The current dosage used like 6mg/week or 12mg every other week are not optimal in term of time in target range as we generally (*) want to avoid the side effects associated with large doses but using smaller doses does not keep the level at a therapeutic level long enough.
(*) Some might disagree here
Here is what I get when playing with my rapamycin pharmacokinetics model fitted to my blood tests.
BTW my rapa half life is 65.1h and I have 2mg pills.
First let’s compare 12 mg/2 weeks vs 6 mg/week
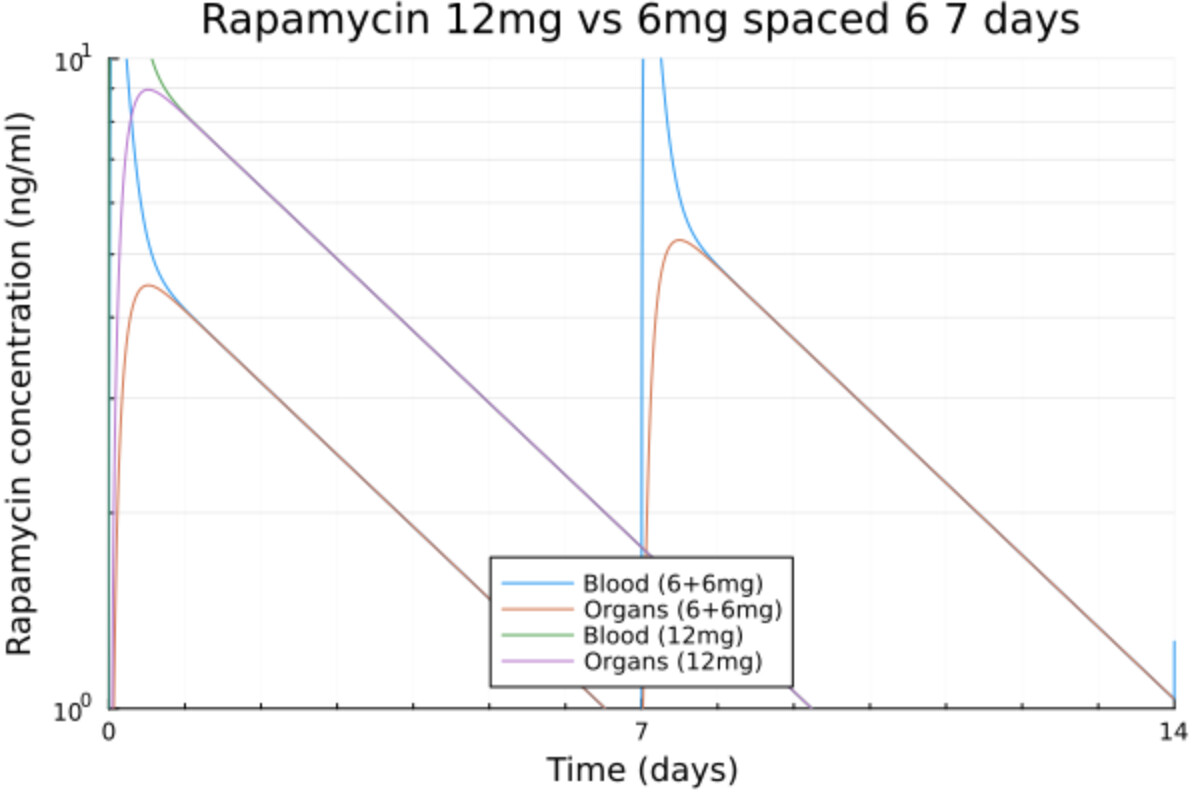
- The time over 3 ng/ml is globally similar.
- The maximum is twice higher for 12 mg as expected and reaches 9 ng/ml
- The trough is not low enough at 6 mg so there is an accumulation and the next dose is higher.
