I just read that telmisartan and Lisinopril can be used as a synergistic combination. As Telmisartan is an ARB and Lisinopril is an ACE. My mom’s BP is still too high as well.
1 Like
I think that American and European guidelines recommend not to mix ARB with ACEI. I don’t know why, but I wouldn’t do it. The most common combination is (ACEI or ARB) + (CCB or thiazide diuretic).
1 Like
Maybe we’ll just go for empagliflozin first. However she is worried empagliflozin may cause side effects.
What do you think about this?
”This analysis shows that risk of cancer and specifically lung cancer increase with increasing cumulative exposure to ARBs.”
A single unknown author (who is not even an oncologist) from a Turkish university. Unless there are other papers confirming this finding, that paper would go to the trash for me.
Here’s another paper coming out from German institutions in a specialized oncology journal: Risk of lung cancer and renin–angiotensin blockade: a concise review 2021
Results
International regulatory agencies (FDA, EMA) have concluded that the use of RAAS blockers is not associated with an increased risk of developing lung cancer. Co-administration of RAAS blockers to systemic therapy of advanced non-small cell lung cancer seems to have positive effects on the outcome.
Conclusion
Until more comprehensive analyses have been completed, there is no need to change clinical practise. Additional prospective randomized trials with long-term follow-up are needed to investigate the effects of these drugs on the development and progression of lung cancer.
2 Likes
Lebanese and Swiss team of oncologists: The association between angiotensin receptor blockers and lung, bladder, and colon cancer development: A 10-year multicentric retrospective Lebanese study 2023
ARBs use was significantly protective (P value = 0.000) against overall cancer development (odds ratio [OR] = 0.127) and against each, lung (OR < 1), bladder (OR < 1), and colorectal cancers (OR < 1). A duration-response relationship was established. This protective effect and the time-dependent relationship remained unchanged after omitting the most relevant risk factors. In summary, a significant overall protective effect of ARBs against lung, bladder and colorectal cancers was found. This beneficial response was time-dependent.
The trash is indeed the correct destination for the Turkish paper.
4 Likes
Yes, we’ve got to really be more skeptical of one off papers by sketchy sources.
3 Likes
True, I agree. There are a lot of conflicting results.
@Tim
White coat syndrome. It was 200/110 at the first measurement in the doctor’s office and 220 at the second one. I’ve always been the same - an increase in bp with each successive measurement at the doctors…… never as high as this previously though.
1 Like
Telmisartan is in the same family as losartan. It has a half life of 24 hours, versus about 9 for losartan. Telmisartan used to be expensive. But its patent expired in 2014, so now affordable.
5 Likes
Those who are taking amlodipine could try the hack below.
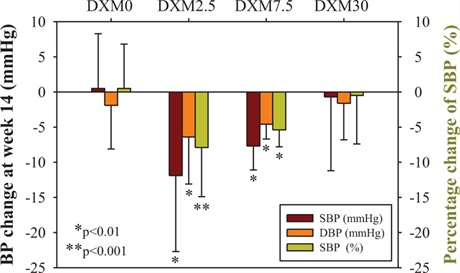
Blood Pressure Changes
In the DXM0 [dextrometorphan] group (n = 31), the mean SBP was 127.2 ± 6.9 mmHg at week 2, which remained stable with AM 5 mg daily through the end of the study. In the DXM2.5 group (n = 16), SBP reduced significantly and constantly from baseline. The reductions were 14.0 ± 8.1 mmHg (P < 0.001), 9.4 ± 12.1 mmHg (P = 0.007), and 11.9 ± 10.8 mmHg (P = 0.003) at week 6, 10, and 14, respectively. In the DXM7.5 group (n = 6), SBP was constantly reduced from baseline by 10.8 ± 10.2 mmHg (P = 0.049) and 7.7 ± 3.4 mmHg (P = 0.003) at week 10 and week 14, respectively. In DXM30 group (n = 25), there was no change in mean SBP from baseline to the end of the study.
2.5 mg is less than ten percent of the DXM dose for cough (30 mg); and that is a daily dose, compared to the four times a day dose for cough. So the daily dose is 2.5% of the dose for cough (120 mg).
Sample size is small - 103 patients.
DXM is also a NADPH oxidase inhibitor. So it may have longevity benefits.
A 2016 paper by a Taiwanese team, almost never cited… Has this finding been reproduced?
1 Like
Also: why the higher the DXM dose the lower the blood pressure lowering effect?!
Has this finding been reproduced?
None that I have found by searching. There seems to be few human studies on DXM, maybe because there is no money in it. It is an old drug. So patent must have expired.
Below is a human study on another possible application.
https://tvst.arvojournals.org/article.aspx?articleid=2718716
Also: why the higher the DXM dose the lower the blood pressure lowering effect?!
Not being a scientist, am not qualified to answer that question. Neither have I found the answer by searching.
I also have a white coat syndrome and my BP goes up much if I’m having a procedure done. And no medication can quickly correct it. Even clonidine fails. My endoscopy was canceled because of that. Other than that, my BP is usually normal and on a lower side. Stress is a killer!
2 Likes
There’s actually a lot of money put on DXM combinations with other drugs (for instance DXM and bupropion, Auvelity, for depression). And many generics are still widely studied (for instance statins and sartans). So in the absence of independent replication AND as we have many proven safe affordable alternatives I would avoid DXM for BP lowering.
@JuanDaw
I find that amlodipine at 10 mg, combined with 100 mg of losartan, effectively controls my BP. The problem for me with amlodipine is pedema, or swelling of the feet.
1 Like
Ask your cardiologist if you can decrease amlodipine to 2.5 mg: the edema should disappear (it is a dose-dependent effect, really common at 10 mg). To make sure your BP is still control, add a thiazide or thiazide-like diuretic like HCTZ (I forgot what the lowest dose is) or indapamide 1.5 mg SR.
1 Like
@adssx
Amlodipine is both dose-dependent and time-dependent. I’ve been on it for five years and the pedema appeared only recently. My nephrologist did suggest a diuretic. Maybe I’ll try a three-pronged attack: losartan, amlodipine, and a diuretic in appropriate dosages.
1 Like