Why don’t you just get a standard lipid panel + apoB?
Use
apob.app
1.23 g/L
I did nut binge a few days before that test (but one entire 1 gallon box in a few days which isn’t the worst I’ve binged). I did try to eat some walnuts a few weeks ago
The exact mechanism by which statin therapy is associated with an increase in the proportion of small, dense LDL is unclear. One possible mechanism is that up-regulation of LDL receptor activity by statins decreases large, buoyant LDL more than small, dense LDL, because statins increase LDL receptor activity and because large, buoyant LDL is a better ligand for the LDL receptor than is small, dense LDL.23 More than 90% of apo B is found on LDL particles, and therefore patients with small, dense LDL (which is relatively low in cholesterol) would be expected to have a low LDL-C/apo B ratio, as has been described previously.17,24 The present study showed that statin therapy was associated with a greater decrease in apo B than in LDL-C, although in the group treated with statins, the levels of LDL-C and apo B were significantly lower than those in the control group. This result suggests that statin therapy is associated with a decrease in total LDL-particle concentration but with a higher proportion of small, dense LDL. In addition, these results support a possibility that statin therapy increases the proportion of small, dense LDL, although controversy still exists as to whether or not statins decrease the small, dense LDL subfraction and increase the LDL peak particle size.9–11 The present study brings up a fundamental question regarding the actual role of small, dense LDL in atherosclerosis.
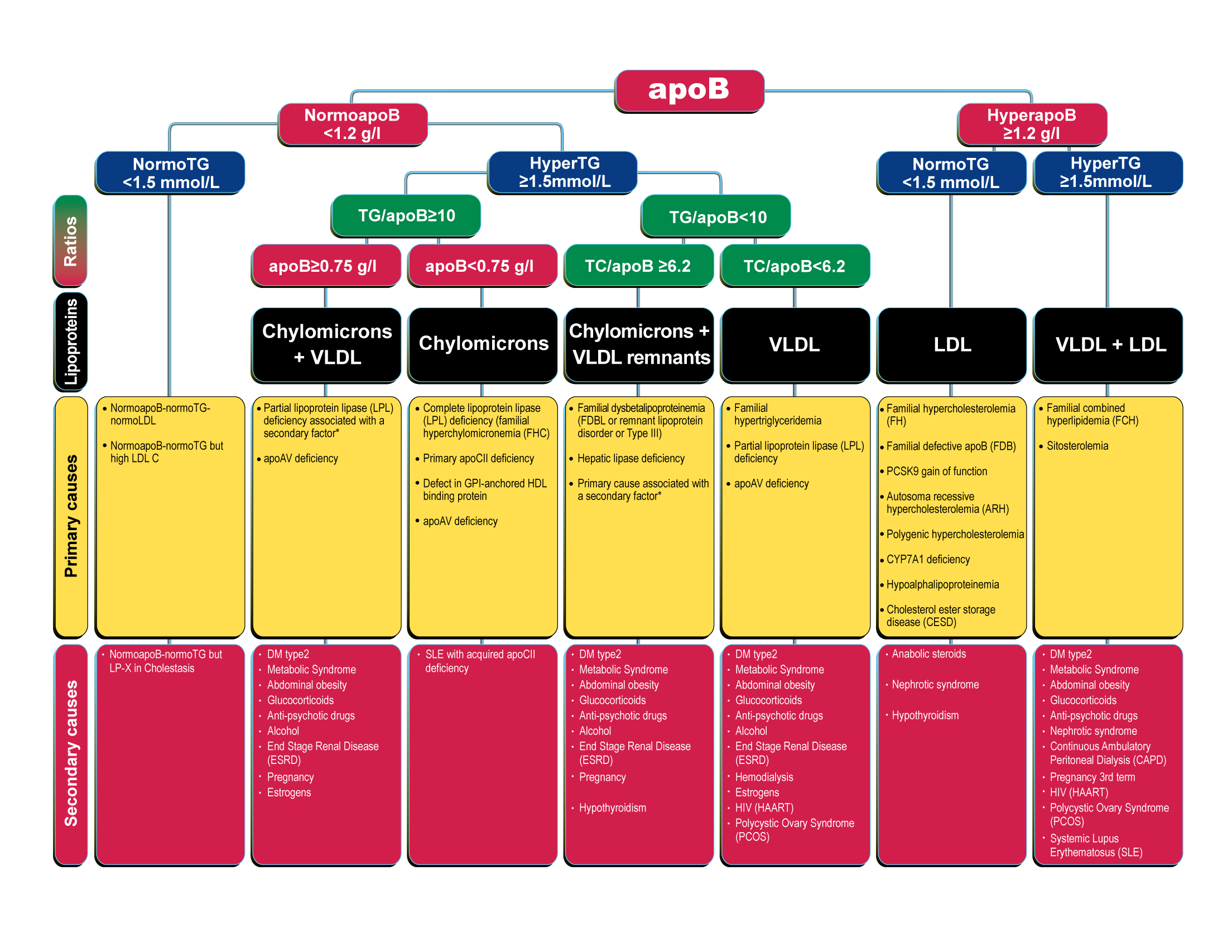
So you have hyperapoB according to apob.app, and around the same percentile as the LDL-P which is as expected.
