This is what is used to market Tesamorelin and if you don’t know that Tesamorelin does NOT reduce visceral fat, you might buy into the hype.
But… but… the clinical trials using Tesa showed a reduction in visceral fat in HIV patients. True but what is the mechanism of how that fat is reduced?
Tesa is a peptide that stimulates the pituitary gland to produce hGH, hGH is what reduces visceral fat, NOT Tesa.
It does not matter how you increase your hGH, Ipamorelin and many other peptides do increase hGH as well as using HRT with Somatropin to replace the hGH.
I’ve puzzled over the Ipa vs Tesa thing for a while now and have come to a couple conclusions.
half-life matters
dose matters
timing matters
The half life of Tesa and Ipa are pretty much the same 1 to 2hrs with Ipa seeming to be closer to 2hrs
Tesa is clinically dosed at 1.0 to 2.0mg
Ipa - internet dose is consider to be 250mcg to 400mcg (the dose i"ve been using for 2.5 years)
Timing, both just before bed time
The dose of Ipa seems way too low as I’ve been comparing what is known about both these peptides so I’ve increased my dose to 1.0mg of Ipa + 250mcg of CJC 1295 noDAC
I’ve asked Perplexity about monotherapy, Tesa alone compared to Ipa alone compared to Ipa in combination with CJC 1295 noDAC, and it looks like combination therapy will provide a bigger hGH boost.
The more one searches and reads what is available in reputable journals, the more you learn.
While there is not the same level of clinical evidence for Ipa re: visceral fat, it has been clinically proven to increase hGH, but not a lot of info on the doses used.
And that is what has spurred me to increase my dose of Ipa to Tesa level dosing.
The study by González-Sales et al. (2015) successfully created a mathematical model that predicts GH and IGF-1 levels in both HIV and healthy populations. The model confirms that the drug’s effect is consistent across health states and changes dynamically over 14 days of treatment.
• Population Consistency: The study statistically proves that HIV infection does not alter the fundamental pharmacodynamic parameters of the drug. The pituitary and liver respond to Tesamorelin with the same capacity and sensitivity in HIV-infected patients as in healthy volunteers.
• Sequential Non-Linearity: The study establishes a sequential link (Tesamorelin \to GH \to IGF-1) that is best described by a power model (exponent 0.35). This confirms that IGF-1 response is not directly proportional to GH changes, but follows a non-linear curve. (Note: The study makes no claims regarding this mechanism’s role in safety).
• Signal Amplification (Day 14 Effect): The most significant finding is the dynamic change in pituitary response over time. On Day 14, the pituitary released GH at a rate (S_{max}) more than double that of Day 1, and required lower concentrations (EC_{50}) to do so. The authors conclude that daily dosing “amplifies the intensity” of the signal transduction cascade.
• Feedback Activation: The study observed that the duration of the GH pulse (T_{GH}) shortened significantly by Day 14 (0.8h \to 0.28h). The authors hypothesize this is due to the amplified signal triggering a faster and stronger negative feedback loop to maintain homeostasis.
You are partially correct, when used as monotherapy, ipamorelin dosage has to be in the mg range, not mcg.
But when used with a ghrh like tesamorelin, you can get away with mcg doses for ipamorelin. This is because studies have shown that the synergy of a ghrh and ghrp enable you to release more growth hormone than using either one separately. Use your favorite Ai to find links to studies in the synergy of ghrh and ghrp, for example, here is one here : https://academic.oup.com/jcem/article-abstract/89/5/2290/2844515?redirectedFrom=fulltext
In summary, in healthy elderly women and men: 1) acute synergy of GHRP-2 and GHRH is greater in the female; 2) 24-h combined GHRP-2 and GHRH drive is more effective than either agonist alone; and 3) 30-d stimulation with GHRP-2 sustains a physiologically activated somatotropic axis.
I was not reading carefully enough, so I’ll modify my Ipa + CJC combo to relect this and drop the IPA back to 400mcg and increase the CJC from what I started with, 250mcg, up to 500mcg to see how that goes.
