Are we sure the pessimistic graph of Alzheimer’s disease rates is for the average population?
The note to the graph in Nature states, “ Kaplan–Meier curves were generated from Alzheimer’s dementia cases and cognitively unimpaired non-AD controls in the neuropathologically confirmed group. Y -axis represents the percentage of persons with each APOE genotype in the neuropathologically confirmed group who remained free from Alzheimer’s dementia. X -axis denotes age at death for controls and age at onset of cases, while replacing with age at death when age at onset was unavailable.”
It seems like the population in the graph wasn’t an average population, but I would appreciate help from others to assess this.
Also, this graph does not appear to be in line with other Alzheimer’s rate studies based on APOE status. Can anyone provide some clarity here?
Inflammaging and the Aging Brain: How Adiposity and Micronutrient Deficits Drive Cognitive Decline
Aging is characterized by creeping, low-grade systemic inflammation—often termed inflammaging—that chronically degrades cognitive reserve. A newly published pilot study provides a granular exploration into the nexus of dietary constituents, lifestyle behaviors, and progressive cognitive decline. The investigators demonstrated that older adults presenting with a high body mass index (BMI) exhibited significantly elevated plasma concentrations of pro-inflammatory cytokines, most notably tumor necrosis factor-alpha (TNF-α). Concurrently, altered interleukin-10 (IL-10) profiles were observed in these individuals, pointing to a severe disruption in basal anti-inflammatory regulation. Similar pro-inflammatory cascades, characterized by surges in TNF-α, interleukin-6 (IL-6), and IL-10, were prevalent among participants with low physical activity metrics.
When evaluating dietary habits against European Food Safety Authority (EFSA) dietary reference values, the findings introduced compelling anomalies. Participants ingesting excessive quantities of carbohydrates and polyunsaturated fatty acids (PUFAs) demonstrated demonstrably poorer cognitive performance across specific memory and learning domains. Conversely, individuals consuming higher amounts of saturated and monounsaturated fatty acids displayed superior cognitive function. This unexpected result challenges entrenched nutritional dogma regarding saturated fats and underscores an ongoing scholarly debate regarding the necessity of specific lipid structures for preserving neural integrity during advanced aging. Furthermore, inadequate overall caloric intake—frequently championed as a proxy for lifespan-extending caloric restriction pathways—was associated with significantly higher error rates in memory tests. This indicates a critical threshold where energetic deficits become neurologically deleterious rather than protective.
Specific micronutrient deficiencies also proved highly toxic to both inflammatory homeostasis and cognitive health. Dietary inadequacies in vitamin B12 and magnesium were strongly correlated with elevated systemic inflammatory markers. Meanwhile, insufficient intake of essential trace minerals like manganese and copper was directly linked to degraded cognitive outcomes. Ultimately, while preliminary, this pilot data strongly reinforces the premise that optimal brain aging, neuroprotection, and overall healthspan extension demand strict precision in both metabolic maintenance and micronutrient sufficiency.
Impact Evaluation The impact score of this journal is 1.4, evaluated against a typical high-end range of 0–15+ for top nutrition science, therefore this is a Low impact journal.
