I have Parkinson’s since December 2020. I do not take any medication! Since three weeks I take 5 mg rapamycin a week. I have published a video about my alternative healing methods:
")
I have Parkinson’s since December 2020. I do not take any medication! Since three weeks I take 5 mg rapamycin a week. I have published a video about my alternative healing methods:
Improving the mitochondria strikes me as a good thing to do to avoid Parkinsons (hence Rapamycin, but also other things for mitophagy).
Zone 2 exercise (as defined by Iñigo San Millán ) is important for mitochondria (improvement in density and amount of mitochondria) but it is unclear to me how it affects systemic mitochondria amount rather than local (exercised muscles, possibly nearby organs). Like the brain.
I understand it is possible for mitochondria to be transferred although I think rare hence autophagy/mitophagy has to be stimulated in the specific cells. There are lots of ways of doing this. Rapamycin is good in systemically doing this. Other stimulations of HIF 1 alpha such as a reduction in partial pressure of Oxygen mainly done through HBOT.
I am currently having a good go with Red Light and Near Infra Red, but that will only go part way into the skull possibly an inch or so.
I wonder how good PEMF is. I have paid for a Hugo Intense device, but not got it yet.
One thing to be careful about is glucose handling as high levels of glucose inhibit autophagy.
Please continue to update us on this. I have a friend recently diagnosed with this. I suspect that rapamycin has potential to greatly slow or stop parkinsons.
I haven’t dove in deep on the literature - but I suspect you may want to do larger pulsed dosing every two weeks to help increase the brain levels of rapamycin. See this thread here. Rapamycin and the Issue of Getting Through the Blood Brain Barrier
And: Blood Brain Barrier

Great video. I am very happy for you! What role do you think Rapamycin played in your sustained recovery?
I know you are doing a lot of alternative treatments. Which ones do you think helped the most?
Which of the alternative healing methods you use works best? (as of 07/29/2023)
That’s hard to answer. On my homepage www.parkinsonclub.de/about an overview diagram is shown, which shows the course of the disease in my case.
Here you can see that after the following applications: TPS Neurolit, PDCare from Symbyx Biome + the Vielight helmet there was a significant improvement in autumn 2021.
In this positive course I also had my first microbiome transfer, which I think is very important.
The 23 stays (April/May 2022) in the HBO (oxygen pressure chamber) had a very positive effect on my mood.
The stay in Cuba (since then I’ve been taking NeuroEpo regularly) from November 14th, 2022 to December 5th, 2022 had a positive effect on my sense of smell and on the swinging of my left arm. I know some Parkinson’s patients who have benefited greatly from this therapy.
I can’t tell you much about the SRT Zeptor, Iboga, Rapamycin, Broccoli Seed Teea and most recently my new HBO chamber and the Smovey rings.
I also do a lot of sports! Please refer sports | My Site (parkinsonclub.de)
Since my condition is very good, the therapies don’t have as much effect on me as they do on someone who has more symptoms.
My course is very good, basically the same since the strong improvement in autumn 2021.
My feeling tells me that I may be able to improve the symptoms a little and I think that I can maintain the level for a few years until there are further therapies.
Please look at my homepage www.parkinsonclub.de
If you could go back in time to the beginning of the diagnosis, what would you do?
I would immediately recommend all alternative healing methods that I believe to be successful, including sport & use nutritional supplements.
If your course worsens – what do you do then?
I would do a TPS refresher (6 times in two weeks), this should actually be done once a year. I hadn’t done this yet as my condition is very good and consistent. I would start taking Mucuna pruriens. Probably going to Cuba again. I would also start alternative therapies - see: what else I have in mind | My Site (parkinsonclub.de)
How much money have you invested so far?
It’s hard to say, fortunately my private health insurance company covered a lot. But I have the following monthly costs: dietary supplements around 350 euros (without rapamycin!), TPS around 500 euros (paid by my private health insurance company), naturopath pays my private health insurance company.
One-off costs: PDCare 1,350 euros, + helmet approx. 1,000 euros, HBOT - chamber for home 12,000 euros, 23 x HBOT in Heidelberg approx. 6,800 euros, 2 x microbiome transfer approx. 7,000 euros, Cuba approx. 15,000 euros (you get the medication for a longer period of time - you would have to go back after about a year - the drug should be available in Cuba at least in the foreseeable future), SRT Zeptor used at home 10,000 euros, infrared sauna about 3,000 euros.
