I need to read this when I have some time, but it all seems to report the consequences of a failing neuron being downstream of damage to Complexes 1 and 3.
I would need to read up on this to say anything of any use. I am too busy at the moment to do this.
Parkinson’s disease (PD) is a neurodegenerative disorder with both genetic and environmental factors contributing to pathogenesis. Viral infections are potential environmental triggers that influence PD pathology. Using ViroFind, an unbiased platform for whole virome sequencing, along with quantitative PCR (qPCR), we identified human pegivirus (HPgV) in 5 of 10 (50%) of PD brains, confirmed by IHC in 2 of 2 cases, suggesting an association with PD. All 14 age- and sex-matched controls were HPgV negative. HPgV-brain positive patients with PD showed increased neuropathology by Braak stage and Complexin-2 levels, while those positive in the blood had higher IGF-1 and lower pS65-ubiquitin, supporting disruption in metabolism or mitophagy in response to HPgV. RNA-Seq revealed altered immune signaling in HPgV-infected PD samples, including consistent suppression of IL-4 signaling in both the brain and blood. Longitudinal analysis of blood samples showed a genotype-dependent viral response, with HPgV titers correlating directly with IL-4 signaling in a LRRK2 genotype–dependent manner. YWHAB was a key hub gene in the LRRK2 genotypic response, which exhibited an altered relationship with immune-related factors, including NFKB1, ITPR2, and LRRK2 itself, in patients with PD who are positive for HPgV. These results suggest a role for HPgV in shaping PD pathology and highlight the complex interplay between viral infection, immunity, and neuropathogenesis.
Press: Groundbreaking study finds possible virus link to Parkinson’s Disease
His team discovered the presence of Human Pegivirus — a virus not previously linked to any known disease — in half of the Parkinson’s patients studied.
“This is a blood-borne virus that can be found in 5-to-10% of healthy blood donors. It’s related to hepatitis C — and we found it in 50% of brains of patients with Parkinson’s disease.”
Because the virus is similar to hepatitis C, researchers now plan to investigate whether existing hepatitis C medications might also help treat or even prevent Parkinson’s.
![]()
3 Likes
There is a correlation with a lot of chronic diseases and pathogens, especially with neurodegenerative disease.
This is why laboratory rodents live longer than wild, lack of predators (including pathogens).
This is why if humans were living an environment free of major pathogens and toxins (except for controlled bioflora) assuming good diet, exercise, sleep and lack of major stressors, they would live much longer IMO.
We already have evidence of that with hygiene, proper nutrition, clean water, vaccinations almost tripled the life span in the past 150 years… mainly by reducing premature deaths.
2 Likes
I performed a search of the site and did not see this study posted. If it had been, I apologize. I make a special effort to find French papers on PD. Obviously this is in women. Note however, again, it does matter which specific statin is used, here even a broad class effect of lipophilic vs hydrophilic. Rather counter to previous hypothesis, it’s the lipophilic that had a positive effect. Given how long symptomless period for PD can be prior to diagnosis, I wonder if 5 years is enough.
Statin Use and Incidence of Parkinson’s Disease in Women from the French E3N Cohort Study
Yes, lipophilic looks better in this paper but overall association studies are mixed:
High LDL is protective in PD (per MR), so this might just be reverse causation (high LDL => statin use & lower PD risk):
- Protective role of apolipoprotein A and B in Parkinson’s disease: A prospective study from UK Biobank 2025: “Elevated baseline levels of serum ApoA (HR = 0.84, 95 % CI: 0.71–0.99, P = 0.047) and ApoB (HR = 0.67, 95 % CI: 0.57–0.78, P = 3.18E-07) were associated with a reduced risk of incident PD.”
- Association of cholesterol and glycemic state biomarkers with phenotypic variation and Parkinson’s disease progression: The Oxford Discovery cohort 2025: “HDL-C and total cholesterol differed across baseline PD phenotype clusters, with reduced levels associated with the most severe motor and non-motor phenotypes (psychological well-being, cognitive impairment, REM sleep behavior disorder, and daytime sleepiness). Higher HDL-C and total cholesterol, although the latter was attenuated after adjustment for statin use, were associated with better baseline activities of daily living (e.g., UPDRS-II score with 1 SD increase in HDL-C −0.74, 95%CI −1.22 to −0.26, p = 0.002) and non-motor features. Neither predicted the rate of motor or non-motor progression.”
Two RCTs tried lipophilic statins in early PD:
- Simvastatin: worsening motor symptoms in the simvastatin-treated group.
- Lovastatin: no significant difference in motor scores but possible beneficial effect in terms of dopaminergic cell loss.
