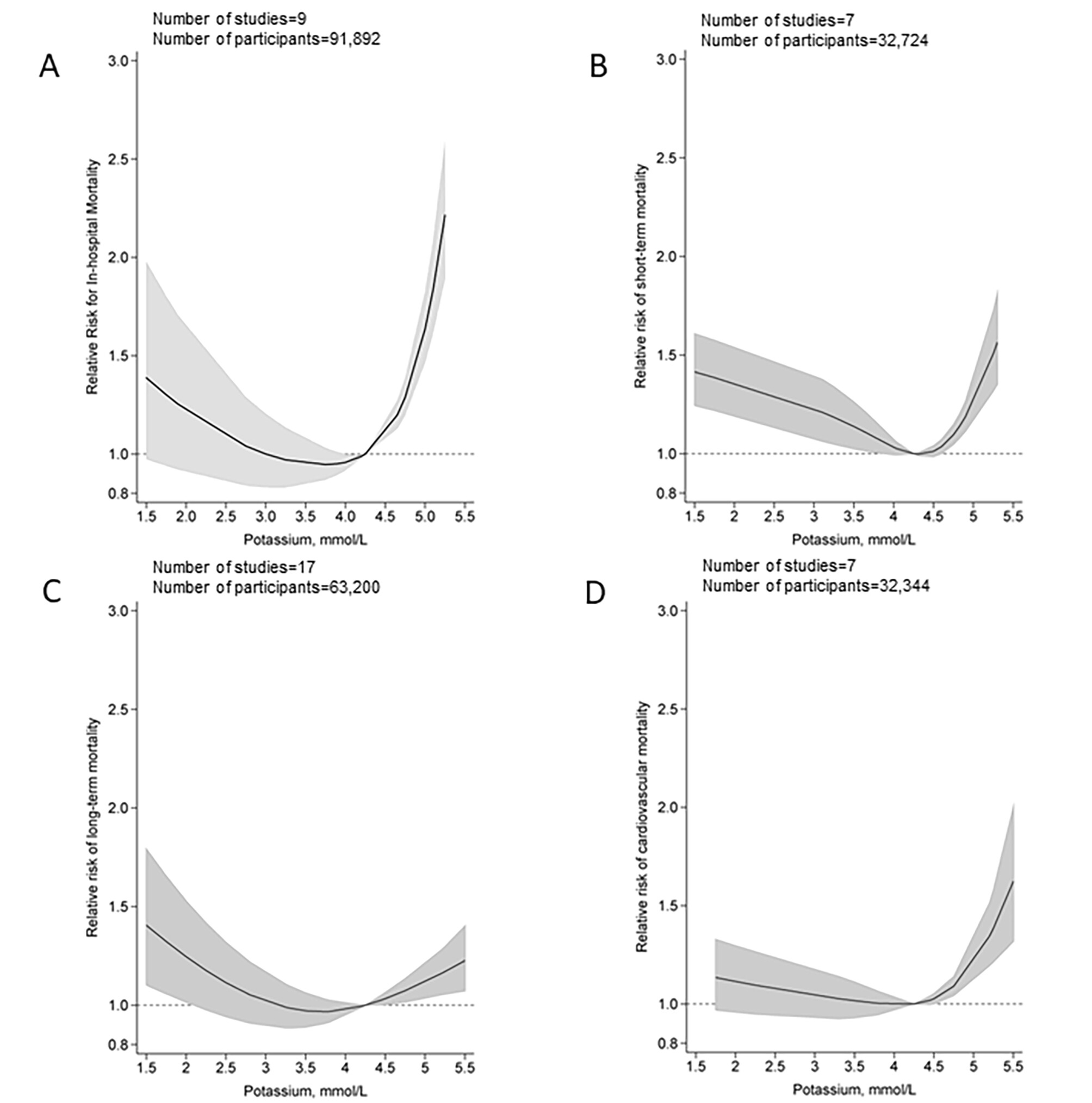
In the dose-response analysis, the association between blood potassium levels and all-cause in-hospital mortality appeared to be nonlinear (Pnon−linearity<0.001; Fig. 3; Figure 25 in Additional file 34). The risk of all-cause in-hospital mortality decreased with increasing potassium levels up to 3.9–4.2 mmol/L. When the potassium level exceeded 4.2 mmol/L, an increased risk of mortality tended to be evident with the magnitude of risk increase being stronger for potassium levels beyond 4.5 mmol. Even for the participants with a potassium level of 5.0 (equivalent to upper limit of normal range), a 65% higher risk of all-cause in-hospital mortality (RR:1.65, 95CI%:1.48,1.86) was observed compared with those with a potassium level in 4.2 mmol/L. Similarly, a U-shaped association was observed for all-cause short-term mortality across the potassium levels (Pnon−linearity<0.001), with the lowest risk associated with potassium level of around 4.2 (4.2–4.5) mmol/L. The risk of mortality tended to increase linearly for blood potassium levels ≥ 4.5 mmol/L (RR per mmol/L increment: 1.05, 95%CI:1.04,1.05). For all-cause long-term and cardiovascular mortality, the dose-response analysis also suggested a U-shaped association between potassium levels and mortality with a nadir of 4.2 mmol/L (Pnon−linearity<0.001).
