Here’s my latest episode…this time with Dr Austin Baraki who argues that blood testing is an important but challenging area of medicine. He argues that people should not put too much faith in imprecise technology measuring indirect markers of biological function. False precision can lead to over confidence, and distract people from the lifestyle improvements that would really make a difference. And he also shares his tips on reducing the variability and error in your own blood test results.
I hope you find this helpful. And be sure to check out this interactive website (and paper behind a firewall; who can get this?)
Another great episode, @Joseph_Lavelle. It strikes me that a lot of us in this community are using blood tests the way we want a diagnostic to be able to operate, but the tests we have, and the knowledge we have about the biology behind the tests, are not always at the point of supporting the use we are putting them to.
A good podcast. One thing I did not notice being mentioned on the podcast, however, was that some biomarkers metabolise in the sample so the delay in doing the testing really matters.
When I do my blood tests I record the time the blood was drawn. That helps in terms of working out where the daily cycle may be.
The amount of data I have enables spotting trends more than someone with say 6 monthly blood tests where many changes fall within a mixture of test accuracy and biological changes.
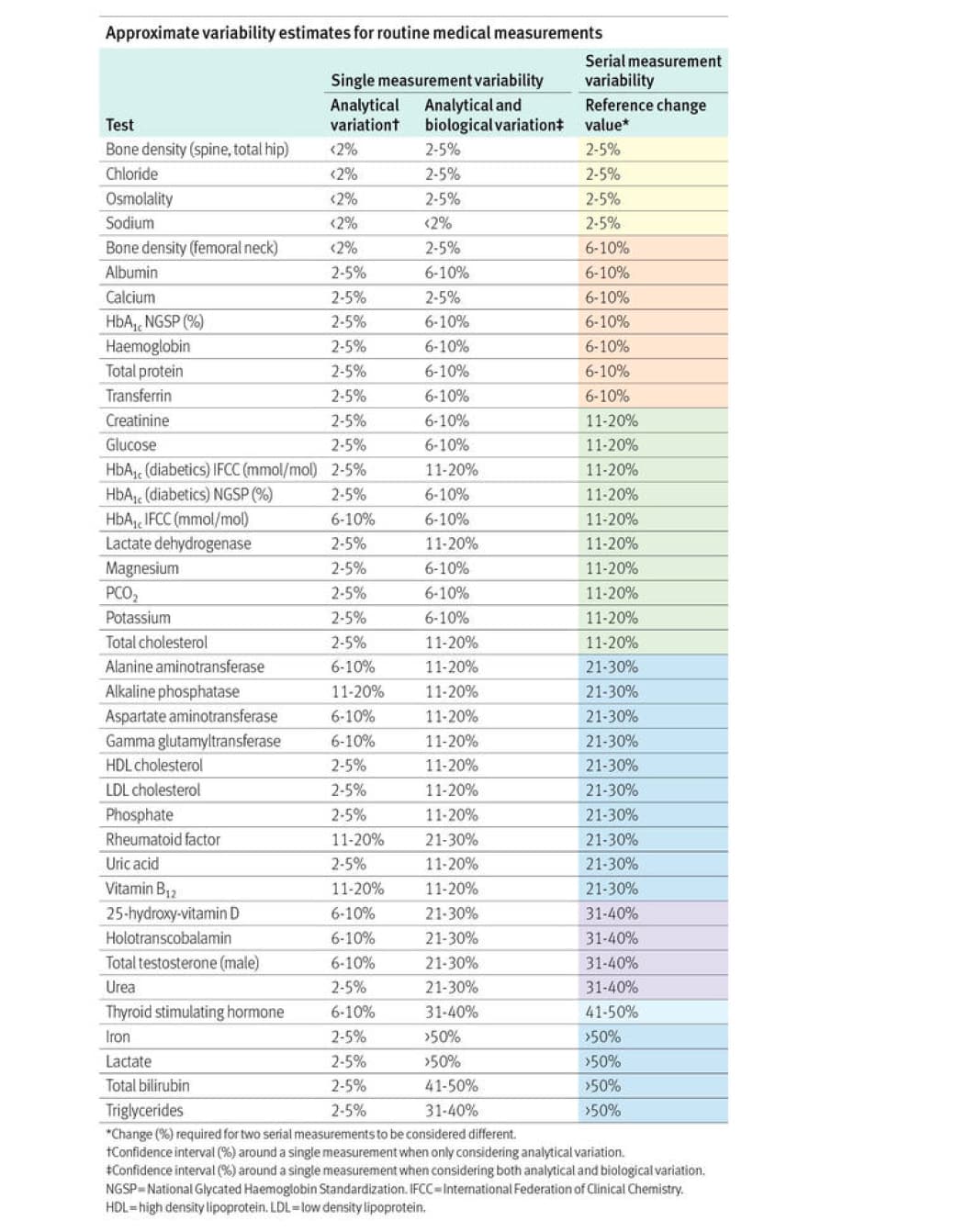
Thanks. This is the key chart, I agree. But even items on the low variability end of the range can vary a lot. Dr Baraki mentioned high albumin as a classic indicator of dehydration, and hemoglobin can look crazy high, which is consistent with my own experience when dehydrated (by not drinking fluids for 12+ hours without exercise or sweating).