Statins lower apoB by around 30% in clinical trials, I think it’s very unlikely it is the reason why your apoB increased. What’s your percent calories from dietary fat?
I would try 10 mg atorvastatin every day for 4 weeks then retest apoB and standard lipids, it seems pitavastatin (Livalo) is best for asian ethnicity according to perplexity so if you can get that might be preferable, a small dose. I don’t think it’s the reason for this result, just I’ve rememberd something about specific about statins for asian ethnicity.
probably 30% calories from fat, but it varies from day to day (i might have a nut binge every other week).
pitavastatin for side effect reduction in Asians, or actually hgiher cholesterol reduction?
I don’t think it’s from the dietary fat / nut consumtion then.
Side effects possibly or dose titration.
There’s warnings in some places about East Asian descent and statins, in official, formal places.
This is cool as well
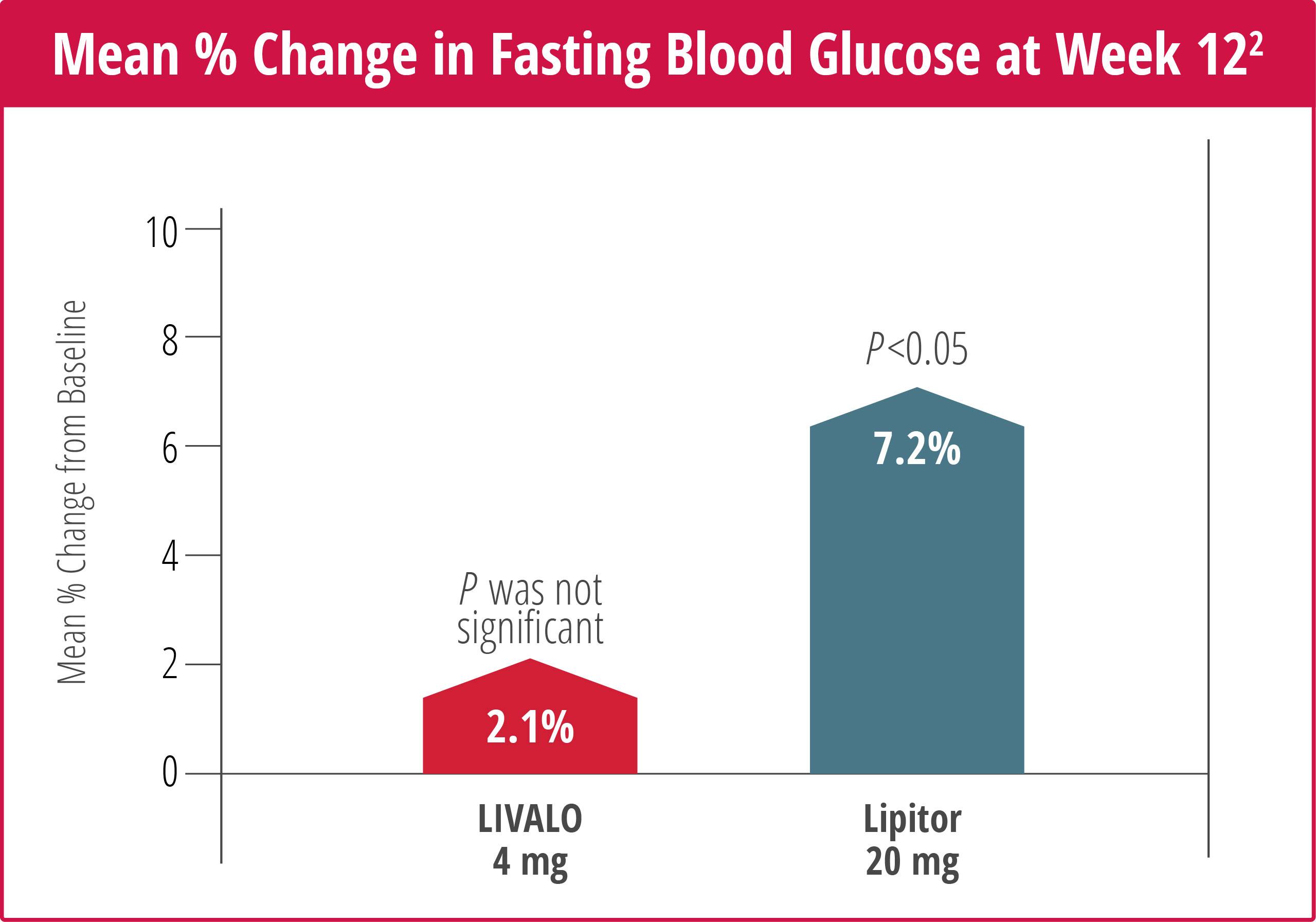
shit, does rosuvastatin also increase blood glucose?
[my nexlizet at least is being reshipped]
my fructosamine went a bit down from 268 to 252, it seems like a good way to measure if you are having problematic changes in glucose (way better than hemoglobin a1c)
I eat LOTS of beans and tomatoes…
Atorvastatin is better than rosuvastatin for diabetes risk according to a large RCT in SK. Not everyone gets increase in glucose but it does happen.
a previous study, 56 healthy participants received a diet that contained high amounts of saturated fat for 2 weeks; and subsequently were randomized to one of three dietary intervention treatments; refined olive oil, rapeseed oil or sunflower oil as the principal source of fat for 4 weeks. The results showed that during the oil diet phase, LDL size significantly reduced though differences between groups were not significant and oil consumption did not significantly change LDL size variation [46]. In a recent report, 40 healthy subjects were randomly allocated to drink an inositol-enriched