One of the studies referenced has some interesting information
Conclusion
The development of GHRH agonists focused on enhancing GH release, improving metabolic functions, and promoting tissue repair. MR-409 demonstrated therapeutic potential across various conditions, from cardioprotection to neuroprotection. The development of GHRH antagonists, particularly those in the MIA and AVR series, has provided new opportunities for cancer therapy and the treatment of other diseases. These antagonists have shown efficacy in antitumor and anti-inflammatory activities with minimal adverse effects, positioning them as favorable alternatives to conventional chemotherapeutic agents. MIA-602 and AVR-352 offer promising clinical applications for human cancers, inflammation-related diseases, and neurodegenerative disorders. The ongoing research and development of GHRH agonists and antagonists continue to highlight their potential as versatile therapeutic agents across a wide range of medical conditions.
Here is all my “research” that got started with the visceral fat thing. What hGH does is very interesting
That particular article is not very helpful. So I will keep looking.
> Based on the study information, here are the peptide doses used:
Acute IV Bolus Injections:
GHRH: 1 µg/kg
GHRP-2: 0.1 µg/kg OR 1.0 µg/kg (two different doses tested)
Combined: GHRP-2 (0.1 µg/kg) + GHRH (1.0 µg/kg)
Single SC injection: GHRP-2 (10 µg/kg)
24-Hour Subcutaneous Infusions:
GHRP-2: 1 µg/kg·h
GHRH: 1, 3, or 10 µg/kg·h (three different doses tested)
Combined: GHRP-2 (1 µg/kg·h) + GHRH at one of the three doses
30-Day Continuous Subcutaneous Infusion:
GHRP-2: 1 µg/kg·h (delivered via portable Panomat pump, with site inspection and reservoir replenishment every 3-4 days)
Regarding the increase with combination therapy vs monotherapy:
From the study results:
The 24-hour infusion of GHRP-2/GHRH (1/10) stimulated significantly more GH secretion than either GHRP-2 alone (P = 0.021) or GHRH alone (P = 0.012), though the exact fold-increase is not specified in the abstract
The combination “drove GH secretion more than GHRH alone” (P ≤ 0.024) when GHRP-2 (1) was combined with GHRH (3 or 10) in men and GHRH (10) in women
The abstract confirms synergy exists but doesn’t quantify the exact magnitude of increase for combination vs monotherapy during the infusion studies. To get precise fold-change or percentage data, you would need access to the full-text results tables and figures.
