I used to be a proponent of rapamycin + metformin combination, since AMPK activation + mTORC1 intuitively makes sense, especially seeing the ITP results from 2016.
It is important to note, though, that metformin had no significant effect itself on lifespan here, but there seemed to be an additive effect when combined with rapamycin (though that was referenced against historical data).
Research over the past few years suggests that metformin has negative effects on the metabolic response from exercise. For example doi: 10.1111/acel.12880
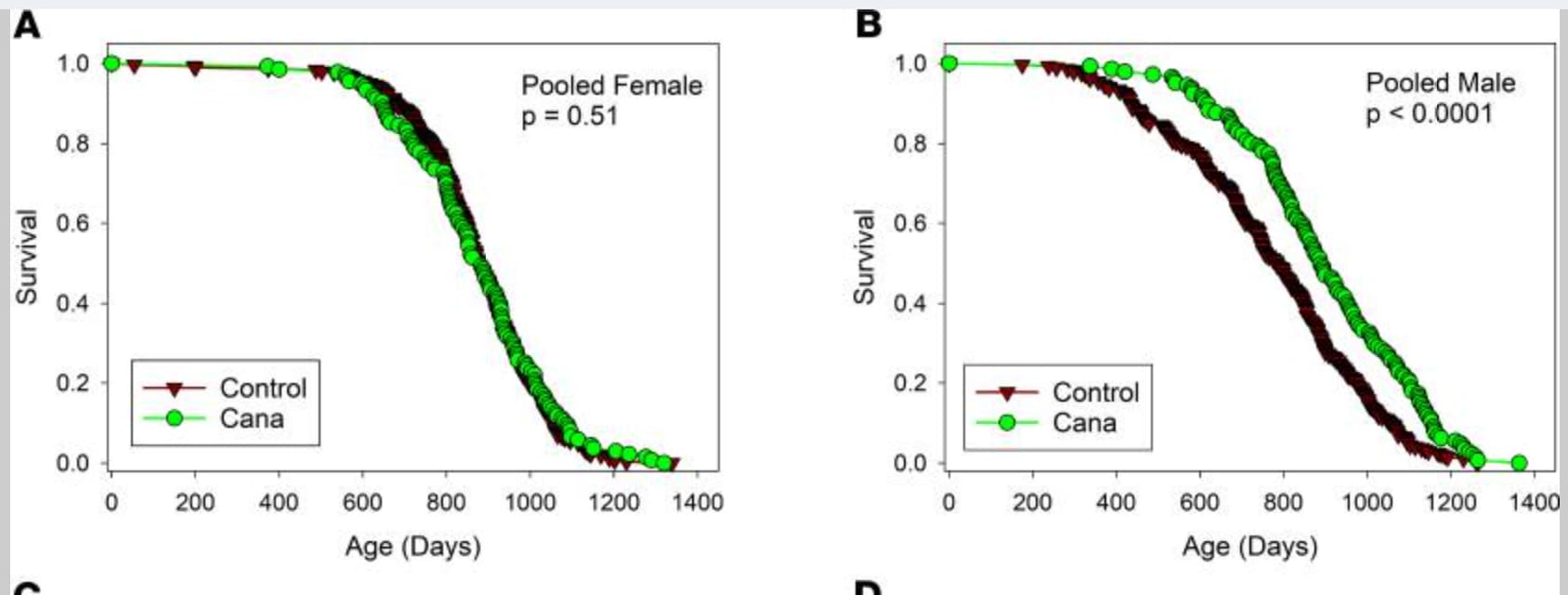
On the other hand, canagliflozin by itself was shown to robustly extend lifespan in the ITP in male mice (from Miller et. Al, 2020).
Other research suggests that canagliflozin also actives AMPK, similar to metformin: The Na+/Glucose Cotransporter Inhibitor Canagliflozin Activates AMPK by Inhibiting Mitochondrial Function and Increasing Cellular AMP Levels - PubMed
I would guess that the additive effect of Rapa + Met is due to the additional AMPK activation rather than control of glucose, since that should have shown up has an independent lifespan extension in male mice (like was seen in canagliflozin and acarbose). But even combining rapa with a “solely” glucose lowering drug like acarbose shows an even larger effect on lifespan in the ITP (see Strong et. Al, 2022). The life extension was very impressive in both male and female mice (28% in females and 34% in males).
Deep investigation into the effect of canagliflozin on exercise has not been done, to my knowledge, but early research suggests that it does not blunt the positive metabolic effects as is seen in metformin (it improves aerobic response): Canagliflozin Prevents Hyperglycemia-Associated Muscle Extracellular Matrix Accumulation and Improves the Adaptive Response to Aerobic Exercise | Diabetes | American Diabetes Association
Given that canagliflozin:
- Robustly lowers glucose and increases male lifespan in the ITP, suggesting an independent mechanism for lifespan extension from rapa by lowering glucose, similar to acarbose.
- Actives AMPK like metformin, whose combination with rapa appears to be additive for longevity.
- Does not seem to have bad metabolic effects on exercise, at least from early research.
I think it’s smart to substitute rapa + metformin for rapa + canagliflozin. I also would guess that rapa + canagliflozin would outperform acarbose, but that’s much harder to say with the currently available data.