This results in monthly costs of approx. 850 euros and one-time costs (without sports equipment) of approx. 58,000 euros. I think I spent at least 88,000 euros (including what I don’t list here, more like 100,000 euros) and got back about 25,000 euros from the health insurance company.
Which applications would you least want to do without if you didn’t have enough money?
PDCare + helmet, nutritional supplements (it doesn’t have to be the expensive products), sports! (Smovey, VR glasses for boxing and table tennis) then in the following order: TPS, microbiome transfer (only if necessary!), Cuba, HBOT – chamber for home, SRT Zeptor
Mayo Clinic just started a small trial of dapagliflozin and sitagliptin for PD and LBD: ClinicalTrials.gov I know that some researchers are interested in GMRx4 (metformin XR 350mg + dapagliflozin 2.5mg + sitagliptin 17.5mg) for PD as well. Wait and see…
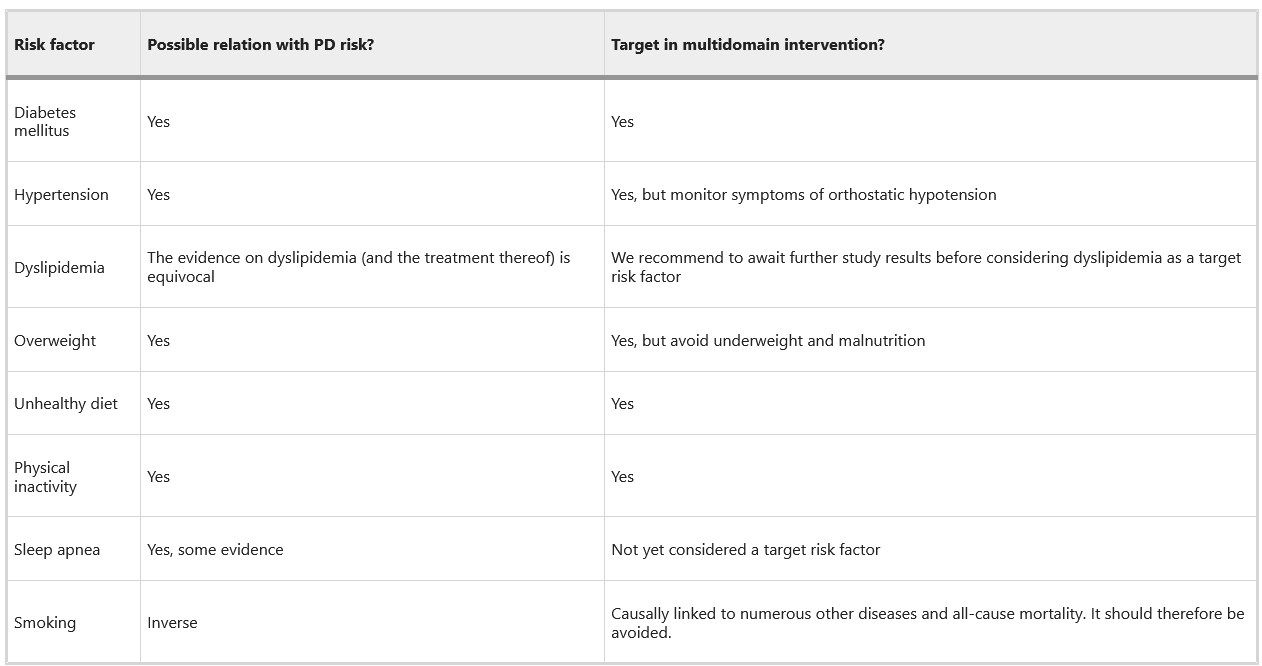
Tackling vascular risk factors as a possible disease modifying intervention in Parkinson’s disease 2024
As a neurologist treating many patients with Parkinson’s disease I have rarely encountered patients with the risk factors mentioned in the table. Many patients with idiopathic Parkinson’s disease are very healthy otherwise. Agree on smoking.
Yes, the table is not well done. For instance, obesity and diabetes mellitus protect against PD, but PD is associated with insulin resistance and use of some anti-diabetic drugs (e.g., GLP1RAs) lowers PD risk (and might slow down the progression).