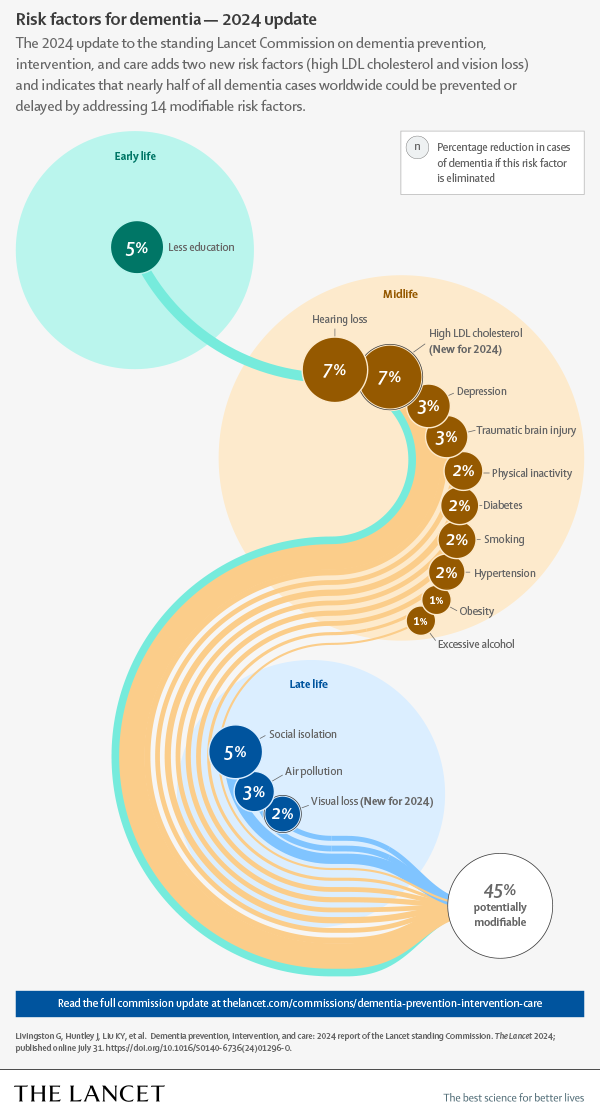
Yes, that’s because half of the dementia risk factors are preventable, and we’ve been better at addressing high cholesterol, hypertension, diabetes, etc.
For the remaining half, though, we have no clue, so we’ll reach a ceiling…
Albayram stressed that the findings should not be taken as a blanket warning against fish oil use. “I am not saying fish oil is good or bad in some universal way,” he said. “What our data highlight is that biology is context-dependent. We need to understand how these supplements behave in the body over time, rather than assuming the same effect applies to everyone.”
He hopes the research encourages closer examination of both the benefits and limits of omega-3 supplements. The study focused on a specific condition, repeated mild traumatic brain injury, and used CTE tissue to provide supporting evidence rather than to prove direct cause.
“As with any study, there are important boundaries,” Albayram said. “In the human CTE tissue, we can observe patterns, but we cannot prove what drove them. We also cannot capture every variable that shapes omega-3 handling in real life, including overall diet, health status, and lifestyle.”
The next step, according to the team, is to better understand how EPA is absorbed, transported, and distributed in the body, especially through fatty acid transport systems. “This paper is a starting point,” Albayram said, “but it is an important one. It opens a new conversation about precision nutrition in neuroscience, and it gives the field a framework to ask better, more testable questions.”
Highlights from the paper itself:
EPA exposure after TBI unmasks a latent cerebrovascular vulnerability
EPA reprograms endothelial metabolism, impairing vascular repair and remodeling
EPA-driven neurovascular instability promotes tauopathy and cognitive decline
Findings reveal metabolic context as key to omega-3 effects in brain injury
Symptoms of early dementia reversed by bespoke treatment plans
People with cognitive decline or early-stage dementia saw their symptoms improve when given bespoke treatment plans that targeted their personal nutritional deficiencies, ongoing infections and environmental exposures
A personalised programme that combines targeted medical interventions with lifestyle changes seems to improve memory and functioning among people with mild cognitive decline or the early stages of dementia. This involves assessing someone for factors that could be affecting their cognition – such as mould exposure, infections or hormonal deficiencies – and creating a bespoke plan to target them.
Dementia is an umbrella term for several conditions that affect memory, thinking and the ability to perform daily activities. It has no cure, with treatment generally focusing on relieving symptoms. But for Alzheimer’s disease – which makes up about 60 to 70 per cent of dementia cases – some drugs, like lecanemab, can clear the sticky protein plaques that form in the brain and are thought to contribute to the condition.
However, many have argued that these don’t improve people’s symptoms in a meaningful way. This may be due to the complexity of Alzheimer’s and other forms of dementia, which, evidence increasingly suggests, involve age-related changes in the brain as well as genetic, health and lifestyle factors. “[Patients] didn’t get well because we weren’t treating what was causing it in the first place,” says Kat Toups at Bay Area Wellness, a private practice in Walnut Creek, California.