Look for a paper called: “History to the discovery of Grehlin”, full text available on scihub. It does a great job of summarizing GHRH/GHRP results.
IV bolus
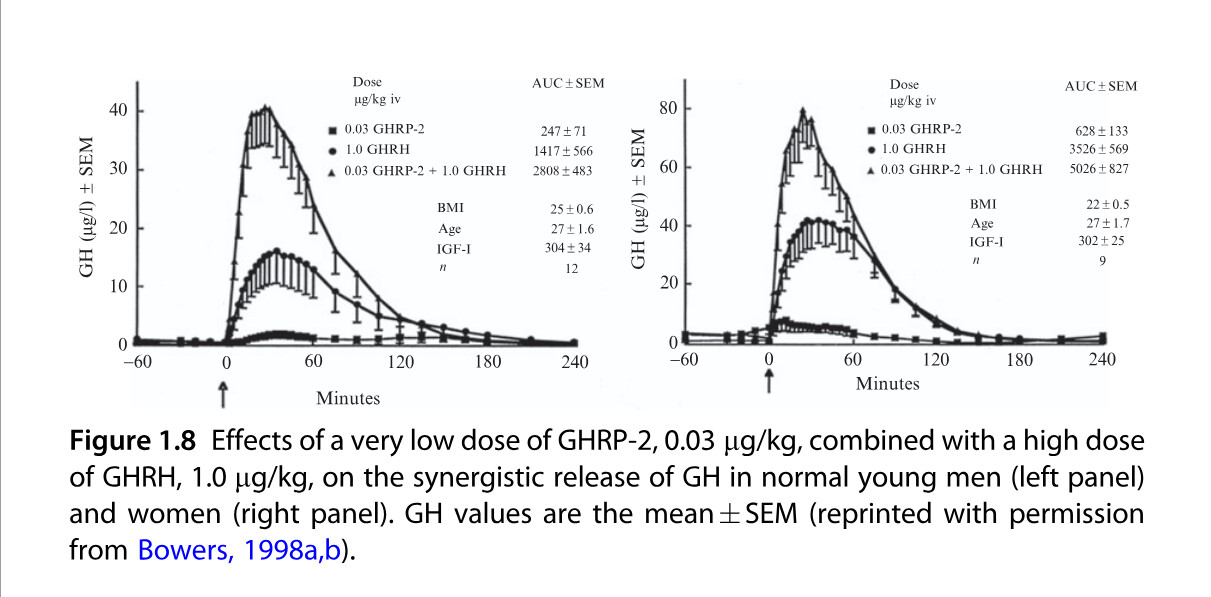
Results in Fig. 1.8 of normal young men (left panel) and women (right
panel) demonstrate that iv bolus combined GHRP-2 and GHRH at the
respective doses of 1 mg/kg GHRH and a subthreshold GH-releasing dose
of 0.03 mg/kg GHRP-2 released GH synergistically (Bowers, 1998). From
these studies, GHRP is envisioned to act on the hypothalamus to release an
unknown factor (U factor) rather than endogenous GHRH which subsequently acts concomitantly with GHRH on the pituitary somatotroph
to release GH synergistically. In this study, the important specific finding is
that GHRP-2 augments GHRH release even when GHRH is present
in excess amounts, and the concomitant GHRP-2 dose of 0.03 mg/kg is a
subthreshold GH-releasing amount. Thus, GHRP þ GHRH is not releasing
GH in this study by augmenting endogenous GHRH release and, further-
more, GHRPþGHRH release in vitro is additive and not synergistic
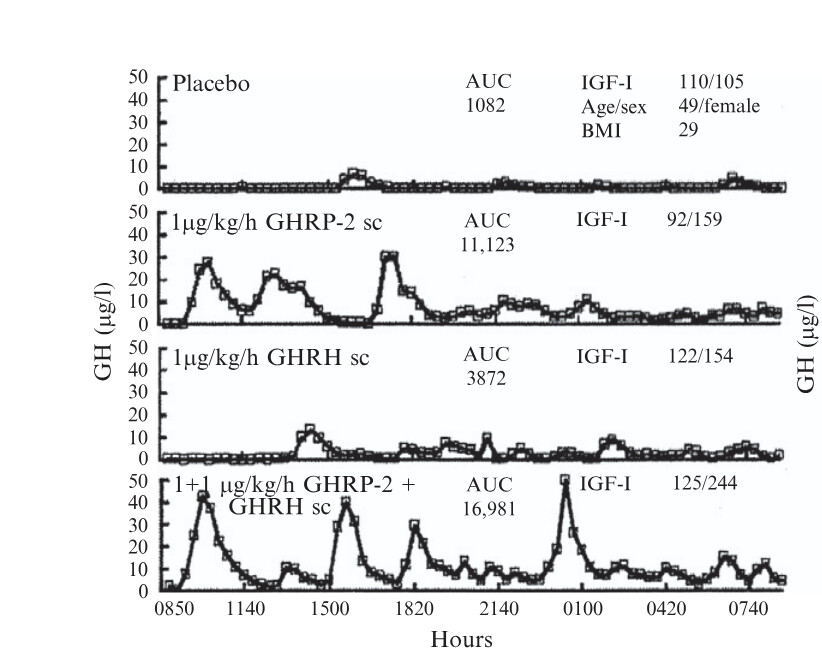
Twenty-four-hour continuous subcutaneous infusion of GHRP-2 (left panel) produced the same effect as ghrelin infusion at 1 mg/kg/h. When GHRP-2 or ghrelin was infused with GHRH, the pulsatile GH secretion pattern was the same but the amplitude of the GH pulses was further increased. IGF-I levels rose by about the same to both peptides
Since I don’t know anyone who is doing 24 hour SubQ infusions or IV bolus some of this data is not completely relevant. Basically infusions are going to induce a bigger, much longer response than a single nightly SubQ injection.
And I don’t see any single SubQ dosing, only single IV Bolus, which is one shot and in a more effective way, i.e. Intravenous, IV dosing is going to provide a more immediate and higher peak response.
One part of the study indicates these 2 doses,
For me (64kg) that would mean 64mg per dose, I’m using 0.75mg (750 mcg)
I see this is referred to as a “subthreshold” GH-release amount" and does increase hGH in this combination. For me (64kg) that would be 2mg, I’m using 0.4mg (400mcg)
From this information my doses are significantly lower than used in part of this study.
In another part of the study they use a much lower dose of GHRP (I’m using Ipamorelin) of 0.03mcg x 64 = 2.0mcg, much lower than my 400mcg dose.
