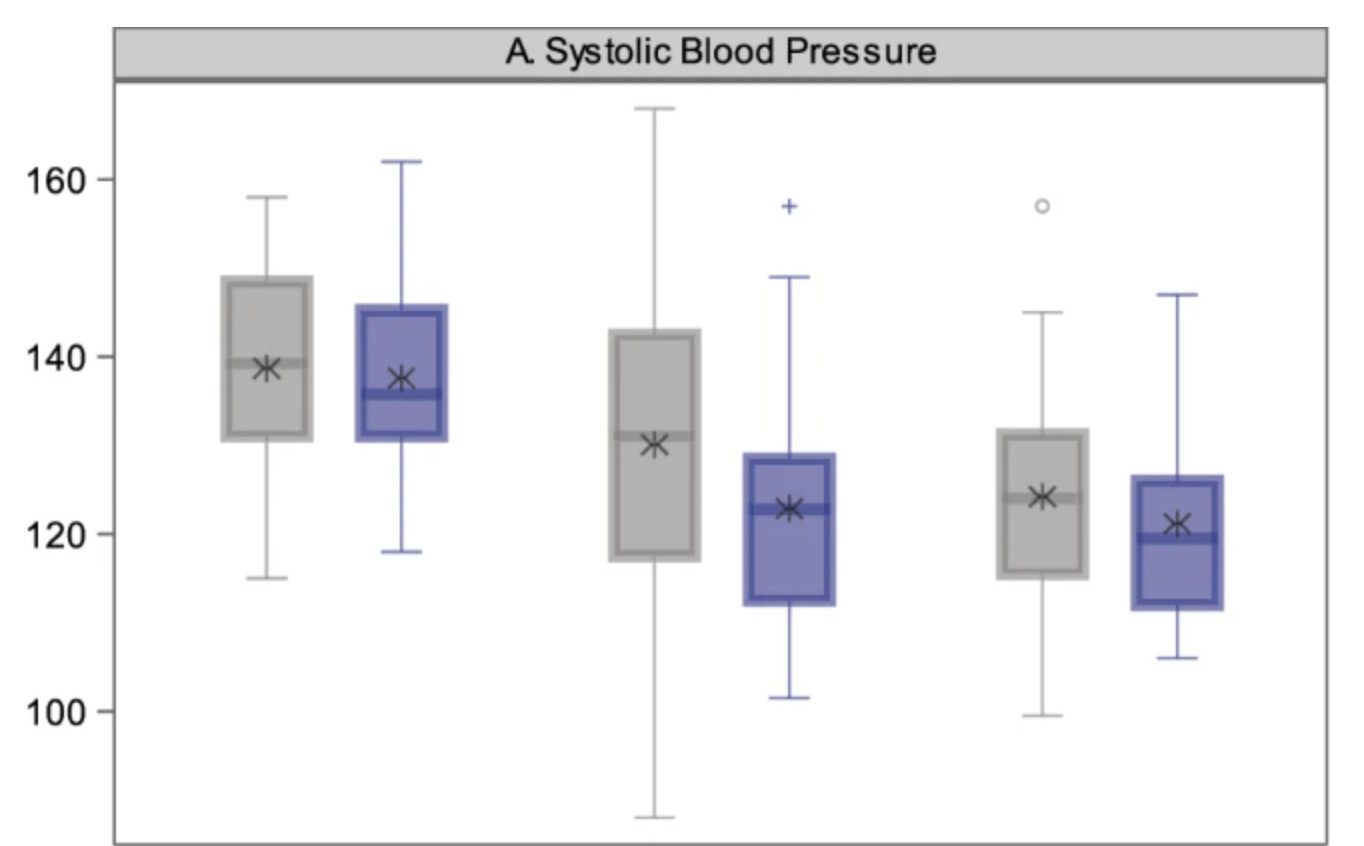
For GMRx2, they note: “The systolic BP (SBP)-lowering efficacy of GMRx2 strengths 1, 2 and 3 (Table 2) from a baseline SBP of 150 mmHg are expected to be approximately 13 mmHg, 18 mmHg and 25 mmHg, respectively.”
So how do you reduce SBP beyond 25 mmHg? I’d say:
Lifestyle: reduce alcohol and salt intake, use potassium salt, more exercise, eat less, sleep hygiene, etc.
