of mechanisms (including many of our normal longevity pathways) have time fundamentally change the base state of people’s CNS and hence you keep getting a further separation vs the control group
As a analog thought experiment, if you’d take the things on the Y-Axis and ask if be shocked to see changes in 30 days if average non optimized developed world citizens where to just for real get optimal sleep, exercise and diet - many would see how there could be a change within a month vs the state average people were in before. Or what do you think?
The mechanism you describe is possible. But it seems unlikely to me that after just 30 days we would see a massive difference between two supposedly identical people: one on semaglutide and one on dulaglutide or dapagliflozin.
Some people say that some cases of delirium might be misdiagnosed as AD and that indeed lowering inflammation can stop delirium.
(That being said, I noticed some weird memory improvements a few days after starting semaglutide 3 mg, which is the non therapeutic starting dose… Just feeling mentally sharper and faster So maybe the study is correct and semaglutide is that magical. I want to believe but I’m skeptical…)
100%. Just saying that guy on twitter did not have a strong argument.
(You know I have question marks about GLP being longevity helpful in metabolically, weight and exercised optimized individuals (not including eg average American or people with specific risks) even if there may be such longevity benefits/pathways from eg SGLTi, Acarbose and Rapa in such optimized individuals.)
Yes, Neo, from your lips to god’s ears. Wouldn’t it be wonderful to have rct studies of these drugs in healthy individuals whose lifestyles (diet, exercise, supplements etc.) are close to optimal. Won’t happen, even though it would enlarge the market for those drugs that pass the test
So, everything has to be decided based on one’s particular situation (biomarkers and genetic background). Hopefully, in the future, you do a DNA methylation test, and you learn which genes to “tune,” and you take drugs accordingly.
We’ll learn a lot from these trials. You should check the list, there’s a lot of interesting stuff.
But we can already learn from trials on sick people as “sick” is usually defined arbitrarily. For instance, CKD = eGFR < 60 mL/min/1.73m2 (or sometimes 75) and T2D = HbA1C > 6.5%. And, if I remember correctly, SGLT2is lower the speed of decline of eGFR in people with T2D but without CKD and in people with CKD but without T2D, in both cases, irrespective of their baseline eGFR. And according to MR studies, “SGLT2 inhibition also protects eGFR” (SGLT2 inhibition, high-density lipoprotein, and kidney function: a mendelian randomization study 2024). So, it’s reasonable to assume that SGLT2i might also protect eGFR in people without CKD and T2D (or, at the very least, in those with pre-CKD and/or pre-diabetes). On top of that, all approved drugs are first tested in healthy volunteers (short-term, normal dose) and on rodent and non-rodent animals (long-term, high doses), so they’re safe-ish. In the case of SGLT2i, we know that canagliflozin and empagliflozin extend lifespan in mice, so probably very safe. So, as eGFR declines from age 30 and lower eGFR is associated with higher all-cause mortality ( Optimal Blood Pressure we Should Target? Systolic Under 110 or 100? - #392 by adssx ), there might be a case for using SGLT2i in everyone above 30yo? Or everyone with eGFR that starts declining? Or everyone with eGFR below 90? I don’t know, but that was just an example of a potential reasoning triangulating RCTs on sick people + MR + association studies in the general population + animal studies.
Above seems to be a way too black and white statement. At the minimum the jury is still out of think? Or do you feel that you actually know it does not work in long-lived animals (and I think you include humans in that)?
Personally think the evidence for CRON is at least as good as for any single FDA approved molecule
Below are some sources to start if you want to look at some of the literature:
Did you read the link I sent? I only mentioned CR in long-lived animals. Otherwise yes, CR is good. It increases longevity in animals on average. But are these animals “metabolically, weight and exercised optimized”? Or is the average animal like the “average American”? We always have this issue.
Risk mitigation begins at birth (or before birth with preimplantation genetic testing). We can model healthy diet and exercise for our children and encourage them to participate in sports that are relatively safer such as swimming or golf rather than more dangerous ones such as boxing or base jumping.
Eventually gene editing may provide one of the best ways to dramatically reduce the risk of Alzheimer’s. Until then, maintaining a healthy lifestyle and intermittent rapamycin use (in adults) seems like a great start.