Now, she and her colleagues have investigated the potential of bespoke treatment plans. “The approach is: let’s find all the things that are hurting the brain [and] get rid of those,” says Toup. “Then let’s put back in whatever the brain and the whole body is needing as far as nutrients and hormones, and then let’s do things for neuroplasticity to help regain your brain.”
The team recruited 73 people – aged 65, on average – with mild cognitive impairment or early-stage dementia. “Some of them met [the] criteria for Alzheimer’s and others for MCI [mild cognitive impairment],” says Toups.
They all underwent testing to identify potential contributors to their symptoms. Alongside blood tests to look for biomarkers of Alzheimer’s, the researchers assessed their levels of inflammation and checked whether they had any underlying infections or hormonal, nutritional or microbial-related deficiencies. Using this information, the researchers created personalised treatment plans for 50 of the participants, such as addressing nutritional deficiencies via supplements.
They were also told to adopt a plant-rich diet, do aerobic and strength training six days a week, and complete daily cognitive training via games that targeted their memory, attention and visual-processing speed. This group was also given tips to optimise sleep and manage stress.
The remaining 23 participants continued with their usual treatment and lifestyle habits.
After nine months, those in the personalised group saw their overall cognitive score – assessed by CNS Vital Signs, a standard computer-based cognitive test – improve by 13.7 points, compared with a decline of 4.5 points in the standard-care group. Improvements were also seen across specific domains within the test, including memory (up by 10.6 points versus a decline of 2.7), executive function (up by 9.8 versus down by 2.2) and processing speed (up by 6.9 versus down by 1). “Over 90 per cent of the patients in the precision-medicine approach had statistically significant improvements,” says Toups.
I do wonder what the corresponding known 0% was in 1984 though. And what the corresponding % will be in 5 years time.
I would argue that we do have “clues” as to the remaining half. This from Gemini suggests we’ll be at 65% modifiable in 10 years. With AGI ot could be much higher
“Factors Expanding the Prevention Percentage
The “preventable” percentage is rising because researchers are identifying more environmental and biological triggers that we can control:
2017 (35%): Identified 9 factors including hearing loss, hypertension, and obesity.
2020 (40%): Added 3 factors: air pollution, excessive alcohol, and head injury.
2024 (45%): Added high LDL cholesterol and vision loss.
Future Projections (Up to 65%): Emerging frameworks now include “structural” factors like poverty, wealth shocks, income inequality, and HIV infection rates.”
Is there any evidence of a ceiling? The trendline suggests that there’s no slowing of our improving ability to avoid/delay dementia. And all other things being equal AI should accelerate prevention
Association between vaccinations and risk of dementia: a systematic review and meta-analysis
Conclusions and relevance
Adult vaccinations, particularly against herpes zoster, influenza, pneumococcus and Tdap, are associated with a lower risk of dementia. Vaccination strategies should be incorporated into public health initiatives for dementia prevention.
There’s nothing in what you copied that suggests that. At most, we can conclude that we add about 1% per year, so in 10 years we could be ~55%. But that’s highly speculative. If you read the Lancet report, they also list some areas that might be modifiable independent risk factors but are not yet confirmed (I think sleep is one of them, for instance). Even if you add those, I’m not sure we’ll go above 60%. And in any case, those interventions are already done by many people so at the population level we might not see more benefits.