Confirmed by MR: Causal relationship between PCSK9 inhibitor and common neurodegenerative diseases: A drug target Mendelian randomization study 2024: “HMGCR inhibitors increased the risk of PD (OR [95%] = 1.907 [1.502 to 2.312], p = 0.001)”
Not PD but see also: Mendelian Randomization Study of PCSK9 and HMG-CoA Reductase Inhibition and Cognitive Function 2022: “Using a wide range of cognitive function and dementia endpoints, we failed to find genetic evidence of an adverse PCSK9-related impact, suggesting a neutral cognitive profile. In contrast, we observed adverse neurocognitive effects related to HMGCR inhibition, which may well be outweighed by the cardiovascular benefits of statin use, but nonetheless may warrant pharmacovigilance.”
Gut disruption of GLP-1 might be the mechanism of action: Cardiovascular Health - #993 by adssx
Association studies + MR + RCT + Mechanistic understanding all point towards statins (and lipid-lowering in general?) being bad in PD.
1 Like
Statins may facilitate Parkinson’s disease: Insight gained from a large, national claims database
As a Black Sabbath fan since I was 14, my very first 8 track was Paranoid, I was saddened when he passed yesterday. I knew he had been ill with Parkinson’s for a while but did not know there are so many version of this disease.
2 Likes
Chinese paper and toxin rodent models but…
Serving as a pivotal hub for cellular metabolism and intracellular signaling, the mitochondrion has emerged as a crucial organelle whose dysfunction is linked to many human diseases, including neurodegenerative disorders, particularly Parkinson’s disease (PD). However, whether mitochondrial quality control (MQC) can be targeted for therapeutic interventions remains uncertain. This study uses clinical samples, molecular biology techniques, pharmacological interventions, and genetic approaches to investigate the significance of NAD+ levels in cross-species models of PD. These results reveal that treatment of rotenone-incubated cells with NAD+ boosters (such as NMN, siCD38, and NAT) increases UPRmt/mitophagy-related MQC, reduces pro-inflammatory cytokine expression, inhibits apoptosis, and strengthen redox reactions. In vivo, NMN supplementation inhibits motor deficit and forestalls the neuropathological phenotypes of MPTP-induced PD mice, which are required for the atf4-related mitochondrial UPR pathway. Notably, bulk omics signatures and metabolomic profiling analyses of the striatum reveal NMN-induced transcriptional changes in genes and proteins involved in mitochondrial homeostasis. Thus, these findings demonstrate that the accelerated pathology in PD models is probably mediated by impaired MQC and that bolstering cellular NAD+ levels alleviates mitochondrial proteotoxic stress and mitigate PD phenotypes.
With a focus on citrate @John_Hemming:
One prevailing strategy for estimating mitochondrial content is to measure the levels of citrate synthase (CS), a common marker of mitochondrial capacity, to normalize a given bioenergetic readout.
Notably, the activity of the CS protein was lower in the rotenone-treated cells than in the vehicle-treated cells, but it significantly increased after treatment with NMN, siCD38, and NAT (Figure 1l–o), indicating that the mitochondrial content was enhanced in the context of NAD+ boosters’ augmentation.
We then visualized the metabolites involved in regulating these pathways in a circos plot and found that citrate regulates multiple metabolic pathways, whereas prolyl, tryptophan, and adenine are involved in multiple sphingolipid pathways (Figure 10f). By combining the MSEA and pathway enrichment results, we preliminarily identified citrate as the key metabolite induced by NMN in the TCA cycle.
Consistent with our previous report, the mice treated with MPTP showed a robust CS decline in the striatum by immunofluorescence and western blot analysis, which was significantly offset by NMN treatment
1 Like
Without reading the paper I don’t think CS is at the core of the issue. The quoted text is not clear on whether it is the quantity of CS or the activity of CS that they are looking at. The activity will be linked with pyruvate influx.
Mechanical Forces Guide Axon Growth through the Nigrostriatal Pathway in an Organotypic Model
https://advanced.onlinelibrary.wiley.com/doi/10.1002/advs.202500400
“Reconstructing the nigrostriatal pathway is one of the major challenges in cell replacement therapies for Parkinson’s disease due to the lack of enabling technologies capable of guiding the reinnervation of dopaminergic precursors transplanted into the substantia nigra toward the striatum. This paper examines nano-pulling, as a technology to enable the remote manipulation of axonal growth.”
