The landscape of metabolic optimization and glycemic control is shifting from peptide-based injectables toward small-molecule oral therapeutics. The ACHIEVE-3 phase 3 clinical trial provides the first direct, head-to-head comparison of two oral glucagon-like peptide-1 (GLP-1) receptor agonists: the novel non-peptide orforglipron and the peptide-based oral semaglutide. The trial enrolled 1698 adults with type 2 diabetes who were inadequately controlled on metformin, testing 52-week outcomes across four arms (12 mg and 36 mg orforglipron versus 7 mg and 14 mg semaglutide).
The primary findings indicate that orforglipron is both non-inferior and superior to semaglutide for glycemic control. At 52 weeks, orforglipron (36 mg) reduced HbA1c by 1.91%, compared to a 1.47% reduction with semaglutide (14 mg). Furthermore, 31% of participants on the 36 mg orforglipron dose achieved near-normoglycemia (HbA1c < 5.7%) compared to only 12% on the highest semaglutide dose.
Beyond glycemic control, orforglipron demonstrated superior efficacy in weight reduction. Participants on 36 mg of orforglipron achieved an 8.2% reduction in body weight, significantly outperforming the 5.3% reduction observed with 14 mg of semaglutide.
However, enhanced efficacy comes with a trade-off in tolerability. Gastrointestinal adverse events were more frequent in the orforglipron cohorts (58-59%) compared to semaglutide (37-45%), driving higher treatment discontinuation rates. Additionally, orforglipron induced a greater mean increase in resting pulse rate (up to 4.7 bpm) compared to semaglutide (up to 1.5 bpm). Ultimately, orforglipron eliminates the strict fasting and fluid restrictions required by oral semaglutide, presenting a highly efficacious, practical, and potent metabolic intervention, provided individuals can navigate the gastrointestinal onboarding phase
Institution: University of Texas Southwestern Medical Center (lead author affiliation), alongside a multinational cohort of 131 medical research centers.
Country: Multinational (Argentina, China, Japan, Mexico, and the USA).
Journal Name:The Lancet. Published: January 17, 2026 Impact Evaluation: The impact score of this journal is 168.9, evaluated against a typical high-end range of 0–60+ for top general science, therefore this is a Elite impact journal.
Target Pharmacology: Orforglipron is a small-molecule, non-peptide partial GLP-1 receptor agonist.
Pathway Bias: It is biased toward G-protein activation over β-arrestin recruitment. This bias may alter receptor internalization dynamics compared to endogenous GLP-1 or peptide mimetics, potentially driving sustained signaling [Confidence: Medium].
Longevity Pathway Implications: By driving significant weight loss (up to 8.2%) and lowering fasting serum glucose, orforglipron effectively acts as a potent caloric restriction mimetic. The resulting metabolic state indirectly downregulates the nutrient-sensing mTOR pathway and upregulates AMPK, promoting autophagy and improving mitochondrial dynamics [Confidence: Medium].
Organ-Specific Priorities: The primary therapeutic impact is systemic metabolic normalization, targeting hepatic lipid accumulation, pancreatic β-cell preservation, and visceral adiposity reduction. The observed reductions in non-HDL cholesterol, triglycerides, and VLDL cholesterol indicate an optimized cardiovascular and hepatic profile
Novelty
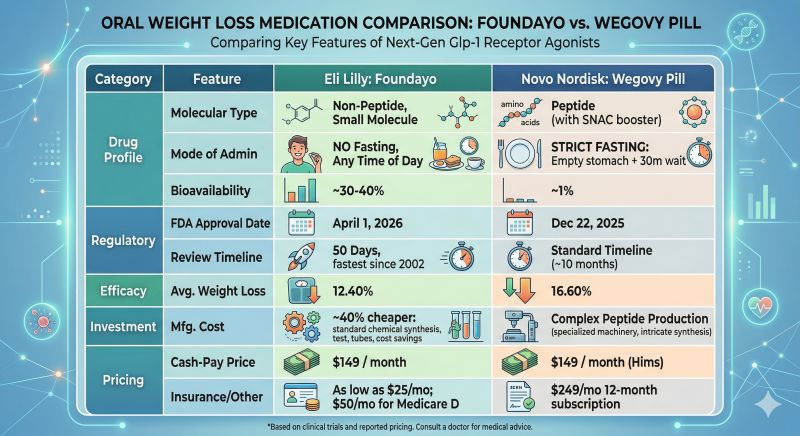
Administration Practicality: Unlike oral semaglutide, which requires fasting administration with ≤120 mL of water at least 30 minutes prior to food or other medications due to ~1% bioavailability, orforglipron has no dietary or fluid restrictions. This practical advantage significantly lowers the barrier to adherence [Confidence: High].
Efficacy Ceiling: This paper proves that a non-peptide oral agonist can safely surpass the efficacy of current approved oral peptide mimetics in both glycemic control and weight reduction.