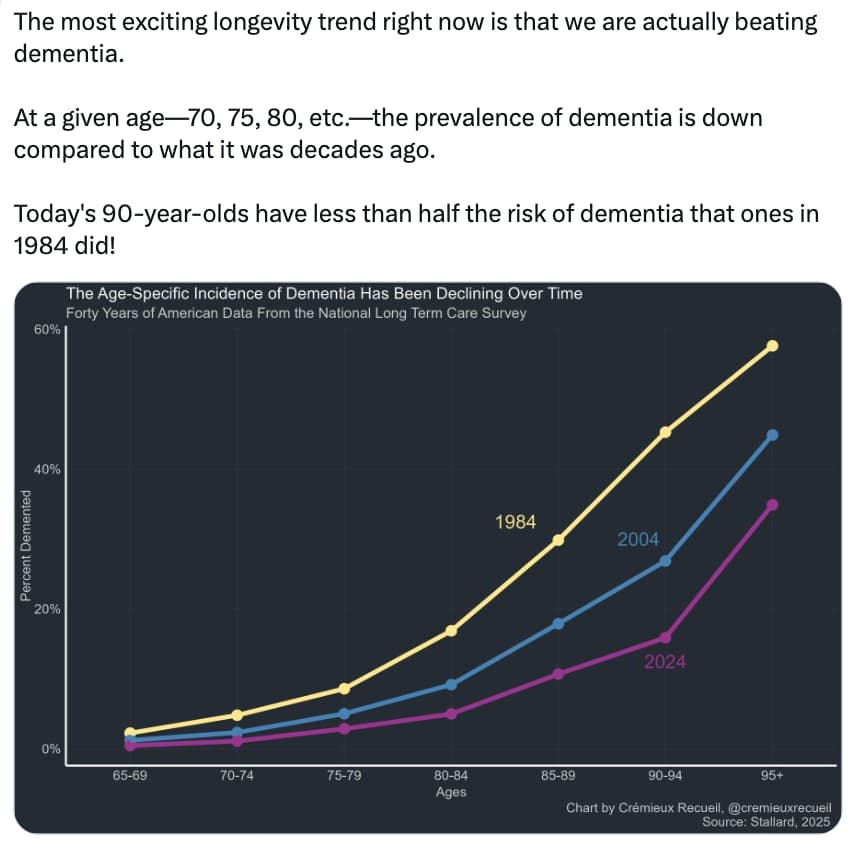
The progress in the 20y from 1984 to 2004 is more than from 2004 to 2024. So most likely 2024 to 2044 will be even less. This is a general rule that the last mile is the hardest to achieve.
A conceptual problem in classifying risk factors goes to derivation of cause. If, for example (only an illustration) a genetic variant determines or increases the probability of decreased folate assimilation, classifying it as a genetic cause with the implication or assertion that it is not modifiable is incorrect. In this example the intervention is simple and effective and the contribution to a causal chain is eliminated. Some genetic variants present as currently unmodifiable effects but many do not. Lp(a) was in that category until recently.
The brain’s cleaning system can be boosted to rid Alzheimer’s proteins
A duo of drugs that boosts our glymphatic system, which clears waste from our brain, also improves the removal of proteins associated with the onset of Alzheimer’s disease
Our brain removes metabolic waste via the glymphatic system, a network of channels surrounding the blood vessels that pump waste fluid to the lymphatic system, where it is carried to the blood for disposal.
The glymphatic system is most active during deeper phases of sleep, when slow brain waves help push along waste fluid after it has been released from brain cells. But it becomes impaired with age, and especially during Alzheimer’s disease.
To explore dexmedetomidine’s effects in people, Paul Dagum at pharmaceutical company Applied Cognition in Redwood City, California, and his colleagues recruited 19 adults – aged 60, on average – who were deprived of sleep for one night in a lab. The morning after, the participants – who had no chronic medical conditions or brain-specific issues – provided blood samples to act as baseline measurements.
They were then given 4 hours while they received an infusion of dexmedetomidine. They also took a drug called midodrine, which treats low blood pressure, a common side effect of dexmedetomidine. When they woke, the participants provided another blood sample.
A few weeks later, the researchers repeated the experiment, but this time, the participants had a placebo pill and saline infusions. The researchers then compared the two post-nap blood samples, accounting for variations in the two baseline samples.
This revealed that taking dexmedetomidine and midodrine, which the company collectively calls ACX-02, cleared two amyloid and tau proteins that are particularly prone to misfolding and forming clumps more effectively than the placebo/saline intervention.