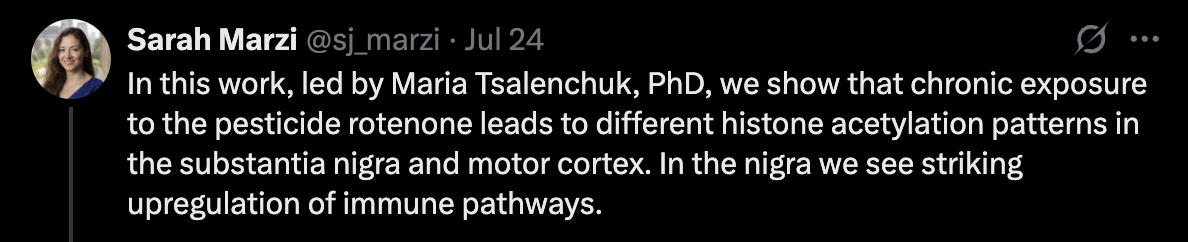
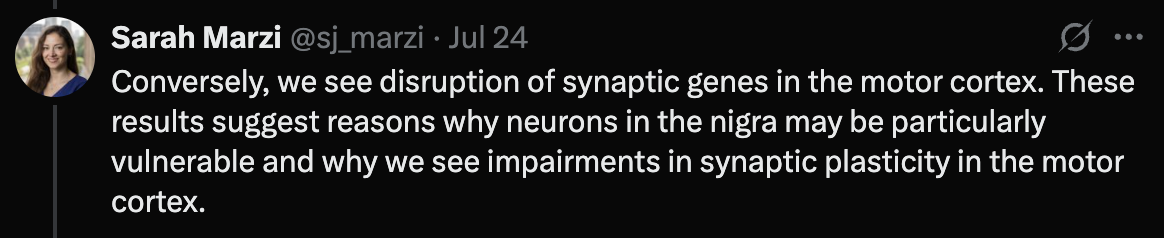
Pesticide exposure is increasingly recognized as a potential environmental factor in idiopathic Parkinson’s disease, though the molecular mechanisms remain unclear. This study explores how pesticide exposure alters gene regulation in key brain regions using the rotenone rat model. We performed H3K27ac ChIP-sequencing to profile active regulatory elements in the substantia nigra and motor cortex. Despite uniform complex I inhibition across regions, we observed region-specific epigenomic changes associated with rotenone exposure. RNA-sequencing confirmed transcriptomic alterations. We identified a strong, rotenone-induced immune response in the substantia nigra, including increased activity in the C1q complement pathway, suggesting immune involvement driven by regulatory mechanisms. In contrast, the cortex showed dysregulation of synaptic function at the gene regulatory level. Our results highlight a role for gene regulatory mechanisms potentially mediating the effects of pesticide exposure, driving region-specific functional responses in the brain that may contribute to the pathology and selective vulnerability that characterise Parkinson’s disease.
Pesticide exposure in rats changes epigenetic signatures in different brain regions (poke @John_Hemming).
1 Like
It hits the higher energy neurons first
UA and PD:
2 Likes
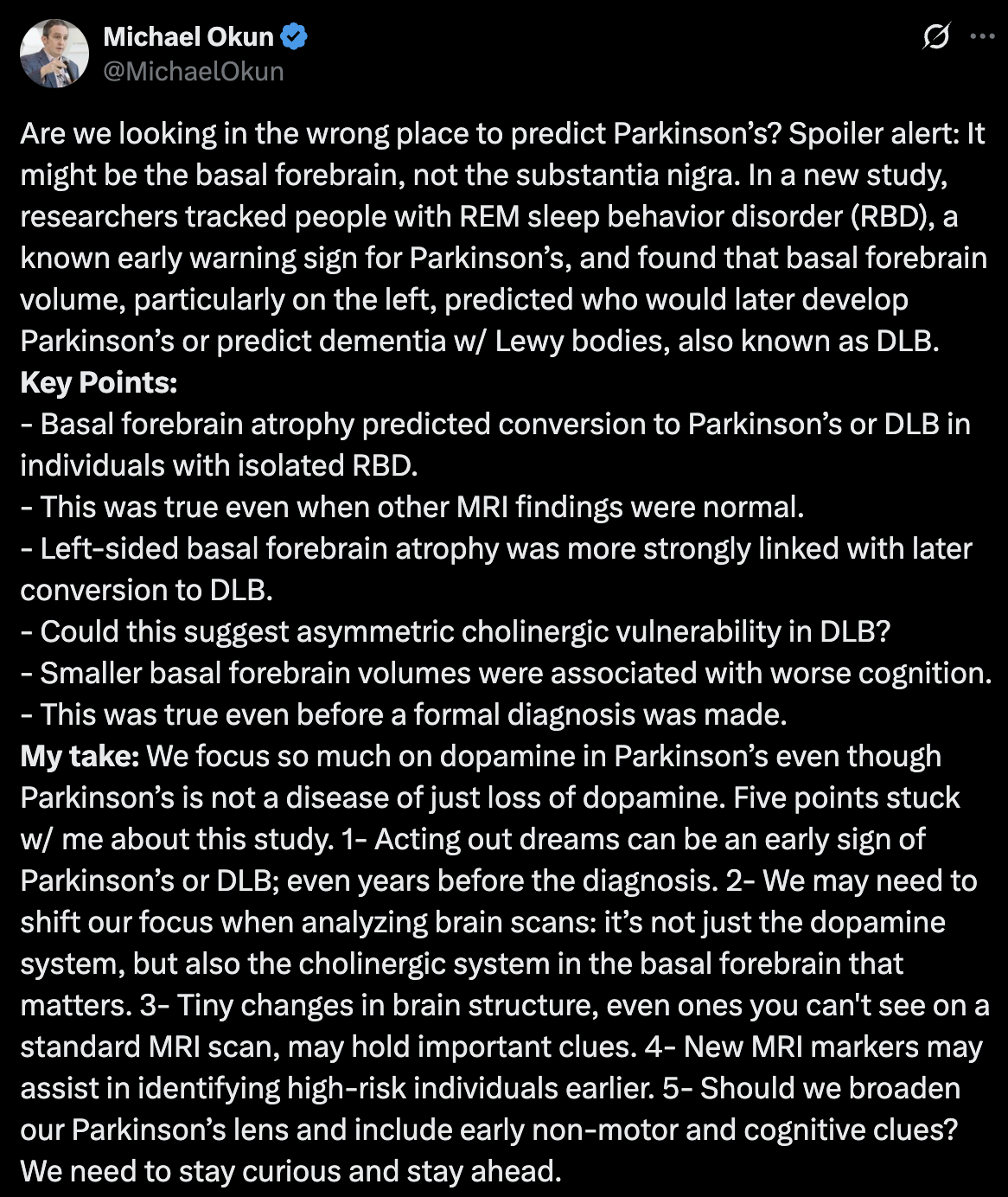
Basal Forebrain Volume Predicts Disease Conversion in Prodromal Synucleinopathy 2025
Thanks for sharing @John_Hemming
If rapa increases caudate and hippocampus volume, could it increase basal forebrain volume as well? Rapamycin as a preventive intervention for Alzheimer’s disease in APOE4 carriers: targeting brain metabolic and vascular restoration - #12 by adssx