In this multicenter, open-label, event-driven, randomized superiority trial conducted in Denmark, we enrolled participants at high risk for ventricular arrhythmias (defined as those with an implantable cardioverter–defibrillator [ICD]) and with a baseline plasma potassium level of 4.3 mmol per liter or lower. Participants were randomly assigned, in a 1:1 ratio, to a treatment regimen aimed at increasing the plasma potassium level to a high-normal level (4.5 to 5.0 mmol per liter) by means of potassium supplementation, a mineralocorticoid receptor antagonist, or both plus dietary guidance and standard care (high-normal potassium group) or to standard care only (standard-care group). The primary end point was a composite of documented sustained ventricular tachycardia or appropriate ICD therapy, unplanned hospitalization (>24 hours) for arrhythmia or heart failure, or death from any cause, assessed in a time-to-first-event analysis.
Among the 1200 participants who underwent randomization (600 assigned to each group), the median duration of follow-up was 39.6 months (interquartile range, 26.4 to 49.3). A primary end-point event occurred in 136 participants (22.7%; 7.3 events per 100 person-years) in the high-normal potassium group, as compared with 175 participants (29.2%; 9.6 events per 100 person-years) in the standard-care group (hazard ratio, 0.76; 95% confidence interval, 0.61 to 0.95; P=0.01). The incidence of hospitalization for hyperkalemia or hypokalemia was similar in the two groups.
There is always a question as to whether a biomarker might cause something to happen or be symptomatic of a situation.
Obviously you can be in a problematic situation (hyperkalemia or hypokalemia), but if it were to be that potassium levels were linked to biological age then that is useful information, but not necessarily something to target.
Somewhat interesting for people with those heart conditions. But optimum potassium levels for people without diagnosed heart disease, also very interesting, perhaps not these particular studies.
Might be relevant. Because we do know that ACM increases sharply when serum sodium levels start approaching the upper band of the “normal” range. Depressing for me, as my sodium levels were always at the upper edge, and in recent tests actually exceeded the upoer range and were flagged. Why, I have no clue, as I do not add sodium to my food, don’t consume processed food, and believe am on a low salt diet.
Its the Chloride that looks particularly bad rather than the Sodium. OTOH your kidney function looks reasonably good. Hence I would wonder about where all the Chloride is coming from or why you are not clearing it.
It does look something odd not related to kidney function per se.
One thing I have looked at more recently is the sensitivity of various metabolites to (urinary) pH. I don’t think that applies with Chloride. However, for things like Urate it is more soluble at a higher pH.
I didn’t have a simultaneous urine test at the time of the blood draw from which these numbers come, but every urine test I’ve had in the past has been absolutely fine - October 2024, the PH was 6 (ref. 5 - 8), and all the while my serum sodium and chloride numbers were high. I’m having my yearly physical late October, so I’ll see what my PC says. He’s never remarked on these numbers, since the rest are fine, but I’ll outright ask him this time - I suspect he’ll be perfectly useless, but at least I can say I was diligent in following up on my abnormal results, so if one day I grow a second head or croak suddenly, I’ll have a record of due diligence.
Sodium levels are tightly regulated by the body and isn’t really affected long term by diet as far as I know. So when someone has hypernatremia (in your case) or hyponatremia there could be some underlying problem.