Now let’s try to improve that by splitting the 12 mg dose into 8+2+2 mg spaced 28h
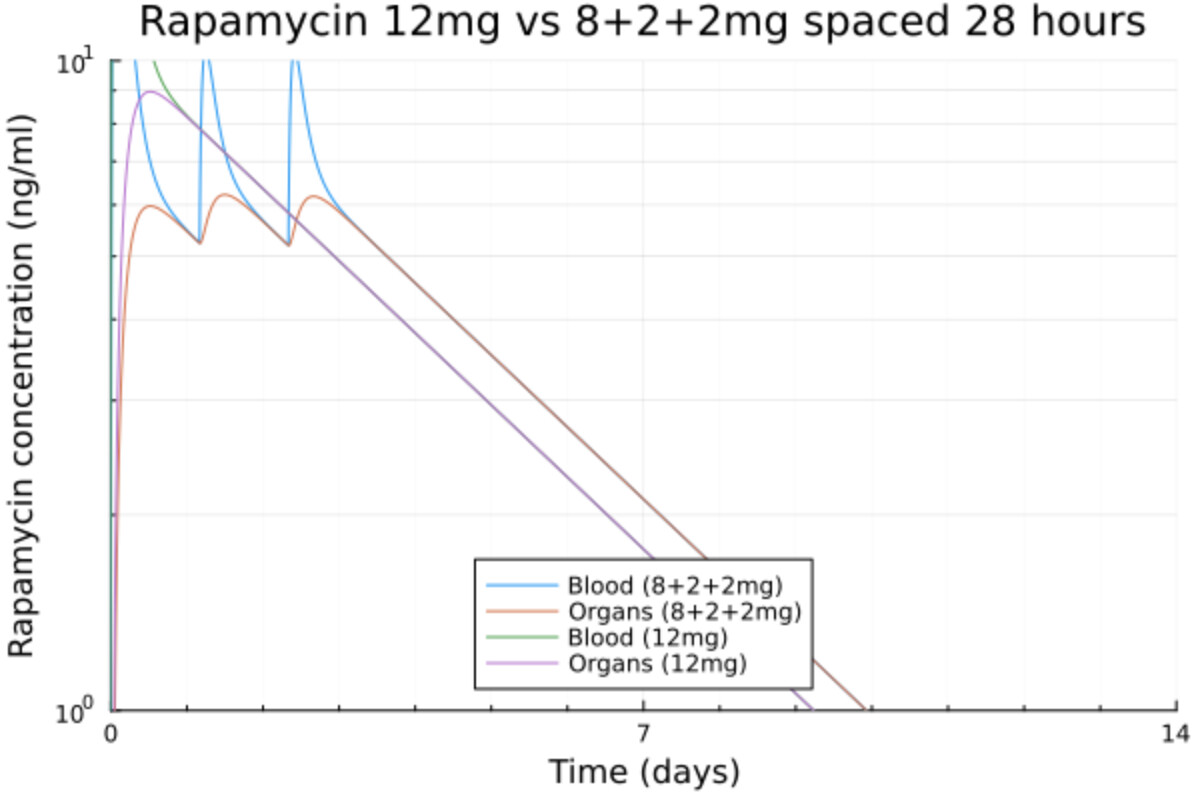
That’s better:
- The max is at 6 ng/ml
- The concentration is consistently mostly between 5 and 6 ng/ml
- The time over 3 ng/ml is almost 1 day longer
- There is a long enough period with very low levels of rapamycin to recover
Let’s look at 6+2+2+2mg spaced 40 hours
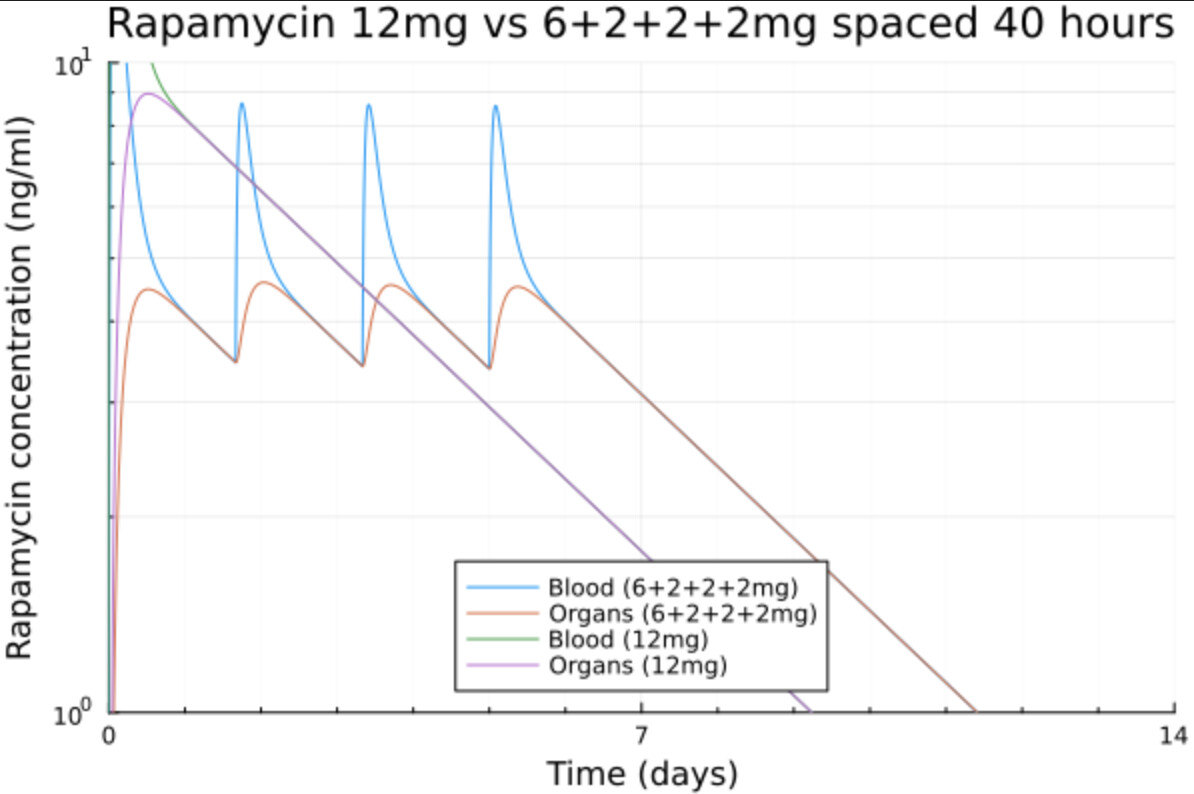
