Fish oil, omega-3s: Many studies were subsidized and heavily promoted by both the fish industry and the supplement industry. Mainly derived from observations that many long-lived populations ate a lot of fish. Then, making the leap, it must be the Omega-3s.
The negative consequences could make you worse off than taking none at all.
Just eat more fish; this is a more proven benefit without the negative consequences.
Look at your supplement list. Do you want to add one more iffy supplement?
My point is that there is insufficient evidence of any benefit to warrant adding it to my supplement list, especially since the consequences could be detrimental to my aging brain if the “good” studies turn out to be wrong.
Here’s ChatGPT 5.5 Thinking Extended Deep Research. It took 58 minutes and 401 searches to output the result. I specifically mentioned the studies you listed @Shady. I mentioned others on the “anti-omega 3” side but I forgot VITAL-DEP and PreventE4 (I later mentioned them). Still, the conclusion is roughly aligned with what I said: ChatGPT - Omega-3 and Mental Health
Bottom line: EPA may have a niche role in depression treatment; DHA/fish oil for cognition or dementia prevention remains unproven.
For a supplement that is so hyped and has been studied for years, if not decades, this shows it’s useless.
@zebit0 I also don’t eat fish (and am apoe3/4), so I’m forever feeling overwhelmed re this topic. Based on all of Adssx’ good work, if I ate fish, I don’t think I’d even supplement at this point….but I don’t, so as you suggest, I suppose the omega index should be our guide (me guessing).
In his recent omega YouTube, Brad Stanfield mentioned the issue with oxidation and how it causes harm. I asked Claude Opus and ‘he’ said algae oil is much less likely to oxidize. But having said that, there is only one source of epa only algae oil… so here I stand between a rock and hard place.
I did start taking Accentrate LPC which is fish oil, but I’ve since learned it is not a slam dunk, so I’m not sure I’ll repurchase.
Continuing your ChatGPT session (thanks for the link) specifically for those like @Beth and me who do not eat fish, came up with the following:
People who do not eat fish usually have much lower blood levels of the long-chain omega-3s EPA and DHA, because conversion from plant omega-3 (ALA from flax/chia/walnuts) into DHA is inefficient. The main rationale for supplementation is therefore nutritional replacement and normalization of omega-3 status — not proven cognitive enhancement. Studies consistently show vegetarians and especially vegans have substantially lower EPA/DHA levels than omnivores.
For most non–fish eaters without depression, the most reasonable approach is a mixed EPA+DHA supplement (often algae-based), typically ~250–500 mg/day combined. A DHA-dominant mix (for example ~2:1 DHA:EPA) is biologically plausible because DHA is the major structural omega-3 in the brain and retina, and dietary DHA is otherwise nearly absent without seafood. EPA-heavy formulas are more relevant to depression treatment, where meta-analyses suggest modest benefit mainly from EPA-predominant products.
However, evidence for cognitive or dementia prevention remains weak. The recent PreventE4 randomized trial gave high-dose DHA (2 g/day) to cognitively healthy adults at elevated Alzheimer’s risk. DHA clearly increased cerebrospinal-fluid DHA biomarkers, showing brain target engagement, but did not improve cognition or brain imaging outcomes over 24 months.
The PreventE4 trial specifically looked at people with “low dietary DHA intake (<200 mg/day)”. And even in those people DHA supplementation failed to move the needle! So even for people who don’t eat a lot of fish, the case for omega 3 supplementation is weak (or most likely non-existant).
I don’t pay much attention to Norwitz, but given that he is in his early 30s, supplements with DHA-rich foods (e.g…sardines), and has two copies of APOE4, perhaps his reasoning is that one has to start many years before Alzheimer’s symptoms typically appear in APOE4 carriers – as the effects of Omega-3 supplementation are gradual and it’s too late if one waits to start later in life.
I personally am more interested in seeing the results of clinical trials on the effects of choline on APOE4 carriers (that is being carried out by people from MIT, as I recall).
Yassine’s commentary on the study would disagree with you. He stated that improvements in DHA status showed cognitive improvements in the DHA and placebo group in apoE4 carriers. Naturally DHA can increase in the placebo group through diet rather than supplementation. Nice that correlated with improvement. I also posted that previous study that showed improvements in brain structure/function with DHA. Only a 2 year study. Lifetime adequate levels may have larger effect. Hard to think of a mechanism that would benefit APOE4 and harm everyone else but I’m sure you’ll find something.