A better way to represent the table would be that intensive glucose and BP management lowers PD risk.
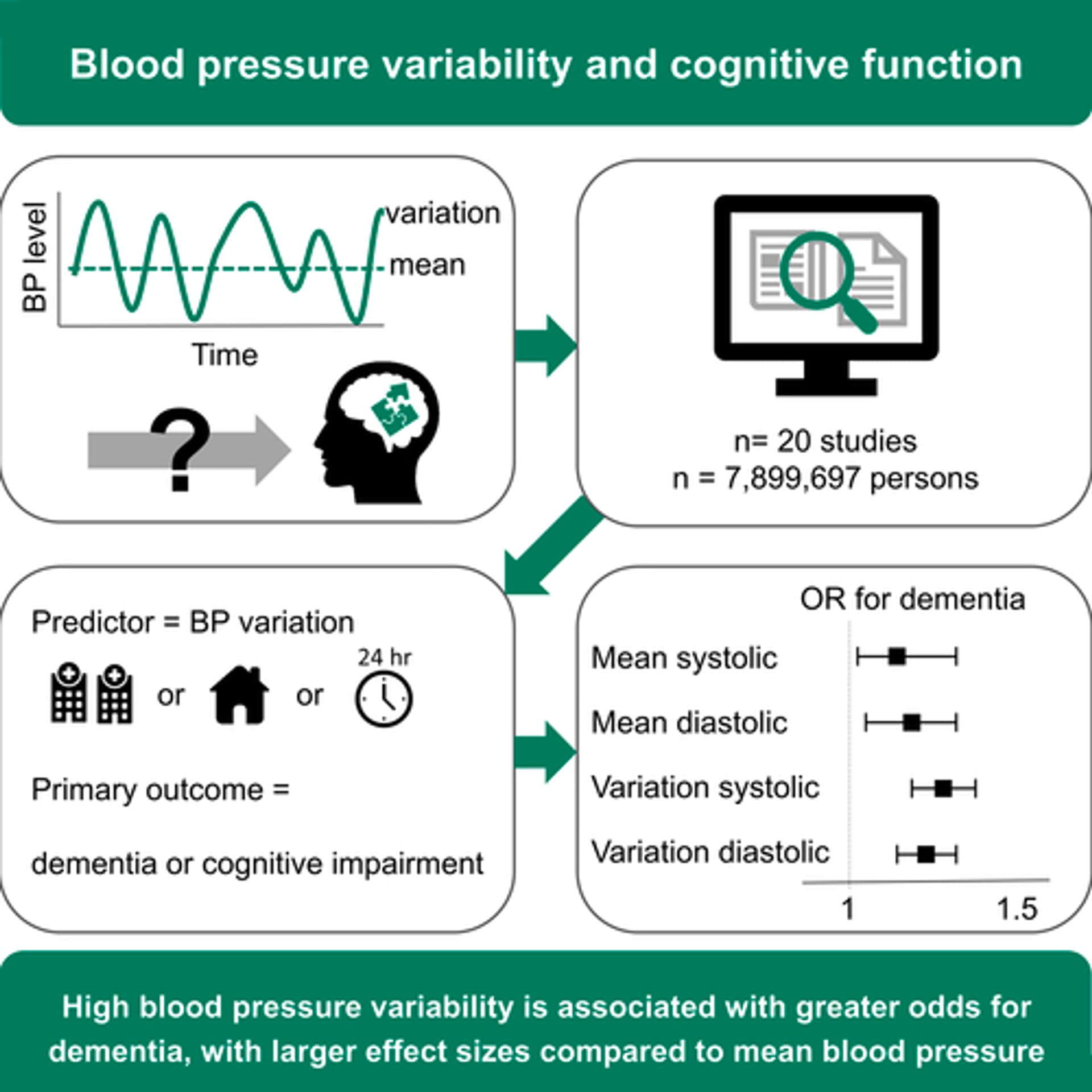
Also, “hypertension” is not the best way to look at things. Blood pressure variability matters more than the mean for NDDs:
And high DBP is protective, while high SBP is bad. So pulse pressure might be more important than mean SBP and mean DBP.
