Brandy, a trough of 1.9 ng/mL isn’t zero, but it’s below any published therapeutic range I’ve been able to find. And 68 ng/mL may not be all that high for a peak, as charts on the grapefruit juice boost, posted elsewhere in the forum, show much higher ng/mL levels for 16 mg plus grapefruit.
Assuming a 66 hour half-life, 14 days, or 5.09 half-lives, would bring the 68 ng/mL down to 2.03. 1.9 is pretty close. That tends to validate 66 hours as the half-life, at least in my case. Would another 66 or 132 hours, getting down to 1 or 0.5 ng/mL, be useful? I don’t know.
I did eat just one grapefruit with the dose last Friday, instead of the three I ate before the peak blood test. Since I’m not having any problems at the current 12 pill dosage, I don’t expect to change that. I’ll have to think about lengthening the time between doses, but I’m kind of inclined to stay at two weeks.
Argonaut, sounds like your approach is reasonable. Have you noticed any changes in your laboratory parameters while on rapamycin? Labs I would consider tracking while on rapamycin are your HOMA-IR (insulin sensitivity), daily glucose levels (preferably checking fasting and post-prandial excursions), CBC (mainly to watch out for anemia), iron/ferritin levels, testosterone levels (watching for decrease from your pre-rapamycin baseline), lipid levels, and white blood cells (esp. lymphocytes).
Might also be helpful to track your PhenoAge using the Phenotypic Age calculator available for download here:
Brandy, thanks for the suggestions and the link to the spreadsheet. I’ll check my phenotypic age when I get the blood tests from my yearly checkup in a few months. Meanwhile, I’ve been remiss in getting blood tests and probably have a too-casual approach to all this.
I got the peak sirolimus test to check the pills. They came from from India and without any noticeable side effects or benefits, I questioned whether they were real. After finding out that they were, testing the trough seemed a good idea. That’s been the limit of my tracking so far.
You and the others on the forum, who obviously know far more than I do about medicine and biology, have been a welcome resource and I appreciate the information and insights.
Argonaut:
Thank you for sharing your test results.
Your test results are very useful information to those of us on this journey into uncharted territory
May I ask which brand of pills you purchase from India?
Also, which lab you are using?
Desertshores, I bought the pills from Pravin Lahoti at Varun Medicals in India. The cost last July, including shipping, was about $1.13 per mg for 1mg Zydus brand pills. I wanted to pay with PayPal, but he didn’t accept that. I had to wire the money to his bank. It has been a while, so that could have changed. The package of 83 strips of 6 pills took about a month to get here, with tracking showing lengthy stops at customs in Mumbai and New Jersey. The return address said Varun Medicals and the box didn’t appear to have been opened.
From bits of information gleaned here and there, I decided on Zydus over other slightly less expensive Indian brands. One of the assays I had seen elsewhere is also posted on this forum.
The lab I used was Quest Diagnostics, purchased through Ulta Labs. The total cost, including the blood draw fee of $8, was $108, this after a 20% discount given when I set up the appointment via phone. It doesn’t appear that you would get the discount by setting it up through the Ulta website, but I don’t know for sure.
Thank you that’s good to know.
I have been using Wise, formerly TransferWise to transfer from my bank to Indian banks.
They have been quick, cheap, and flawless. https://wise.com/
Pravin may take that. He does use all the Indiamart payment methods. I was stuck on PayPal because I had experience with it and didn’t know how secure some of the others might be. So I just wired the money.
Argo, great to hear your report. Amazingly coincidentally, I just took delivery of my first Indian order of rapa from Pravin and had a similar experience except I received mine in about three weeks. I had been taking 6 mg per day since last August and over the last month I have bumped it up 1 mg per week and this morning I took a 10 mg dose and plan to maintain that level for a while. My plan was to take 6 mg of $4 American pills and supplement them with the Indian product but may transition to the Zydus brand since your blood tests indicates that it is obviously legit. Thanks for posting; this was great affirmation of my plan. Other readers, take note of this Very reasonably priced rapa resource….it’s so weird to wire money to an unknown bank account but it worked out very well and I intend to use Pravin exclusively in the future.
Methuselah, I had called a couple of companies that test drugs and their prices were very high. They aren’t meant for individuals. When someone in this forum mentioned doing a blood test, I wondered why I hadn’t thought of it. Someone else posted the name of the lab that I then used for the test. This is a great site. Thanks, RapAdmin.
I’ve been reflecting some more on this topic of dosing.
MK is using 0.15mg/kg/wk in the current TRIAD trial and is presumably, based on the pilot study, confident of a benefit at that dosage. The literature shows that the conversion from dogs to humans is 0.541 so:
0.15 x 0.541 = 0.08115mg/kg
This equates to 6mg/wk for a 74kg individual which is (as a %) significantly less than the 8 to 10mg/kg I’ve been taking to date and interestingly identical to Peter Attia’s stated dose.
I’m still yet to hear a strong rationale for going above 0.1mg/kg OR a compelling argument for the use of GFJ (beyond cost)?
I’m gaining a strong conviction that more is not better here and indeed now plan to take a 4 week ‘vacation’ before restarting at 6mg.
Possible, though unproved or speculative, reasons might include:
if you start rapa late in life, higher dosage might clean up more damage (autophagy, etc)
many experts (MK?) have said that we are guessing on dosage–this is the first large dog trial and there are no large human trials
absorption and half-life are known to vary widely from one individual to another
rapa might cross the BBB more readily at higher dosages
biweekly dosing might make inhibition of mTORC2 less likely, as there is a longer tail with lower concentration
Any more? I realize these are not strong rationales, but I think the only strong ones for 6mg/wk is a safety margin and a (recent) tradition in the community.