I have come to believe that there are very very “free lunches” in biology - i.e. where you can get some sort of benefits without any corresponding harm.
Most things are trade-offs. Inflammation is bad, except for all the times when it’s actually important. Oxidative stress is bad, except for the functioning of your immune system. Living in a city is bad (pollution etc) except when it’s good (rapid access to hospitals).
So with fish oil, just looking from principles and not even thinking about studies, I can’t really see strong logic supporting mega-dosing in healthy people as some sort of preventative measure. To believe that means you believe that fish oil/omega-3/DHA/EPA is some sort of “super fuel” where you provide more and it’s beneficial. Or that everybody is somehow deficient and it needs to be corrected. However, we have documented harms of high doses, such as atrial fibrillation.
On the other hand, there are studies out there showing positive data. The PISCES trial reports results that would seem like total bullshit if they weren’t published in NEJM (Hazard ratios in the 0.5 to 0.6 range). So clearly, DHA+EPA supplementation is at least bioactive and does something.
Lastly, there are huge conflicts of interest in this field. Bill Harris is one of the main guys, and the whole omega-3 index thing is his baby. So Rhonda and others are his disciples and help spread his message.
So for me personally (and otherwise healthy person, some CVD risk, and very very low baseline fish consumption), I take 1g per day. I go for a high-quality supplement (Nordic Naturals), and I store it in the freezer. This is basically a “cover the bases” logic so that, in theory, I do not end up deficient. However, I don’t expect this dose to provide any measurable benefit, but I also don’t expect it will cause harm. I would feel uncomfortable not taking any fish oil, since I would be consuming very little marine omega 3 (seafood allergy), but I also wouldn’t increase the dose due to the known risks.
With the current evidence, that’s pretty much the best I can do.
“daily supplementation with fish oil (4 g of n−3 polyunsaturated fatty acids [1.6 g of EPA and 0.8 g of DHA])”
“The rate of the extended primary end point that included noncardiac causes of death appeared to be lower in the fish-oil group than in the placebo group, with a hazard ratio of 0.77 (95% CI, 0.65 to 0.90).”
It’s among “adult patients receiving maintenance hemodialysis”, though. That’s a very specific population. Can we generalize to the overall healthy population?
The shift in the fatty acid composition of the circulating lipidome in Alzheimer’s disease 2024: “Higher levels of docosahexaenoic acid in plasma were associated with a greater rate of MCI-to-AD progression.” (of course, could only be due to disruption in the transport of DHA from plasma to CSF / deficiency in DHA transporters across the BBB but still a risk)
A total of 24 articles met the inclusion criteria. In 5 of the 24 studies reviewed, supplementation with n-3 PUFAs improved cognition. All four trials in persons with AD reported null outcomes. Most of the n-3 PUFA studies in cognitively normal individuals or participants with mild cognitive impairment were null, not powered to detect small effect sizes, or selected participants without dementia risk factors.
We recommend that newer n-3 PUFA supplement trials targeting AD prevention be personalized. For the general population, the null hypothesis appears to be correct, and future interventions are needed to identify and test dietary patterns that include PUFA-rich food rather than supplements.
On Twitter/X as of Dec 2024, he was still recommending 1 mg/day of a mix of EPA + DHA + DPA (interestingly, not DHA only!) but he did not answer my questions and left Twitter altogether: https://x.com/ADssx/status/1904659149750702156
2y is long for a trial. And even imaging did not find anything.
What kind of evidence would be needed for you to change your mind? For me, it’s easy: Mendelian randomization + high-quality RCT showing benefits. We kind of have that for EPA-only supplementation for depression + in people with high Tg.
Crazy results, right? Often with supplements, one of my first questions is whether it actually does anything. But at least for fish oil, we do have these very high quality trials showing biological effects at doses that are feasible for us to take.
But you’re right, I don’t think the PISCES findings can generalise to the otherwise healthy population who is trying to prevent disease. (That was kind of my point that most of these trials are in sick people, not healthy people trying to "optimise). I work closely with a nephrologist, and we chatted about the PISCES trial and he said the results are incredibly impressive, but you have to remember that these are very sick people. We also both noted the curve for serious cardiovascular events (Figure 1A) start to diverge almost immediately after commencing treatment. After only 3 months you can see the two lines and confidence limits clearly separate. That’s pretty interesting, telling us that there is some sort of potent effect which happens very quickly. If you look at Fig 1B, the event-free survival curves also separate relatively quickly, with the biggest uptick between 1.0 and 1.5 years.