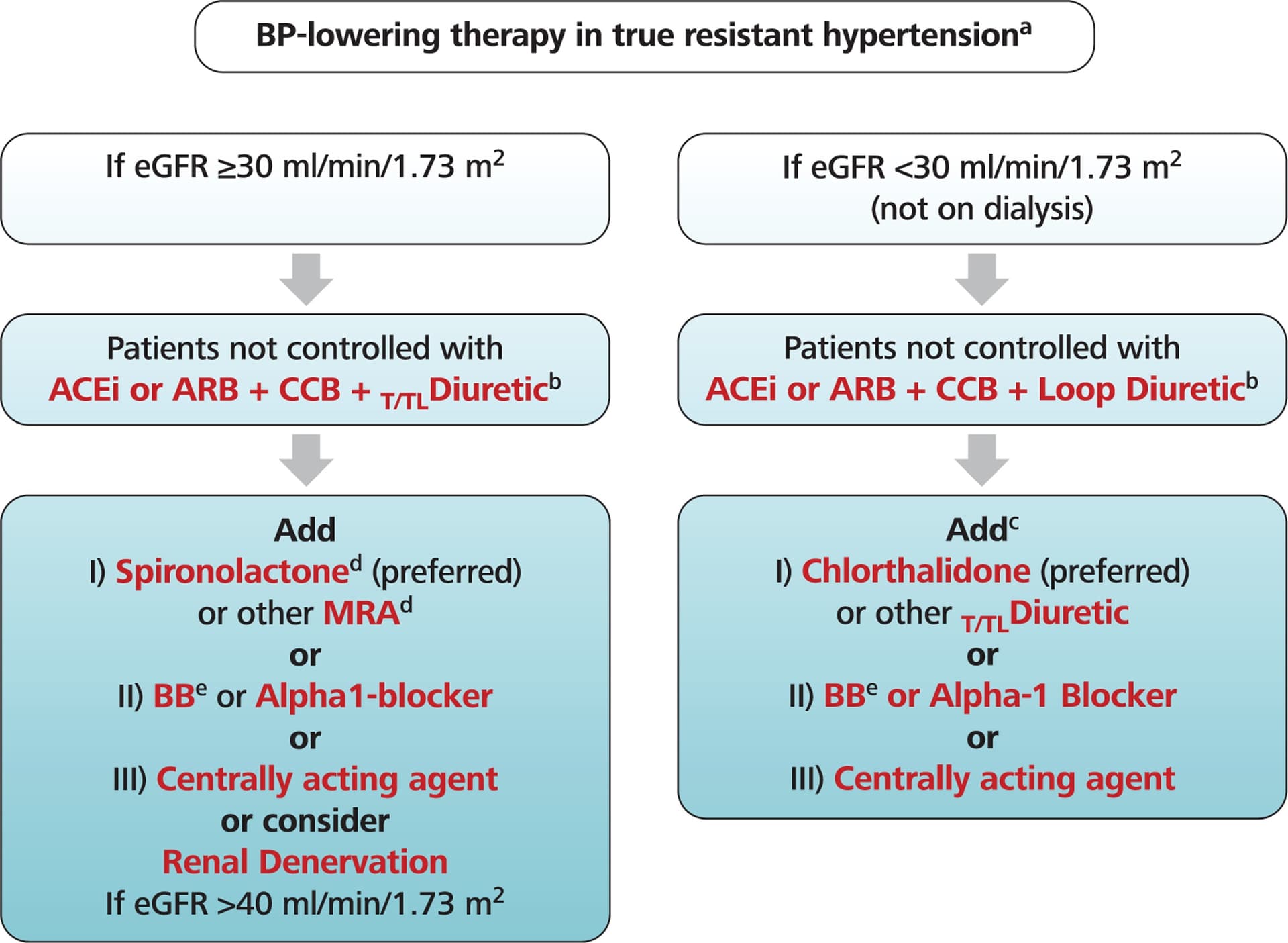
These guidelines are very sensible. I think the issue is tolerability. As people get older, the tendency to have significant postural changes is a real risk for falls and loss of consciousness. There is a need for careful advice on change of position and making sure everything is doing well before just going from lying to standing and heading off. Most agents have significant risks - and when we are looking at moderate/high doses of 3-4+ classes of medications, there has to be a careful evaluation of risk/benefits.