Critical Limitations
Methodological Weaknesses: The trial utilized an open-label design. While laboratory values (HbA1c) are objective, patient-reported outcomes, adverse event reporting, and study dropouts are highly susceptible to placebo/nocebo effects when treatment assignments are known [Confidence: High].
Tolerability and Dropout Bias: The discontinuation rate due to adverse events was approximately double in the orforglipron arms (9-10%) compared to the semaglutide arms (4-5%). This high attrition rate indicates that the superior efficacy observed in the intention-to-treat analysis may be limited in real-world settings by gastrointestinal intolerance [Confidence: High].
Cardiovascular Uncertainty: Orforglipron elevated the mean resting pulse rate by up to 4.7 bpm, compared to 1.5 bpm for semaglutide. While a known GLP-1RA class effect, this exaggerated chronotropic response requires rigorous, long-term cardiovascular outcome data to confirm it does not offset the metabolic benefits [Confidence: High]. Long-term cardiovascular safety data remains missing from this 52-week trial
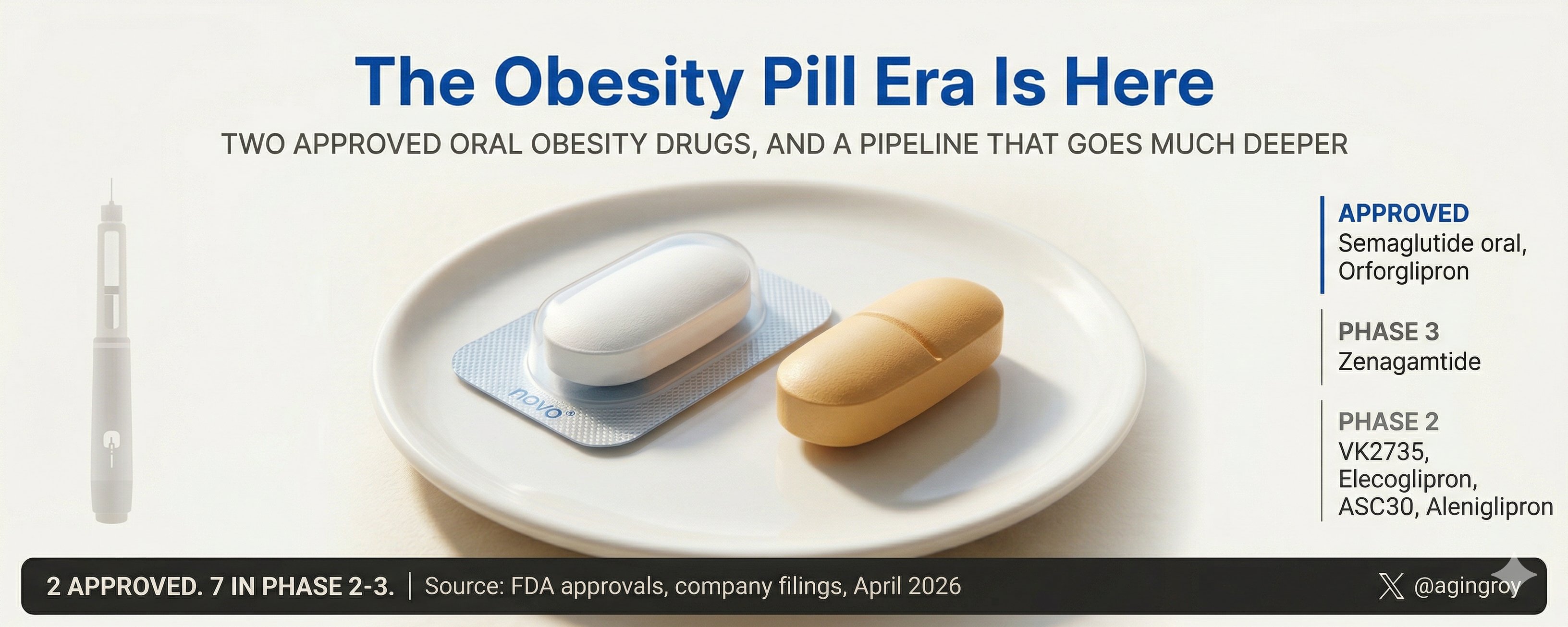
April 1 (Reuters) - The U.S. Food and Drug Administration on Wednesday approved Eli Lilly’s (LLY.N), opens new tab weight-loss pill, making it the second to market after Novo Nordisk’s (NOVOb.CO), opens new tab oral Wegovy, as the companies fight to capture more customers with the convenience of pills over injectables.
The Lilly drug, orforglipron, which will be sold under the brand name Foundayo, is a once-daily oral medication designed to mimic the appetite-suppressing GLP-1 hormone targeted by the company’s blockbuster injection tirzepatide, sold as Mounjaro for diabetes and Zepbound for weight loss.