beverage (IEB) that contained inositols 2.23 g in 250 ml or a sucrose-sweetened beverage (SB) twice daily for 12 weeks. The study showed that those subjects in the IEB arm had a significant increase in LDL particle size compared to the SB group [42]. Shrestha et al. conducted a randomized, crossover study, in which 33 healthy adults were allocated to treatment cookies (7.68 g/d psyllium and 2.6 g/d plant sterols) and a placebo cookie (0 g psyllium and plant sterols) for 4 weeks (each separated by a 3-week washout period). At the end of the study, psyllium and plant sterol cookies reduced the medium-small LDL particles, and markedly increased mean and peak LDL particle sizes compared with placebo [47, 48]. In a randomized double-blind clinical trial, 54 adults with LDL-C level ≥ 3.33 mmol/L were randomized into two groups to receive four capsules of phytosterol esters (2.6 g/day phytosterol esters) or placebo (canola oil) per day for 12 weeks. At the end of the study the proportion of LDL, mean and peak LDL particle sizes did not differ between groups [49]. Matvienko et al. conducted a clinical trial study in which 34 men with moderate hypercholesterolemia and hypertriglyceridemia
Our Ingredients – Unbun Foods. is full of it
This study showed that adding supplement of omega-3 fatty acid 4 g/day to statin therapy significantly increased LDL particle size
4g/day… Yeah I better binge on them
In a double-blind, controlled, crossover study, 48 men and 106 women with abdominal obesity and subclinical inflammation were randomized to a sequence of three treatment phases: phase 1, 2.7 g/d of EPA; phase 2, 2.7 g/d of DHA; and phase 3, 3 g/d of corn oil. All supplements were provided as three 1-g capsules for a total of 3 g/d. The 10-week treatment phases were separated by a 9-week washout period.
Main Outcome Measure
In vivo kinetics of apolipoprotein (apo)B100-containing lipoproteins were assessed using primed-constant infusion of deuterated leucine at the end of each treatment in a subset of participants (n = 19).