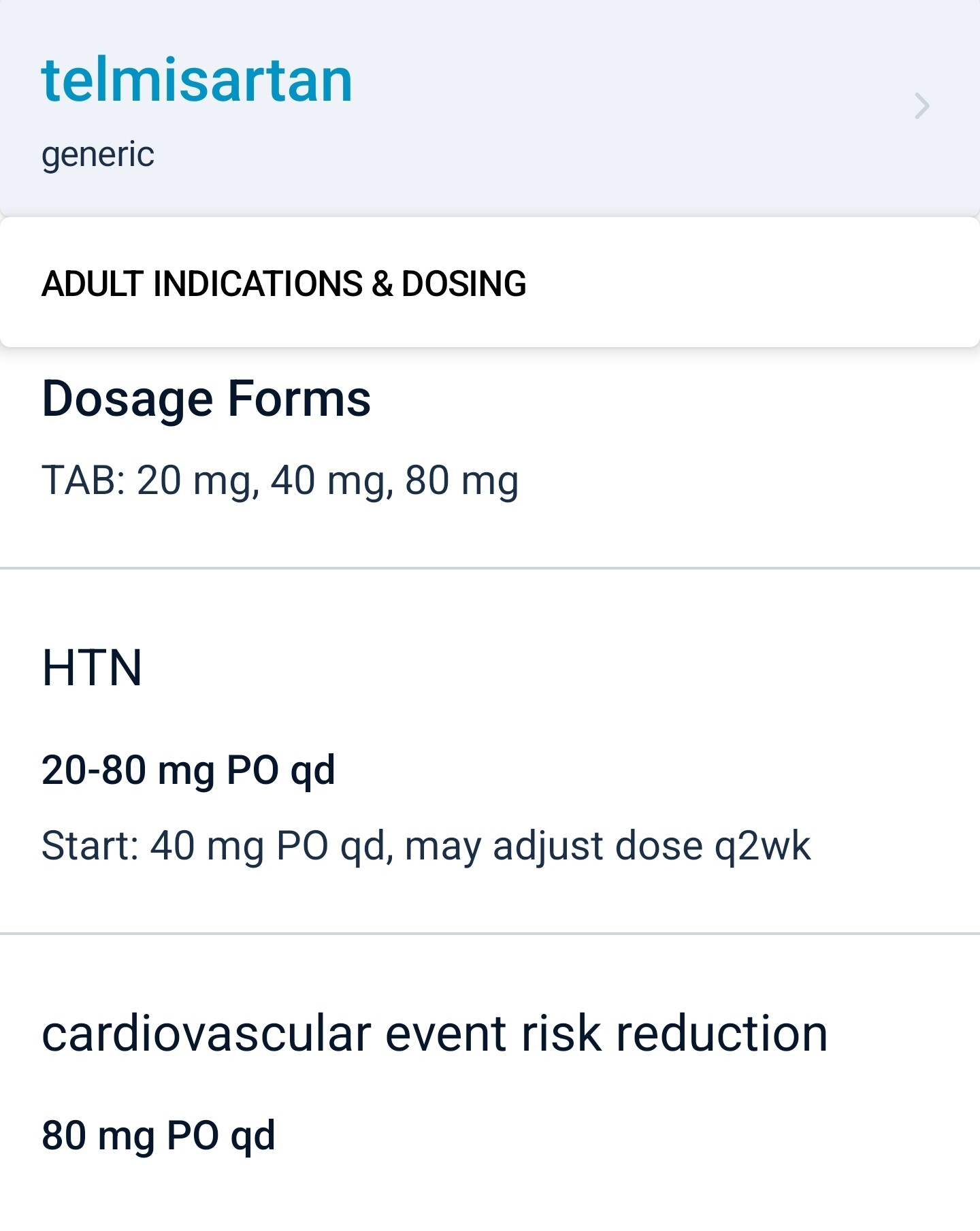
I find that I can get most people controlled nicely with no more than 3 agents - and I do go stepwise with telmisartan, then amlodipine, then indapamide unless there is a reason to do something else. In violation of the usual approach of not pushing the dose of any drug - I will maximize telmisartan as the neuroprotection seems to occur at 80 mg but not necessarily at 40 mg.
This is an interesting area where there is nuance. Just in the same way one looks at colon, breast, prostate cancer screening and consider at what age stop doing this? It shouldn’t be the age - it should be the anticipated years of quality life potentially remaining. So if a person is expected to only live another 5 years - tightly controlling their blood pressure isn’t sensible if it risks falls and loss of consciousness - if the life expectancy might be 20 years - then managing this becomes more relevant -similarly with cancer screening.
It is complicated when having a gestalt of how long someone will live. I think I have a pretty good sense of this … as there are people who are 35 years old who are not likely to see age 40, and there are people who are 80 that I think are likely to live to 100.
So this is an issue with PPAR-y activation which if one does a search on Pubmed you’ll see that the higher dose telmisartan seems to be important - whereas under 80 mg isn’t active.
You are much more skilled than am I finding all the references and citing them. But there are a whole lot in this space that I’ve looked through. I think if you are on telmisartan - this is a drug worth pushing to at least 80 mg before adding another drug. Also - for my patients who have risk of neurocognitive decline - if they have enough BP to allow adding this - as it usually doesn’t lower BP that much - I think it is very sensible to get them on this.