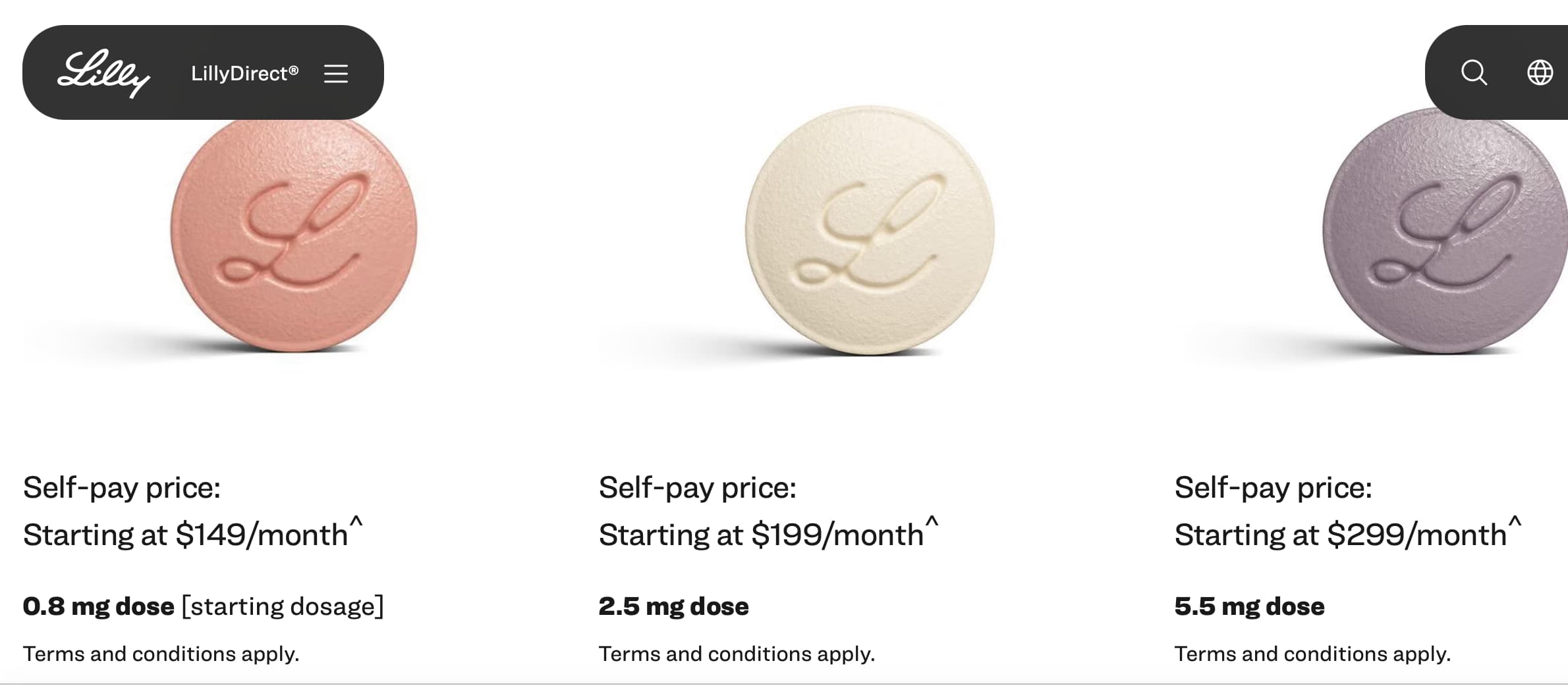
Lilly said the drug will be available for shipping beginning April 6 through its LillyDirect program and cost $149 per month for the lowest dose for self-pay customers, on par with Novo’s pill. Soon after, it will be available through retail pharmacies and telehealth providers, the Indianapolis-based company said.
The ATTAIN-MAINTAIN study has some numbers on that. On average, those who switched from semaglutide regained only about 2 lbs, and those switching from tirzepatide regained approximately 11 lbs, after switching to orforglipron for maintenance.
Notes :
People lost more on tirzepatide, 50 lbs on tirzepatide vs 33lbs on semaglutide. So to me, semaglutide users could be more incentivized to switch since weight gain is minimal.
fair to say that if patients had stayed on their initial medication, they would have kept their original weight loss, and not gained back 11 lbs for switching away from tirzepatide.
Just a quick comment - this study used Rybelsus dosing for comparison rather than oral Wegovy dosing. In other words, they used 14mg instead of 25mg. So not surprising it was better and had more side effects.
I think oral Wegovy is pretty decent and will be even cheaper from India over the next few months. Sub $100 a month is a game changer for people. Yes, for some, the 30 min fast in the AM is a big barrier but money is a bigger barrier for most.
I worry about crackdowns from India because of cheap semaglutide.
I could see them cracking down on the US-based vendors selling it, but the amount of cargo that moves through the ports is so vast that I don’t they could realistically stop the bootleg GLPs even if they wanted to. They can’t even keep stuff like fentanyl from being shipped. Even trying would require a huge amount of resources devoted to it, and what politician is going to want to piss off the overweight part of the population by forcing them to to either stay overweight or pay thousands of dollars a year in perpetuity for the Eli Lilly-manufactured stuff?