I remember a few papers in 2020-2022 discussing PD as likely a prion disease- with bacterial amyloid (curli peptides) from certain strains of bacteria(non butyrate producing) travelling up the vagus from the gut// and a variety of known causes of PD acting through this pathway. I always thought butyrate probiotics would be a nice helping hand( i think Pendulumm brands produce some). I also think there was some regression analysis on certain antibiotics that preferentially lowered butyrate producing bacteria (penicillins? or maybe macrolides?) I will go dig up the papers.
Thanks, would be interesting
“Dysbiosis in Parkinson’s disease might be triggered by certain antibiotics” Gabor Ternak et al, Journal:“Medical Hypothesis”
“Gut Microbiota: A novel therapeutic target for Parkinson’s Disease”, Manlian Zhu et al, Journal:“Frontiers in Immunology.”
Also the most interesting one was a little off topic but;
"Overwhelming Evidence for a major role for Herpes Simplex Virus Type 1 (HSV1) in Alzheimer’s disease: underwhelming evidence against. Ruth F. Itzhaki, Journal: “Vaccines”
the Alzheimer article has all sorts of interesting data on how different causes work through the HSV1 pathway-and even more tidbits on how things that prevent HSV1 seem to prevent Alzheimers. (pretty much any regular vaccination, in the elderly keeps their immune