This is a interesting article about Lp(a) lowering drugs;
I have just began a 3 month personal experiment to see if taking 400mg bezafibrate daily decreases my Lp(a)
This is a interesting article about Lp(a) lowering drugs;
I have just began a 3 month personal experiment to see if taking 400mg bezafibrate daily decreases my Lp(a)
Please let me know how it pans out, I would be very interested to know ![]()
Ok, I will post an update here in 3 months ![]()
That was a very useful article, thank you. I look forward to hearing your progress report.
Gemfibrozil, mentioned in the same paragraph as bezafibrate, is believed to have anti-aging potential according to Brian Kennedy.
In the small study referenced to, three of eight patients got an lp(a) reduction of at least 33 % with gemfibrozil.
I now, that’s why I’m so interested in it ![]()
I already use Pioglitazone, a stimulator of PPAR gamma, which is currently been tested in ITP. It’s also one of the drugs I used to work with.
Interesting, do you also use metformin or acarbose? I already use acarbose but would consider to add pioglitazone to my daily stack
Yes, I use both metformin and acarbose alongside pioglitazone. I take 2.125g of immediate release metformin ![]() (that one surprised me) and 200mg of acarbose, both are spread out around meal times (also take metformin dose last thing before bed).
(that one surprised me) and 200mg of acarbose, both are spread out around meal times (also take metformin dose last thing before bed).
The dose of pioglitazone I use is 7.5mgs, I know it’s a low dose, but imo it’s a good drug for diabetes but has its problems, hence the low dose. There is literature precedence for that dose, see below.
Whether I continue with may depend on the results from the ITP study.
Any more color on the part bolded above?
There is a short video clip on you tube Brian Kennedy AKG and gemfibrozil 2 promising geroprotectors for slowing aging
And a longer video clip posted by Rapadmin in a thread on Gemfibrozil started by him in January. There is good info there.
No published data on humans yet. A bunch of animal studies.
Combined with a possible lpa lowering, I find gemfibrozil attractive and will start it
Headache, rash and fatigue 1 - 10 %.
Rarer, more serious side effects.
Dont use together with statins and loperamide. Ok with ezetimibe except if you have tendency for gall stones. As far as I know.
Thanks Ulf. Do keep us posted, including on if it impacts your Lp(a).
For most people, keeping their BMI low and exercising will keep their lipids in the good range.
I was just taking one atorvastatin 40 mg tablet in the evening.
I no longer pay extra to have Lipoprotein(a) because it always comes back below the limit my lab measures.
Unless I see something untoward in my regular measurements, I won’t pay for the additional tests. I am sure that with me it is a genetic factor that causes it to be so low.
Because I eat a lot of steaks, eggs, whole milk, etc, I recently added Ezitimibe in the evening and Pantethine in the morning. I am not sure I am taking Pantethine at the optimal time, but it seems to be working.
For the past several weeks I have been taking 4mg of rapamycin with GFJ every week. Before that, I was taking 3 mg with GFJ
I just received these results today:
@desertshores Does ezetemibe give you an energy boost? I couldn’t take it at night as it kept me from falling asleep!
I have noticed no effects from taking ezetimibe other than it has improved my lipid results.
“There is no specific time of the day that is best to take ezetimibe, as it works exactly the same whether you take in the morning, afternoon or at night. Ezetimibe is taken once a day, at the same time each day and it can be taken with or without food.”
I just assumed that I would take it with my statin which my doctor prescribed as an evening dose.
So, each of us sometimes has our own personal side effects.
One I discovered, which maybe only affects me, is magnesium citrate. I took some before bedtime for a couple of days and it made me get up several times during the night to go pee.
I didn’t see this side effect listed in any of the papers on magnesium citrate that I read.
Sure. Will start it end of next month.
Plasma concentrations of Lp(a) are predominantly genetically determined, they are relatively stable over a lifetime. Therefore, Lp(a) may only need to be measured once. Repeated measurements would only make sense if you are taking interventions to lower Lp(a) and want to check the effect.
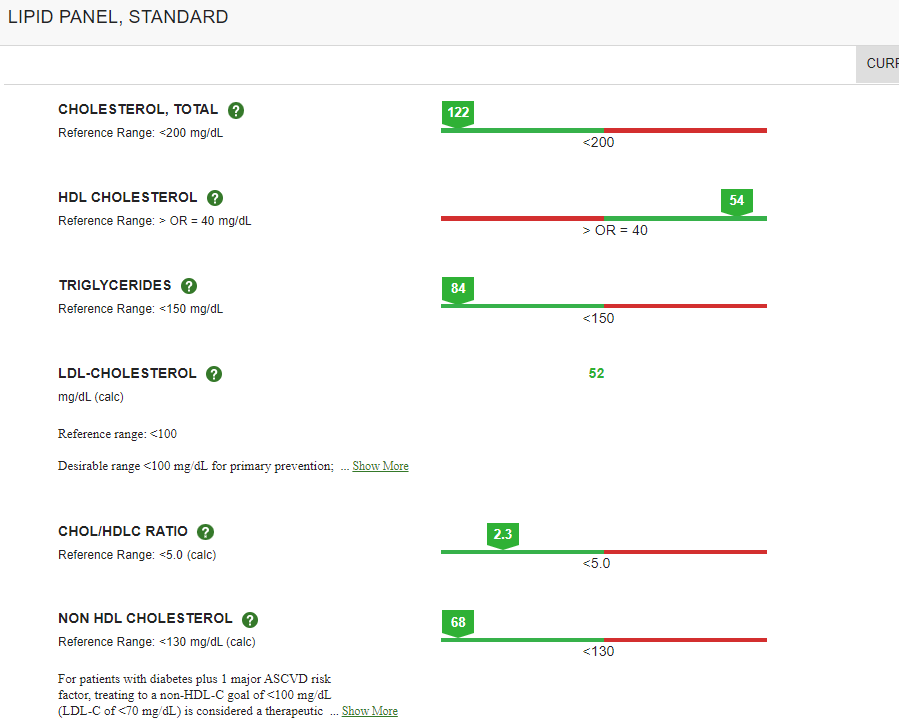
Correct, Lp(a) concentrations are predominantly gentically determined. I am other wise very healthy, but have bad genes for cardiovascular health; I have genetic cardiomyopathy and I have an Lp(a) of 96 mg/dL (normal is < 30). That’s why I follow Peter Attia’s recommendations for cardiovascular health and I do 3h of zone 2 per week and I keep my LDL cholesterol low. I take 10mg ezetimib every day and 10mg rosuvastatin every third day. My LDL is 54 mg/dL and total cholesterol 113 mg/dL. From 17 novembre on I started taking 400mg bezafibrate daily and with get my blood checked again around 17 february
Great results for my Lp(a) from adding daily 400mg bezafibrate from 16 november to 16 februari;
Lp(a) dropped from 96 mg/dL to 54 mg/dL, so a 43% reduction. Didn’t expect that at all
Excellent reduction, right at the high end of the reduction range noted in the Greek paper.
What is the name/brand/source of the Bezafibrate that you take? When I search on Indiamart, nothing readily comes up.