5 Likes
One more datapoint in favor of our future Nobel prize @John_Hemming: Mitochondrial dysfunction-mediated metabolic remodeling of TCA cycle promotes Parkinson’s disease through inhibition of H3K4me3 demethylation 2025
(that being said, unfortunately it’s a group of weak Chinese universities + one Italian researcher)
Parkinson’s disease (PD), a neurodegenerative disorder caused by complex factors, is usually associated to mitochondrial dysfunctions but the links between such disorder and PD remain object of research. Here, we report that impaired mitochondrial quality control (MQC) system is a molecular basis of the mitochondrial dysfunction in PD and that tricarboxylic acid cycle (TCA cycle) disorder is the main feature of such mitochondrial dysfunction. Multi-omics analysis revealed that MDH2, OGDHL and IDH3G enzymes are bottlenecks in the enzymatic reactions of the TCA cycle in PD. Mechanistically, the abnormal α-KG/fumarate ratio caused by the TCA cycle bottleneck inhibits histone H3K4me3 demethylation and further enhances the expression of alpha-synuclein (SNCA), which may promote PD at an early stage. On these bases, we proposed a number of PD therapeutic strategies targeting mitochondria and histone methylation modifications, which proved to be effective in in vitro or in vivo models, especially citrate supplementation, in restoring normal TCA cycle enzymatic reactions. Taken together, our work highlights the non-negligible regulatory role of “mitochondrial-nuclear” communication in PD and provides important insights for the development of PD therapeutic strategies.