system stimulated enough to prevent an HSV1 flareup) there were other things like populations that took as little as 2 weeks of antivirals for herpes had a much lower alzheimer rate…
Sorry to careen off topic…not even close to a Rapa topic…oops
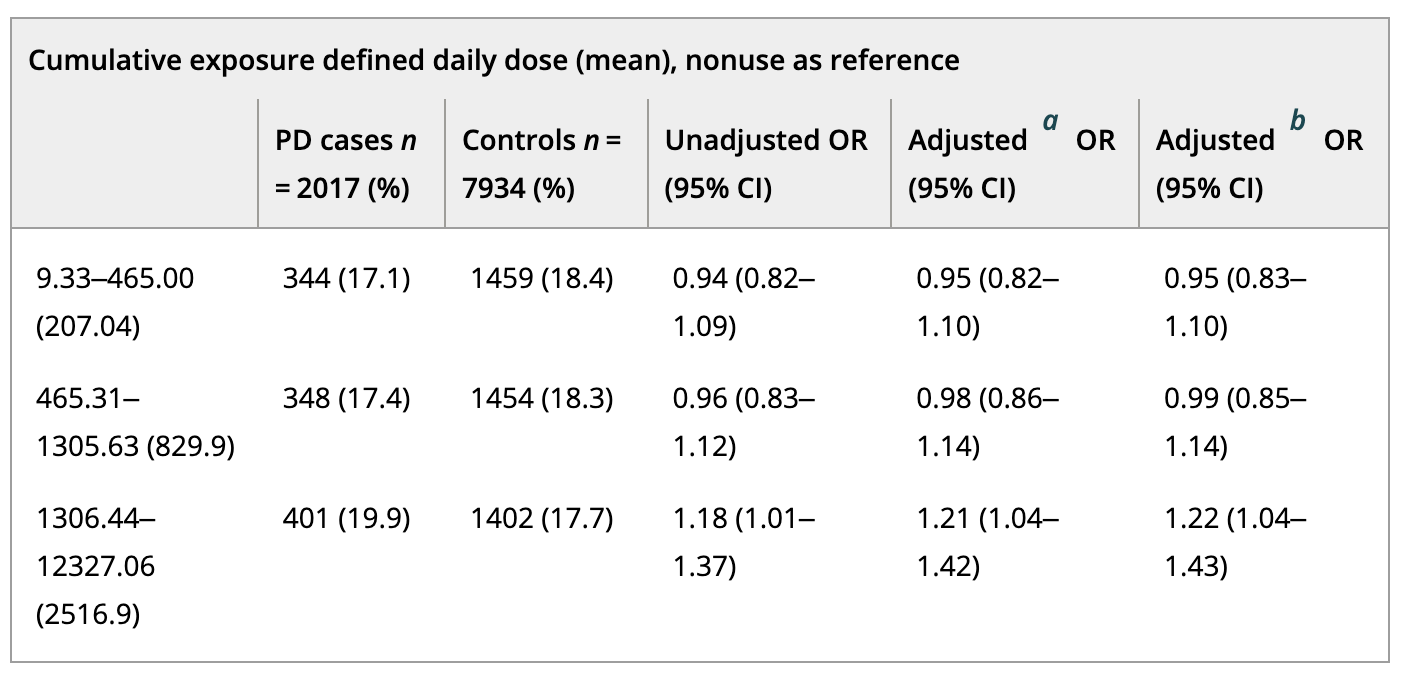
A nationwide study that controlled for diabetes duration and used a 3-year lag between exposure and outcome to account for reverse causality does not provide support for the hypothesis that statin use decreases the risk of Parkinson’s: Statin use and the risk of Parkinson’s disease in persons with diabetes: A nested case–control study 2024