The team estimates that if ACX-02’s effect were sustained over several years, it could delay the onset or worsening of Alzheimer’s disease by about seven years, based on levels of misfolded amyloid that are typically seen in people who go on to develop the condition, says Dagum. “That would be a significant, meaningful effect for those at risk,” adds team member Jeff Iliff at the University of Washington in Seattle.
Gu accepts that previous efforts to clear misfolded amyloid-beta and tau from the brains of people with Alzheimer’s disease have had limited benefits. Nevertheless, he adds that if the new approach is safe and effective, it could have a wide use. “It could benefit people with other brain conditions caused by a build-up of misfolded proteins, such as Parkinson’s,” he says. It might even be possible to develop a pill form of dexmedetomidine to treat attention lapses following sleep deprivation, says Iliff.
I didn’t interpret the chart’s trend as having much predictive power, because it only has three temporal data points. And the trendlines are so different depending on which age you look at
But i can see that extrapolation is tempting…
Estimating at the raw data, and looking at say , “% with dementia aged 90to94” - this falls from 45% in 1984 to 25% in 2004 and 15% in 2024. Extrapolating could suggest 10% in 2044, 7.5% in 2064 etc ultimately plateauing to only 5%.
But that’s relying quite a bit on a very limited trendline. And the historic deceleration may have a lot more to do with public health issues (accelerating processed food consumption, or inactivity or social isolation or inequality etc) than anything that should be applied to the modifiability of an individual’s risk
I would argue that accelerating progress in medicine and healthcare from AGI amd also the the increasing capital for research and development and the fact that we have so many “clues” as to where to investigate next will mean that we wont see this deceleration in practice…
As an example, ive just put my genome into claude.ai and it has generated reams of advice on bespoke preventative measures for preserving cognitive health. Most i was doing anyway, but several are novel and with decent logic behind them. For example my PEMT allele status means i dont effectively produce
phosphatidylcholine (along with a third if the population) - taking citicholine more regularly should have a marked impact on my dementia risk. Yet this would not be in the radar of either the general population or a typical doctor.
Decoding the Fifteen-Year Countdown to Brain Decay
The Pre-Diagnostic Map: How Your Medical History Predicts the Velocity of Neurodegeneration
Neurodegenerative diseases like Alzheimer’s and Parkinson’s are traditionally viewed through a categorical lens—binary states of “healthy” or “diagnosed.” A landmark study by Lian and colleagues, analyzed here by Nedelec and Corvol, shatters this simplistic model. By applying transformer-based AI to the electronic health records (EHR) of over 100,000 patients, researchers have mapped a complex, 15-year “prodromal” period where the seeds of brain decay are visible long before the first tremor or memory lapse appears.
The investigation identifies five distinct subtypes for both Alzheimer’s and Parkinson’s, characterized by unique clinical trajectories and comorbidity burdens. The “Big Idea” is a fundamental shift in perspective: neurodegeneration does not happen in isolation. Instead, it is the culmination of a decade-plus of systemic failures in metabolic, vascular, and psychiatric health.
Perhaps most striking is the discovery of “convergent phenotypes”. Patients with metabolic-inflammatory profiles—marked by obesity, diabetes, and renal disease—follow nearly identical, aggressive paths toward disability regardless of whether their primary diagnosis is Alzheimer’s or Parkinson’s. This suggests that while genetics might load the gun by determining disease susceptibility, systemic factors like insulin resistance and neuroinflammation pull the trigger on the rate of progression.
The study also reveals a counterintuitive “dissociation” between genetic risk and clinical severity. Some individuals with high polygenic risk scores follow a “classic” slow-burn trajectory, while those with lower genetic risk but high metabolic dysfunction suffer rapid, high-mortality outcomes. This underscores a critical reality for the longevity community: your “genetic destiny” is a poor predictor of how fast you will decline if your metabolic health is compromised.