And hey, at least the placebo wasn’t literally harmful like in some previous studies haha!
1g per day of EPA? DHA? Mix?
The exact product I take is Nordic Natural ProOmega 2000. But I take 1 capsule, which would mean:
1,075mg total
562mg EPA
438mg DHA
In triglyceride form, which supposedly is better.
I was aware of all of them, thanks to your previous posts. However, I just can’t really make any sensible evidence-based decisions here, based on how I can interpret these studies and relate them to my own circumstances. So I come to my personal viewpoint which is that I don’t eat any seafood and I do believe that omega-3s are something we should consume. I do have some CVD risk, thanks to genetic factors and high Lp(a). However, I am not mega dosing or going for 'optimisation" etc. I reckon 1g per day is enough to do something, but not too much to do too much, haha. Not very scientific I fully admit. My aim is to cover bases and try to avoid any sort of deficiency. I also take my fat-soluble astaxanthin and vitamin D at the same time.
That’s a very good point: we do have trials showing massive benefits in some populations (PISCES EPA-dominant in hemodialysis, and REDUCE-IT, JELIS, and EVAPORATE for EPA-only in high Tg).
I agree with your reasoning. My only question is: why DHA? I dug a bit more and can’t see any benefits to DHA supplementation. Here are more recent papers, all of relatively good quality, and they all point to DHA being useless or even detrimental (as adding DHA to EPA blunts the benefits, and the plasma EPA/DHA ratio seems to matter):
Both dietary and blood levels of n-3 FAs are negatively associated with RDW in individuals with prior MI. The findings are consistent with the hypothesis that RDW may play a potential mediating role in the association between n-3 FAs and mortality risk. Given that a high RDW signifies an inflammatory state and abnormal erythrocyte function, the observed association between higher blood levels of n-3 FAs and improved prognosis after MI aligns with potential underlying mechanisms: attenuated inflammation and enhanced erythrocyte function.
Our findings suggest that n-3 FAs may confer cardiovascular protection, although recent large-scale trials have yielded conflicting results [9,10,11]. Notably, unlike EPA, DHA has been hypothesized to lack cardiovascular benefits—or even to attenuate the protective effects of EPA [38]. Consistent with this hypothesis, our mediation analyses indicated that EPA-specific biomarker (eEPAp) accounted for a larger proportion of the association with clinical outcomes than DHA-related biomarkers, potentially explaining the inconsistent evidence across studies, which often differ in their EPA-to-DHA ratios. Although the EPA-to-DHA ratio (EDR)—a measure of their relative abundance—was not statistically significant in our analysis, it showed a consistent inverse association with mortality. This aligns with emerging evidence suggesting that the EPA:DHA balance, rather than absolute levels alone, may influence cardiovascular risk. Intriguingly, all participants exhibited low EDR values, indicating a population-level relative deficiency of EPA compared with DHA. Whether selectively increasing EDR through EPA-predominant supplementation confers additional clinical benefit remains an open question warranting focused investigation.
(poke @John_Hemming, above paper on RDW, you might be interested)
EPA showed a significant inverse association (OR 0·907, 95 % CI 0·824, 0·998, P = 0·045); ALA, DPA and DHA were NS. […] Dietary n-3 intake, particularly EPA, was modestly and inversely associated with depression severity.