Thanks, @Barnabas. I really didn’t like the answer so I kept fighting back but in the end I knew he was right. I will still get blood tests. I just will no longer use them like Google Maps step by step directions towards health.
In particular I will keep looking for the outlier result that means something has gone badly wrong (or at least might have).
The really fine tuning might be quixotic, but I actually think Dr. Bakari raised a lot of points that are already known to people in this community, like exercise impacting AST and ALT or cystatin-C being better than creatinine for assessing kidney function in muscular people. I think with all the various metabolomics research happening we’ll see more ability to do sophisticated screening and get the kind of deeper insights we are hoping for. In the meantime, staying in range on the big ones is still a reasonable goal.
I think the main learning is how much variability exists in the test data from testing error (inconsistent time of day, hydration, delays in processing blood, etc) AND the nature of what is being tested is often an indirect measure of what we are trying to assess.
These problems can be overcome with enough care and a large volume of test results, but our personal data of full of issues. Don’t make confident conclusions based on the test numbers alone.
This fits with Dr Batakis advice to focus on the big levers of health vs making rifle shot attempts to tweak one or more blood test results over time.
I enjoyed this episode and think it provides some practical guidance.
Most people (e.g. not on this forum) undertest both in frequency and scope of testing.
Patients I get from routine primary care have labs once a year, with a CBC, Comp, maybe lipids … and that is about it.
People on this forum are more likely to at least average labs every 3 months, I’d guess.
The biggest issue is contextualization of how to interpret, and also what variances and abnormalities to ignore.
The next issue is being aware a lot of the tests people get quarterly add nothing … and if testing is done more frequently, it should generally be targeted to limited labs that might be at risk of change, or are under therapy (e.g. insulin resistance, ApoB)
IMO: It adds to the statistical evaluation of how we are doing by giving us enough data points to get a statistical average, which may be meaningful.
The cost for the test for me is small. My doctor prescribes the tests every six months because of my age, and I buy my own tests twice a year from Utla Labs.
Whether it is meaningless or not, I cannot say as I do not have the expertise, but it gives me a warm fuzzy feeling to evaluate more frequent data points.
Michael Lustgarten, PhD certainly thinks more data is better and tests much more frequently than I do.
I just got my quarterly last week and got a surprise! My Alkaline Phosphatase was 64. It’s always been 95 or so. I think this is a good thing, it means my microbial burden is smaller for some reason. The only things I can think of:
I’ve been taking 1000mg lactoferrin since chelation because my ferritin dropped to 75. Since taking it, the ferritin it has rebounded to 95. Close to perfect for me. Lactoferrin helps.
I’ve been taking exogenous ketone salts regularly. BHB kills bacteria, and helps also.
I do 3 doses of 33mg doxycycline around when I do oral DMSA every 2 weeks. Doubt that does anything, but it is a possibility since the timing is right.
So the blood tests are useful and it gives me something to think about.
@desertshores I’ve been thinking more about Lustgarten’s health optimization measurements and practices that have led him to lowering his bf% to 10% with a CR diet largely comprising strawberries and sardines (approximately true I think). I appreciate his contributions to us all but he now seems trapped in this continuous optimization effort. I hope he gets rich and famous for his “all in” investment. I wonder how much normal variation in blood test results are confounding his calculations…