- The max is at 5.4 ng/ml
- The concentration is consistently around 4 ng/ml
- The time over 3 ng/ml is almost 2 days longer
- There is still a long enough period with very low levels of rapamycin to recover
With 1mg pills we can split even more and do 6+6x1mg
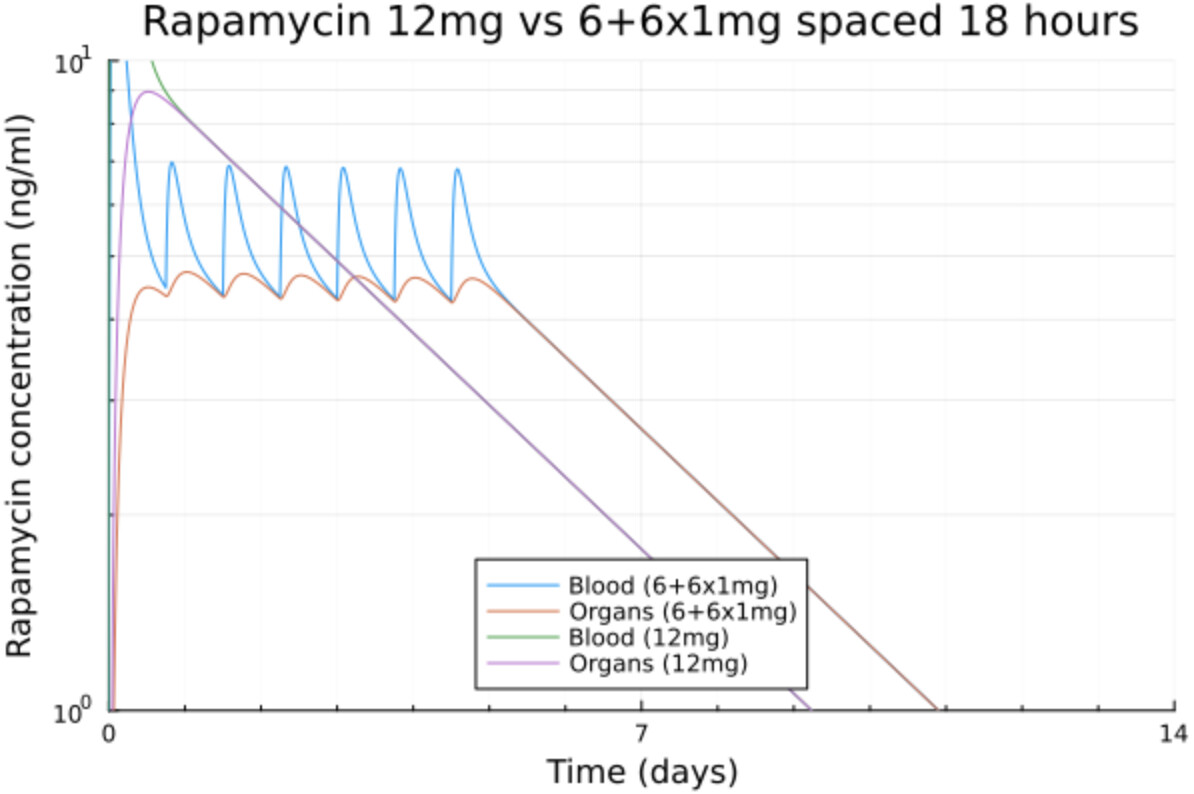
In fact we can get the level we want and extend it as long as we want. For instance here I go just above 3 ng/ml and extend it even more.