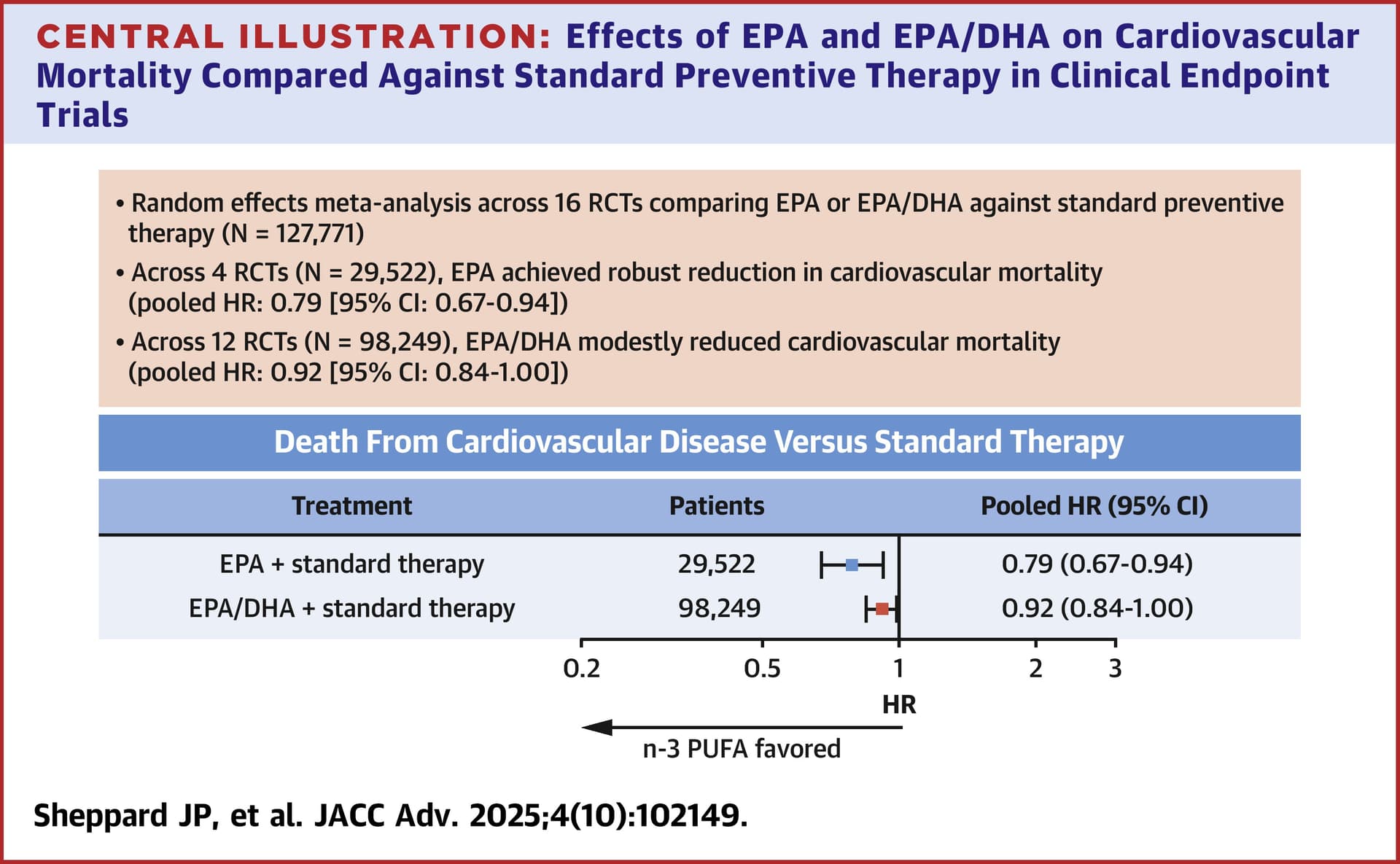
EPA lowered incident CVD-attributable mortality in RCTs investigating its use for primary or secondary CVD prevention. Relative to EPA, benefits reported with EPA/DHA were attenuated. Although more work is needed to understand these differences, EPA should preferentially be used in cardiovascular conditions for which it is indicated.