Any statin use before the 3-year lag was not associated with the risk of PD (adjusted odds ratio [aOR] = 1.03; 95% confidence interval [CI]: 0.92–1.15; Table 4). In the dose–response analyses, an increased risk of PD was observed in the highest statin exposure tertile compared to statin nonuse (aOR = 1.22; 95% CI: 1.04–1.43). Similarly, in the secondary analysis restricted to statin users only, an increased risk of PD was observed in the highest exposure tertile compared to the lowest exposure tertile (aOR = 1.29; 95% CI: 1.07–1.57).
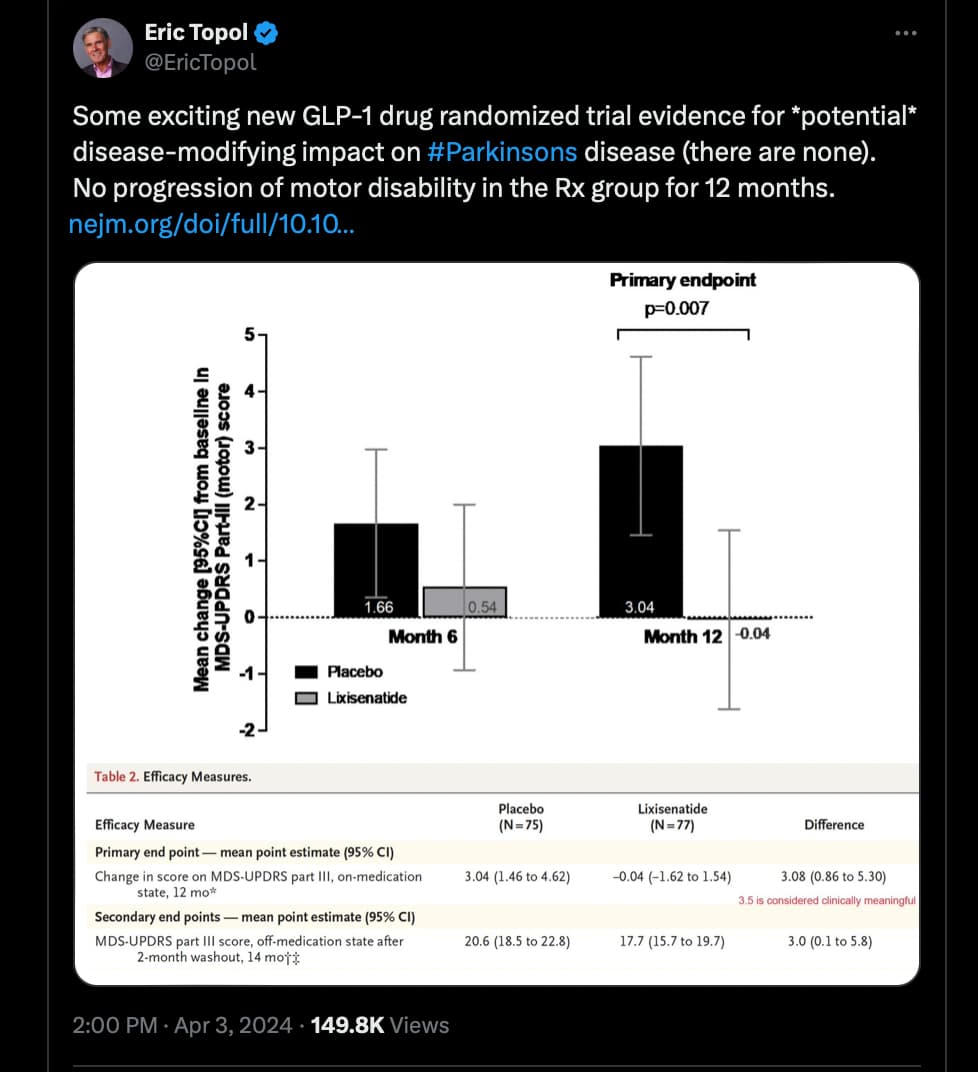
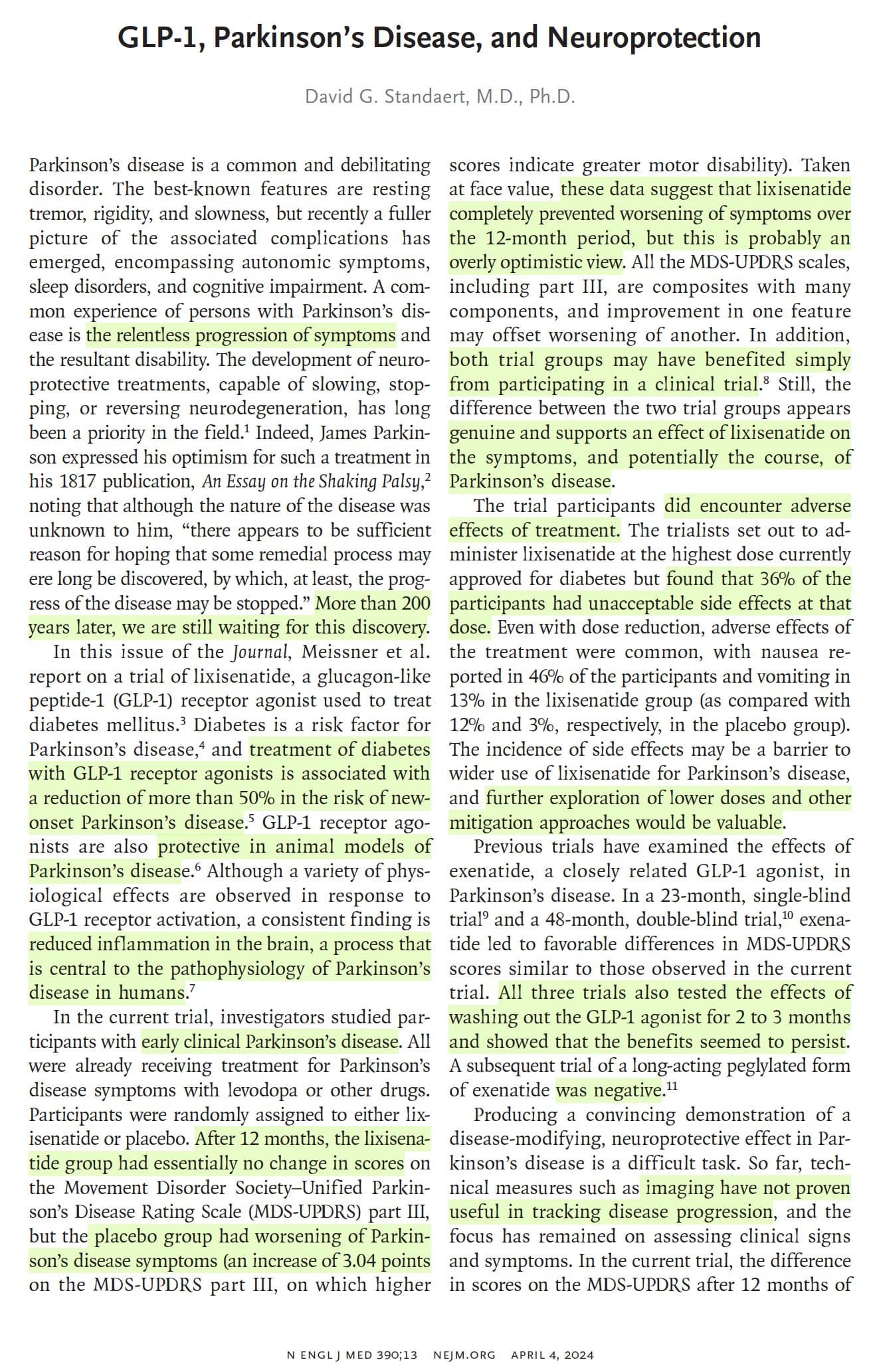
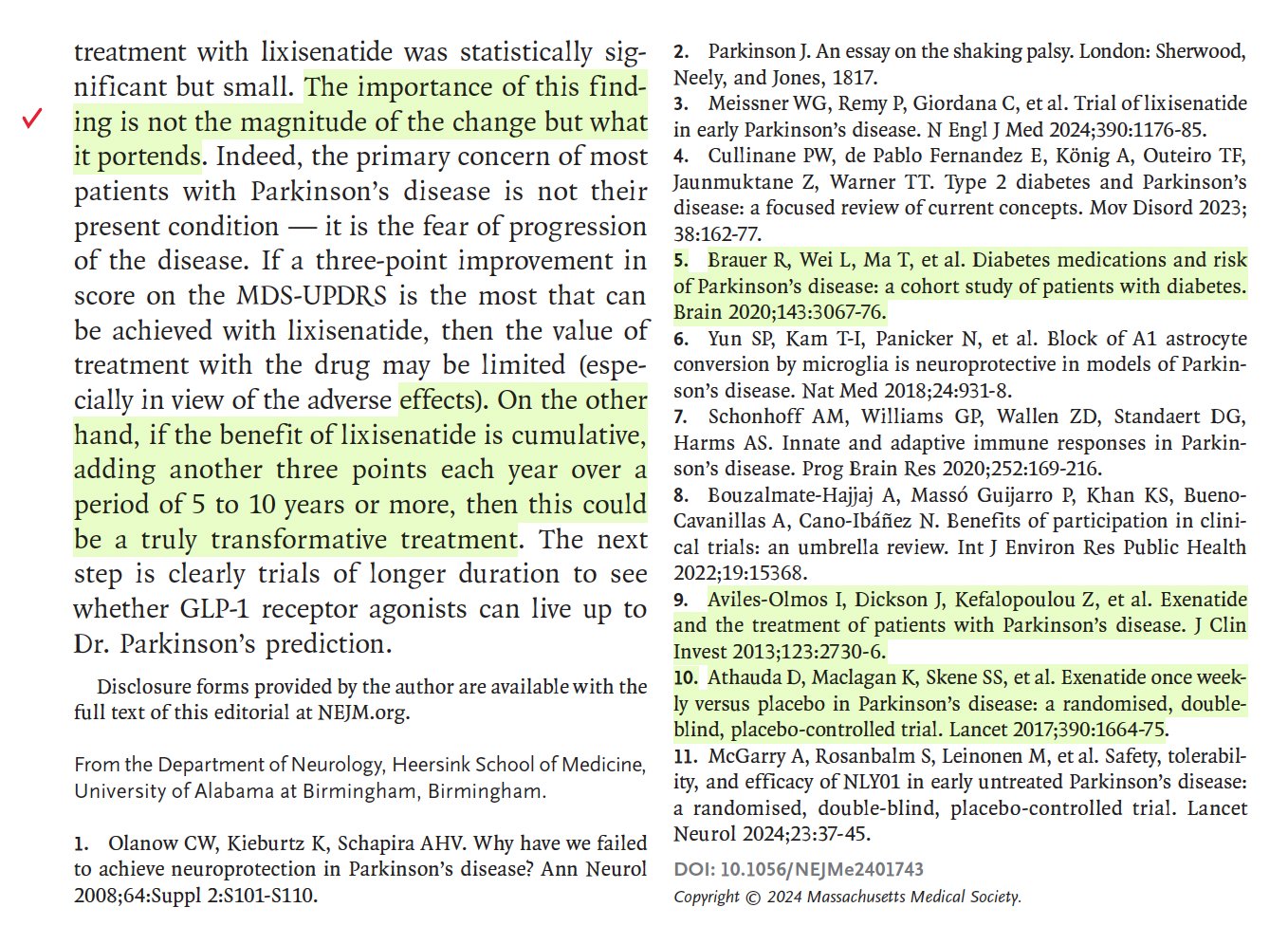
https://x.com/EricTopol/status/1775629568671629576?s=20