Actionable Insights
Aggressive Metabolic Management: The “Metabolic-inflammatory” subtype (Cluster 4) across both diseases exhibits the most aggressive clinical decline and highest mortality. Managing biomarkers associated with diabetes, obesity, and renal health is not just for heart health; it is the primary lever for slowing neurodegenerative velocity. [Confidence: High]
The 15-Year Window: Prodromal signals—including depression, hearing loss, sleep disturbances, and constipation—precede motor and cognitive symptoms by up to 15 years. Treating these “unrelated” comorbidities early may alter the eventual disease trajectory. [Confidence: Medium]
Modifiable Risk Supremacy: Up to 45% of dementia cases may be attributable to modifiable risk factors. Interventions targeting insulin signaling and systemic inflammation (e.g., GLP-1 agonists, SGLT2 inhibitors, or senolytics) could potentially benefit patients across different diagnostic categories by stabilizing the “progression environment” of the brain. [Confidence: Medium]
Institution: Sorbonne University, Paris Brain Institute (ICM).
Country: France.
Journal: Nature Aging.
Impact Evaluation: The impact score of this journal is 16.6 (JIF 2023/2024), evaluated against a typical high-end range of 0–60+ for top general science, therefore this is a High impact journal.
The Silent Signal: Mapping 20 Years of the Hearing-Dementia Connection
For decades, the medical community treated hearing loss (HL) and Alzheimer’s disease (AD) as distinct consequences of the aging process—one a matter of sensory degradation, the other a catastrophic cognitive collapse. However, a comprehensive 20-year retrospective analysis published in Ageing Research Reviews (2025) confirms that these two conditions are biologically and mechanistically entwined. Analyzing 349 core studies from 2004 to 2024, researchers have mapped a “closed-loop” relationship where auditory decline not only signals early neurodegeneration but actively accelerates it.
The study identifies a critical distinction between peripheral hearing loss (PHL) —stemming from the ear’s hardware—and central hearing loss (CHL) , which involves the brain’s processing centers. PHL acts as a “gateway” to cognitive decline primarily through sensory deprivation; when the brain is starved of auditory input, it undergoes structural atrophy due to disuse and increased social isolation. Conversely, CHL shares a direct molecular “handshake” with Alzheimer’s, characterized by synaptic degeneration and neuroinflammation in the same regions responsible for memory, such as the hippocampus.
Bioinformatic mapping revealed 2,747 shared genes between the two conditions. These genes cluster around three primary axes: the PI3K-Akt signaling pathway (critical for neuronal survival), the AGE-RAGE axis (a driver of inflammation), and canonical Alzheimer’s pathways. The research suggests that hearing impairment, particularly central auditory dysfunction, may serve as one of the earliest detectable biomarkers for AD, often appearing before clinical memory loss. As global populations age, this meta-analysis underscores that hearing health is not a secondary quality-of-life issue but a frontline defense in the fight against dementia.
Actionable Insights
Prioritize Subtype Diagnosis: Distinguish between ear-level (peripheral) and brain-level (central) hearing issues. Central auditory processing deficits are more indicative of direct neurodegenerative risk.
Hearing as a Modifiable Risk Factor: Treat hearing loss as a primary, modifiable risk factor for dementia. Early intervention with hearing aids or cochlear implants may mitigate the “sensory deprivation” pathway that leads to cortical atrophy.
Targeted Screening: Integrate auditory assessments into standard neurological exams for adults over 65, as hearing thresholds are strong prognostic indicators of future cognitive decline.
Molecular Synergy: Consider that compounds supporting the PI3K-Akt pathway (e.g., certain neuroprotectives) may simultaneously benefit both auditory longevity and cognitive resilience.
Institution: Department of Otolaryngology, Head and Neck Surgery, The First Affiliated Hospital of Anhui Medical University.
Country: China.
Journal Name:Ageing Research Reviews.
Impact Evaluation: The impact score (CiteScore 2023) of this journal is 25.7, evaluated against a typical high-end range of 0–60+ for top general science, therefore this is an Elite impact journal.
Yes, i was mainly highlighting it as an example of where we have “clues” as to other factors we can fix. But there is some evidence beyond the mechanics:
A note on using claude.ai with your genome. About half the recommendations were overstated and didn’t stand up to scrutiny. Getting claude to check its own work is a quick fix