Citrate exhibits neuroprotective effects by correcting the abnormal α-KG/Fumarate ratio in PD
Based on the above results, we sought to find a natural supplement to correct the abnormal TCA cycle in PD. Given the extraordinary potential of citrate supplementation in improving cognitive ability, we constructed a subacute PD mouse model using MPTP and supplemented citrate through drinking water (Fig. 6A), which maximally simulated the dietary intake of natural supplements under physiological conditions [21]. Although continuous intraperitoneal injection of MPTP during model construction affected the food intake of mice, and this effect was reflected in changes in mouse body weight, the weight difference became no longer significant in the later stages of the model construction (Fig. 6B, C). During the establishment of the model, the water intake of mice was not affected, which ensured the stability of citrate supplementation (Fig. 6D). As expected, dietary citrate supplementation did not show systemic toxicity, while significantly increasing serum and midbrain citrate levels, confirming the safety and effectiveness of the citrate supplementation model, especially that citrate can cross the blood-brain barrier (BBB) and enter the midbrain (Fig. 6E, F). To evaluate the effect of citrate on motor dysfunction in the subacute PD model, we tested the motor ability and coordination ability of the model mice by behavioral tests. Compared with MPTP-treated mice, citrate supplementation reduced the time mice spent on the pole and increased the grasping time of mice on the inverted grid (Fig. 6G, H), indicating that citrate supplementation alleviated motor impairment in PD mice. Importantly, citrate supplementation restored the impaired tyrosine hydroxylase (TH; DaN marker) protein expression in the SN of PD mice and reduced MPTP-induced SNCA accumulation in the midbrain (Fig. 6I–K).
Currently, about the TCA cycle, supplementation of multiple metabolites including isocitrate [36] and α-KG [37] has been reported to show neuroprotective effects in PD. Based on the metabolic bottleneck of the TCA cycle reported here, we propose citrate as a potential metabolite for the treatment of PD. Actually, citrate can cross the BBB and shows good prospects in improving memory and treating Alzheimer’s disease [38,39,40]. At the same time, citrate, as α-KG precursor, acts as a metabolic supplement to help increase α-KG levels. More importantly, citrate can also act as a metabolic activator to enhance the activity of MDH2 in a high malate environment, promoting the conversion of fumarate metabolite malate to oxaloacetate [41], which reduces the accumulation of its substrate fumarate. Taken together, the multiple effects of citrate help reduce the α-KG/Fumarate ratio and correct abnormal TCA cycle flux, making it a very promising natural candidate for the treatment of PD. Previous reports have highlighted SNCA accumulation as an upstream event that triggers mitochondrial damage [42]. Here, our work emphasizes mitochondrial damage as an early factor in the pathogenesis of PD, and SNCA accumulation as a downstream molecular event that is finely regulated by α-KG/Fumarate ratio and H3K4me3 levels. These works reflect the complex crosstalk in the pathogenesis of PD and provide a more comprehensive perspective for the development of therapeutic strategies.
Briefly, mice (8 weeks old) received 12 days of daily drinking water containing citrate (Sigma; 1% w/v) and intraperitoneal injection (i. p.) of MPTP (MedChemExpress, HY-15608; 30 mg/kg body weight) or vehicle treatment for 8th to 12th days; the behavioral teste and sampling were performed three days after the last injection. Citrate was dissolved in drinking water, with pH adjusted to 7.3–7.4 by addition of sodium hydroxide.
They used the same dose as the paper Dietary citrate supplementation enhances longevity, metabolic health, and memory performance through promoting ketogenesis, which, according to ChatGPT, is equivalent to 8–10 g/day for a 70-kg human.
5 Likes
Thanks for this.
I take about 20g a day. I was this morning 82.2 kg.
Searching the paper there appears to be no mention of acetyl-CoA although there is a mention of acetylation. Hence I don’t think they have the mechanism right.
Still my citrate mix has now been mixed and is sitting in the factory to go to Amazon. I just need to sort out process.
5 Likes
Chinese preprint: Regulation of mitochondrial dynamics and function by MT1 melatonin receptor in Parkinson’s disease 2025
Here, we found the expressions of PINK1, and Parkin were decreased with MT1 deficits in vitro but not in vitro. The discrepancies between in vitro and in vivo models are probably because of the complex physiological conditions in the central nervous system, such as the interactions and signaling among neurons and glial cells. This effect is not similar to melatonin, which reported to be neuroprotective in PD by mitophagy augment [56]. Mitophagy is a selective autophagic removal process of damaged mitochondria. Since exacerbated LC3II/LC3I and P62 accumulation were observed in MT1 depleted PD mice, it is reasonable to speculate the autophagy of aggregates was also inhibited. Although we didn’t observe the TH loss in striatum and motor abnormality by MT1 knockout, the alteration of LC3II/LC3I ratio and P62 accumulation were found. This indicates the absence of MT1 may increase the susceptibility of PD occurrence through autophagy inhibition but is not the key etiological factor.
So melatonin “not the key etiological factor” @John_Hemming?
That’s the absence of a receptor not melatonin itself.
“Here, we found the expressions of PINK1, and Parkin were decreased with MT1 deficits in vitro but not in vitro.”
For the sake of clarity, this should be corrected, which is ‘in vivo’?
1 Like