Results
Compared with EPA, DHA increased LDL-C concentrations (+3.3%; P = 0.038) and mean LDL particle size (+0.7 Å; P < 0.001) and reduced the proportion of small LDL (−3.2%; P < 0.01). Both EPA and DHA decreased proprotein convertase subtilisin/kexin type 9 concentrations similarly (−18.2% vs −25.0%; P < 0.0001 vs control). Compared with EPA, DHA supplementation increased both the LDL apoB100 fractional catabolic rate (+11.4%; P = 0.008) and the production rate (+9.4%; P = 0.03).
2.7g DHA a day, I better do it and not chicken out… it’s easy enough to take the omega-3’s…
meanwhile my PCP won’t prescribe statins or get particle sizes, and the cardiologist’s next appointment is next year but it’s fine, I can manage all with self-medication
I’m eating more chia seeds. I dont like their taste very much, but it means that I eat them when I’m really hungry, which can substitute for other binges or ubereats. and I seem to never binge on them. They seem to be more uniquely good for me.
They taste worse than flaxseeds, which is also good for me.
Anyways I guess I’ll try to retest in like 2 weeks
I mean it’s unlikely that no one controls ASI so why would you worry that much about microplastics and binges, the next years matters the most, maybe the next 10 years since humans are still needed for manual labor. Binges and MP’s matter in the scenario of no ASI, then taking some nexlizet could be considered enough and some other relatively easy interventions.
It’s still not a 100% probability of ASI happening
But I don’t like making life harder than it is, so semaglutide and nexlizet and canagliflozin should do most of it. It’s certainly true near-term tail risk from sudden cardiac death/heart disease is way higher than tail risk from slightly increased aging
I’ve been eating A LOT of canned food the past half year.
![]()
I think you’ve come up with the ‘most reasonable’ answer given all available information and for relatively younger chronological age <50 yrs old. I think I am going to lean towards 1000 kal whatever I feel like in my first meal of the day, then maybe 500 kcal ‘healthier’ basically to get fiber and other things that make life more pleasant, and body composition, and maybe some other nutrition (at a total -500 kcal deficit right now, if my maintenance is 2000 kcal). (If I was chronologically older I might optimize more).
Why only semaglutide and nexlizet, no SLGT2i etc? Or is that in order of priority, meaning if you were taking two meds those are the best?
Also I wouldn’t worry about heart disease in next decade or two, it takes more then that unless lipids in FH territory. I just think it’s good to take it just like it’s good to invest some money, in case of long ASI timelines.
yes i do canagliflozin too, it’s very low-effort and low-risk (lower than rapamycin). And acarbose
Anyways, it incrementally helps decrease mental decline and that matters
also, being able to stay cute matters a lot to me (and has personally has extremely important social effects, especially for giving me more second chances in life).This is why I still take really good care of my health - being able to stay cute for 5-8 more years makes a huge difference (esp b/c I got adopted once and that changed my life so much for the better).
If AGI timelines are ~10-15 years away (these seem conservative estimates now, but w/e), staying cute matters even more for my well-being than living longer.
But most things in life are harder than in theory, and many theoretically possible things have just been intractably difficult for some reason or another (fusion power, flying cars, nanotech, etc). If self-play/synthetic data doesn’t work, the models look fucked - you’re never gonna get anywhere near that platonic irreducible loss. Also, the theoretical reason to expect scaling to keep working are murky, and the benchmarks on which scaling seems to lead to better performance have debatable generality.
So my tentative probabilities are: 70%: scaling + algorithmic progress + hardware advances will get us to AGI by 2040. 30%: the skeptic is right - LLMs and anything even roughly in that vein is fucked.
they have one of these. maybe iollo covers them too, i’d have to check again
What about estriol in your list for some of your goals? I don’t think it should be longer than that, as long as estriol doesn’t have bad side effects…
yeah I have estriol, the amount of plastic around it is worrisome.
I may get an estradiol Rx in a couple of weeks, I can always stop and restart if the amount of feminization is too high
What’s the side effect profile compared to estriol, too much feminization aside? Possible long-term cancer risk?
Increased breast cancer risk doesn’t really matter for males
Too much feminization is the main side effect, I don’t want breasts
==
anyways, while my LDL is high it’s impt to increase astaxanthin and taurine to reduced oxLDL