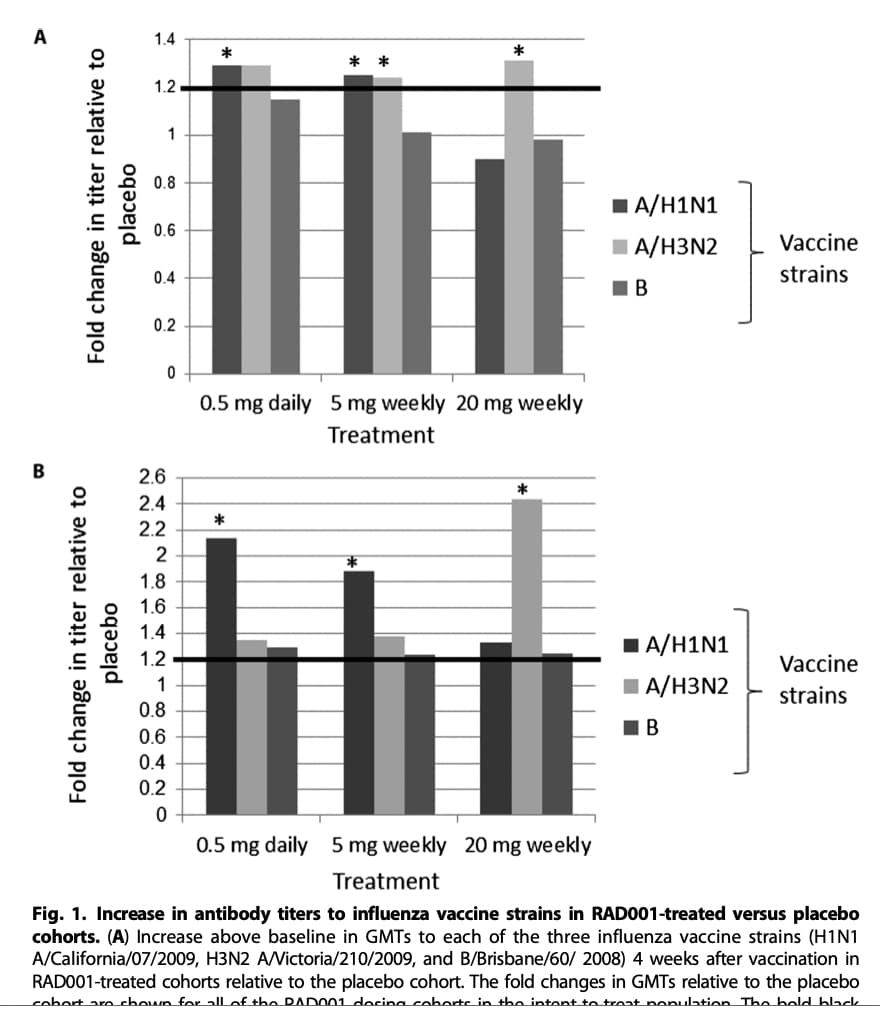
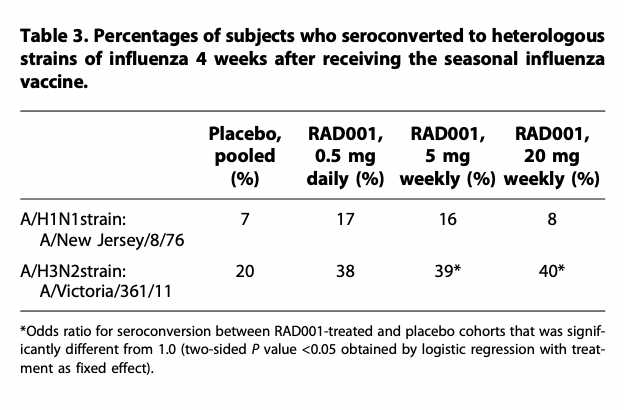
We have peer reviewed data that shows 20mg/wk of Everolimus had a negative impact on immune response. We also know that 20mg everolimus is approximately equal to 16mg of Rapamune.
That gives a small range of effective dose since somewhere between 4 and 16mg Rapamune (5 and 20 of Everolimus) the balance shifts negatively (at least for immune response).
It seems the data are a little less clear on that and that the response is flu strain dependent, don’t you think? What data point did you see as most compelling to support your statement that 20mg / week is clearly negative?
The other issue may be that perhaps immune system response may not be the best proxy for measuring lifespan extension. It may just be the easiest to measure.
I’m leaning in the 6 mg/ week direction especially after reading that low dose rapamycin prevented atherosclerosis by inducing only a moderate degree of autophagy. Higher doses gave no increase in effect and may be associated with greater side effects.
Impossible to estimate optimal human doses for longevity based on studies in mice. Mice studies have their limitations. Even human studies on various drugs will look good in phase 1&2 trials just to fail in phase 3. And that’s in humans.
Maybe the dog study will shed some additional light on this.
RapAdmin, if you get a chance to ask Matt Kaeberlein questions in an upcoming “ask me anything” session, it would be great to get his perspective on the following:
For longevity purposes, based on his knowledge of the literature, is the rapamycin peak blood concentration (Cmax) or Area Under the Curve (AUC) more important?
Prolonged mTORC1 inhibition eventually leads to mTORC2 inhibition. In humans, how long of a washout period is required to replenish mTORC2 to its normal (pre-rapamycin exposure) levels?
In a previous interview, Matt mentioned that he takes between 6 to 10 mg of sirolimus per week for 8 to10 weeks, then cycles off. For how long does he cycle off, and what is his rationale for cycling off?
If the Mannick study (which showed mTOR inhibition improves immune function in the elderly) is being used as the framework for rapamycin dosing, shouldn’t we be using biweekly dosing of sirolimus instead of weekly, given that the half-life of sirolimus is roughly double that of everolimus?