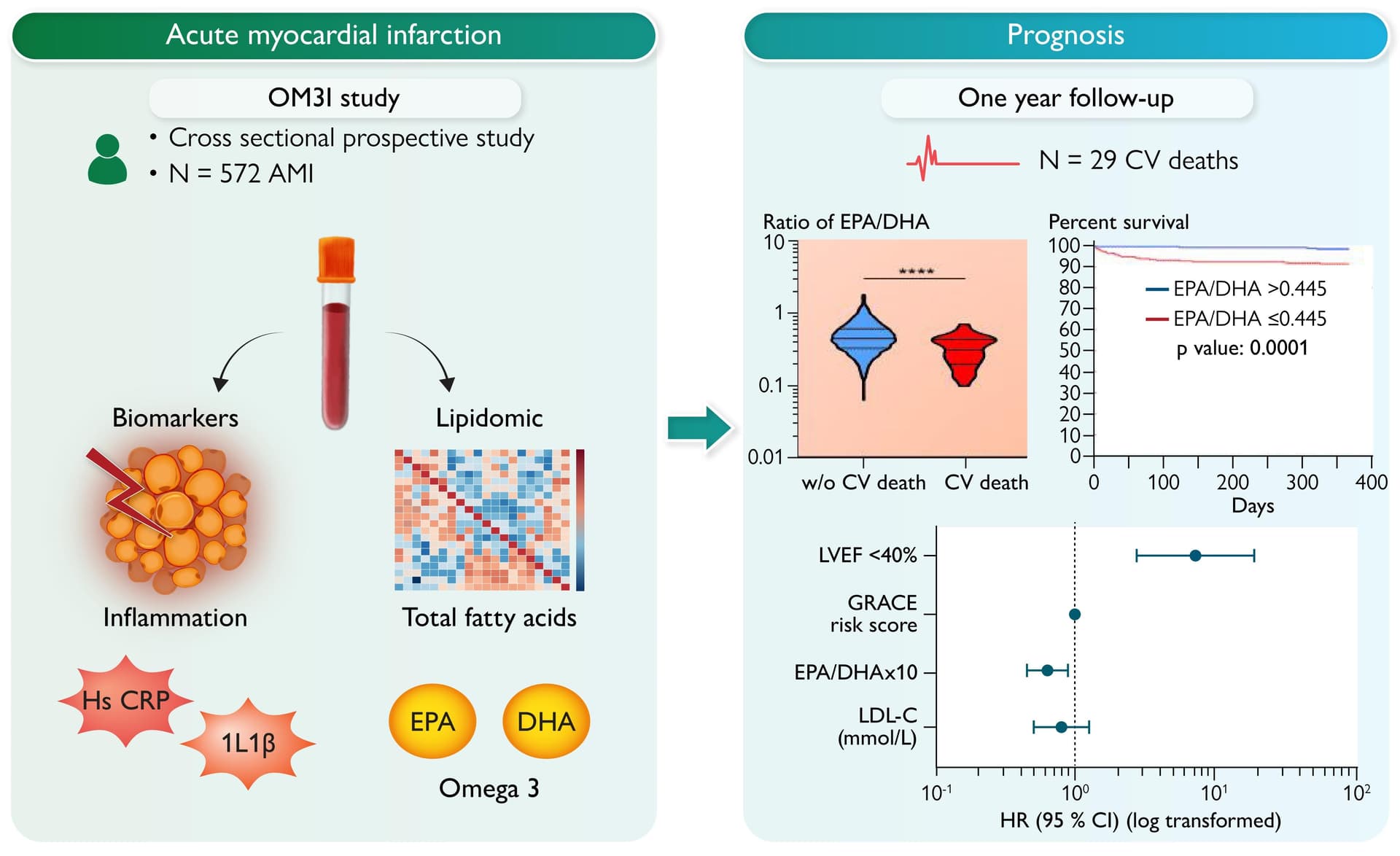
Patients who died had lower relative levels of EPA [0.47% (0.28–0.73) vs. 0.73% (0.52–1.02), P < 0.001], a lower EPA/DHA ratio [0.33 (0.22–0.43) vs. 0.44 (0.33–0.61), P < 0.001], and more elevated levels of inflammatory biomarkers, including hs-CRP and interleukin-1β. In contrast, DHA levels were not associated with CV mortality. In multivariate analysis, the EPA/DHA ratio was associated with lower CV mortality, even after adjustment for confounding factors including GRACE risk score, left ventricular ejection fraction, and inflammatory biomarkers.
So, is there a case for supplementing with DHA in 2026? For depression, the answer is a clear no to me (VITAL-DEP EPA+DHA showed increased depression, while EPA-only showed benefits). For CVD, EPA-only seems better. Even PISCES was 2:1; maybe EPA-only would find even better outcomes! And, for cognitive health, after PreventE4, it’s very hard to make a case for DHA supplementation as PreventE4 was the perfect trial design recommended by “pro fish oil” people: DHA only, high dose, long duration, fairly large trial, with vitamin B, in a population with low baseline, with imaging + cognitive measurements, etc.
Thank you for all of your analysis. I have decided to switch from 2:1 EPA/DHA to EPA only. The main reason I take it is to reduce triglycerides, which I have found to have a noticeable effect.