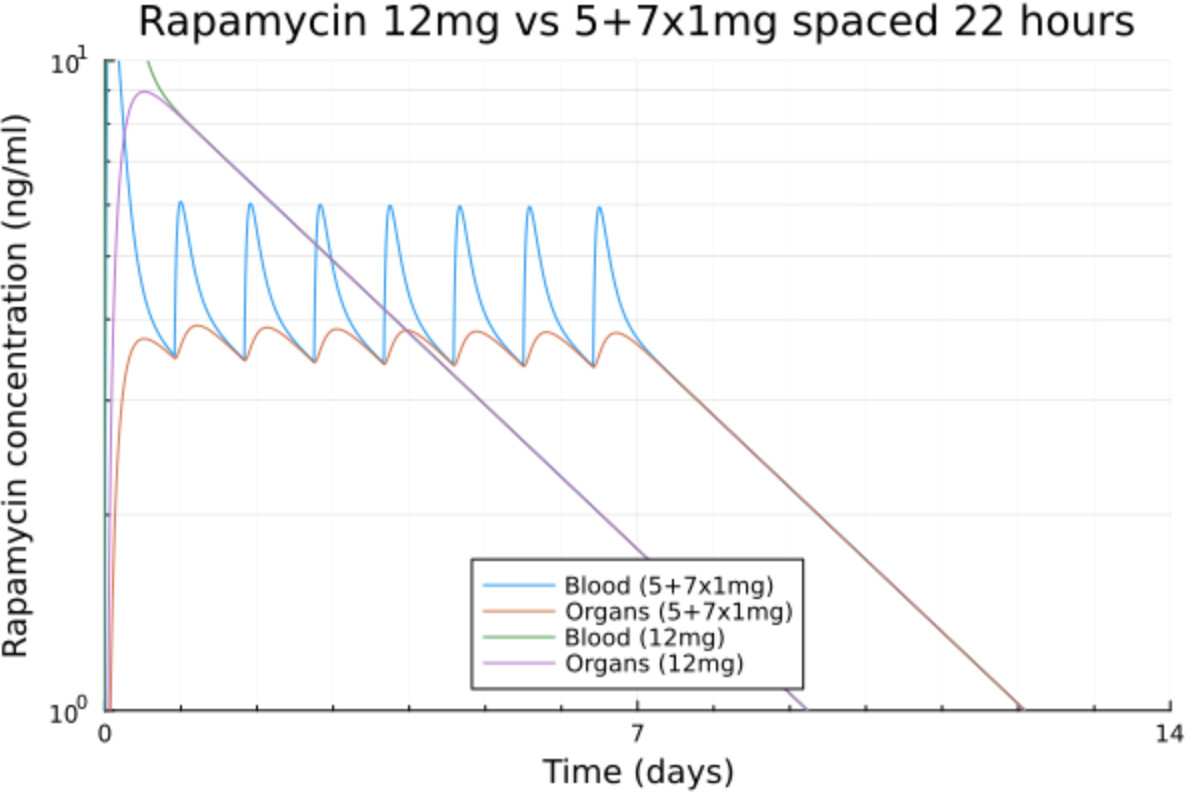
The time in range is now increased by 3 days with the same total dose.
Basically by splitting the dose into a starting dose to reach the desired level and then maintaining it by periodic small doses of 1 or 2 mg we can maintain that exact level for the time we want and we don’t get any high levels that can potentially cause issues.