Also these doses responses are in young men and women. I’m neither
Since I’m a 70 y/o guy who’s natural hGH production is going to be very low, there is limited info on what dose should be used.
An update on this. I’m on to my third bottle. I’m really loving this product. I don’t see myself going without it. Combined with lowering my caffeine intake, this has given me a sense of inner peace like nothing else. I feel like I’m able to tackle most situations without any stress where other people seem to get mad and lose their shit.
Does there happen to be any biochemist on board… ? I would be extremely grateful for some insight into the structural and functional implications of a cysteine-to-alanine substitution in a peptide (as described in a patent) that eliminates a disulfide bond. I’m particularly interested in how this modification might affect folding and stability, and whether it could significantly impact its biological activity.
I don’t really consider myself a biochemist but alanine substitutions are generally a stratagy to put a relatively inert filler aa in the place of one that you think has significance in the peptide or protein’s activity/stability. Cysteine Cysteine disulfide bonds are a biological solution to hold a protein in its 3-D structure. So molecular biologists often perform alanine substitutions to knock out a stabilizing bond between two loops of a peptide or protein. This could be used as a blind mutagenesis strategy where every cysteine in a region was substituted for an alanine and then proteins were screened for properties of increased or decreased structural sensitivity by looking for temperature-sensitive (either cold or hot) mutations. These were valuable tools because the activity of a protein could be modulated by say growing yeast carrying the mutated proteins at a couple of degrees warmer or colder than usual and then controlling the experiment with growth where the protein was stable.
In the case of peptides these bonds might be critical for the peptide activity since peptides lack multiple long secondary structures (beta barrels and alpha helices) that also contribute to the folding and stability and I would think substituting a known peptide disulfide bond with an alanine would have a huge effect on the stability of a peptide, likely destabilizing it and making it inert.
If you were looking for the affect of an alanine substitution in a specific peptide sequence to predict a change in protein folding then I’d agree with John that computer modeling of protein/peptide structure would be the way to investigate it.
Why not opt for Ibutamoren? Grehlin receptor agonist, orally bioavailable, proven by FDA trials to raise endogenous HGH almost as much as the jab (noninferior). And one less thing to inject, with all the risks of that.
Wrong, Ibutamoren is not approved by the FDA, because of concerns of congestive heart failures, and excessive edema. Iparemorelin, another ghrelin agonist seems to have comparatively less side effects and is more selective regarding cortisol and prolactin elevation. Iparorelin is also not FDA approved.
Did you end up trying this? I’m thinking of getting BPC157 capsules to see if it can improve gut health. Sometimes I get indigestion and stuff and know when this happens I feel some autoimmune conditions get a bit worse so there might be a connection there.
Who has tried it and does anyone know a good affordable source of BPC157 capsules?
Floxed - a serious untreatable condition brought on by an allergic reaction to the ciprofloxacin antibiotic (and it’s 'floxacin relatives) .
Cipro is a black label antibiotic due to the severity of an allergic reaction with this one. This means it’s an antibiotic of last resort. Incredibly useful in most cases. Problem is, you don’t know who is allergic until it happens. Then it’s too late.
Our daughter was “floxed” about 8 years a ago and has suffered extreme neuropathic pain from her calves to her toes, it varies in severity but has never gone away until now. She has other symptoms but this one was the most prevalent for her.
We tried a number of things over the years and nothing would touch it.
She was visiting us this weekend and commented that the neuropathic pain is now gone. She noticed that about 2 weeks ago. Funny how when things get better it can sneak up on us and quickly become the new “normal” It took her a few days to recognize this was not a transient improvement. That it seems to be “permanent” but time will tell.
What may have done this?
She has been taking a number of peptides over the years with no effect on this.
8 months ago she started on ARA 290 - 4mg per day, 5 days a week. Not an overnight change but she “thought” she was experiencing fewer high level incidents.
3 months ago we added SS 31 as being floxed does affect the mitochondria.
We are not sure which of these 2 or if it’s the combination has finally given her some relief but we are all pretty excited for her to finally be pain free after 8 years.
The severity of this condition for some is extreme, ruptured tendons, relentless pain, living in a wheel chair, etc. There are over 100,000 cases of this in the US so probably 10,000 in Canada, not to mention the rest of the world.