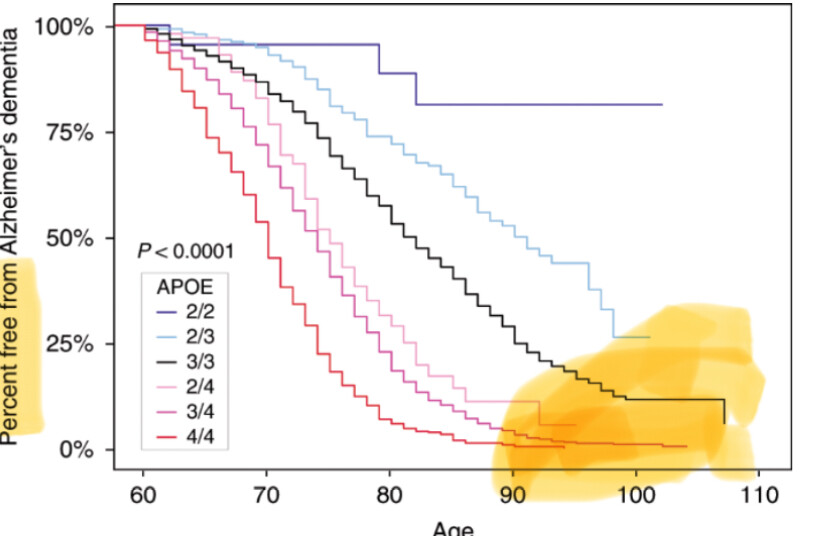
I must say the recent post by @RapAdmin showing dementia risk by ApoE status has me doubling down on the need to do everything possible to decrease risk and start as early as possible. My goal to live >100 years cognitively intact is threatened by my ApoE3/E4. I’m happy that I’m able to tolerate Telmisartan 80 mg with no seeming side effects.
I appreciate that Dr. Greger does cherry pick things a bit – but his take on ApoE is really interesting, given high prevalence on Nigeria, but low rate of AD. Here is a link to his video on this topic: https://www.youtube.com/watch?v=zQBJScaGxJI
I think if you target all of the diseases of time early and have optimal levels, like lipids, blood pressure and blood sugar, that will have an outsized impact on Alzheimer’s dementia via compounding benefits. This should be pretty much proven at this point based on effects from short term trials that are extrapolated with MR. It probably will have a larger impact than waiting for an Alzheimer’s drug as time under treatment might be very powerful.
I believe this will end up being the case. The evidence keeps moving in that direction. It is such an interesting time to see most newer agents for T2DM having efficacy in the neurocognitive decline space. The focus of pharma with AD currently has been a failure with nothing being disease modifying - same with Parkinson’s. The clock is ticking … and for many, taking a combination of agents seems sensible. There is a risk/benefit, but it seems like the major risk for most is simply cost and coordinating care.
It would seem unlikely to me that many primary care physicians would be keen to prescribe such a combination to prevent or slow disease. This complicates things for individuals who read the literature that their primary care physicians should be reading-- who then have to obtain medications outside the usual medical system as their only option to obtain the therapies that seem sensible based on current literature.
We know the targets and the best treatments for optimal BP and blood sugar. As said in the paper, it’s not as clear for lipids, but I’m convinced newer lipid-lowering drugs (e.g., PCSK9i and CETPi) will soon be proven to be neuroprotective. Then you have the big unknown of mental health and sleep: we don’t know the best way to measure it, the targets, the treatments, etc.
For adults over the age of 60, low blood pressure is generally defined as Systolic: Less than 90 mmHg, Diastolic: Less than 60 mmHg
“cardiovascular disease risk doubles for every 20 mmHg systolic or 10 mmHg diastolic
increase in blood pressure, starting at 115/75 mmHg. This means that the risk of death from stroke and ischemic heart disease (IHD) increases linearly and progressively from levels as low as 115 mmHg SBP and 75 mmHg DBP upward. These increased risks are present in individuals ranging from 40 to 89 years of age.”
It looks like 115/75 would probably be close to the sweet spot for most older people.
This would be for healthy people. Low blood pressure is a comorbidity of vascular diseases,
etc., in old people.
The director of the Center for Brain Health and Alzheimer Prevention Clinic at Florida Atlantic University provided perspectives on the multimodal, multitargeted approach needed to treat Alzheimer disease. [WATCH TIME: 5 minutes]
An overview of biomarkers and a bit of what the future holds
MASTER CLASS WITH DR. RICHARD ISAACSON
Alzheimer’s Prevention
Get practical, up-to-date information on Alzheimer’s risk reduction from Dr. Isaacson’s Alzheimer’s Prevention Clinic
I emailed them in Feb to ask about SGLTi, BPV (instead of just mean BP), low-dose lithium, neuromodulation (inc. light therapy), and non-statin lipid-lowering drugs (inc. obicetrapib). No answer so far.
You wrote: " Also, can you recommend a good blood pressure device that is accurate but does not break the bank?"
Sure, Buy a Littman Stethoscope for $60 on zon and a blood pressure cuff that is the proper size.
There are some good youtube videos on how to read it. It’s a bit intimidating at first but after a dozen tries you’ll get quite accurate.
No batteries, and it never breaks… and you can listen to your lower right lung lobe and tell you are getting pneumonia (it usually starts there) early.