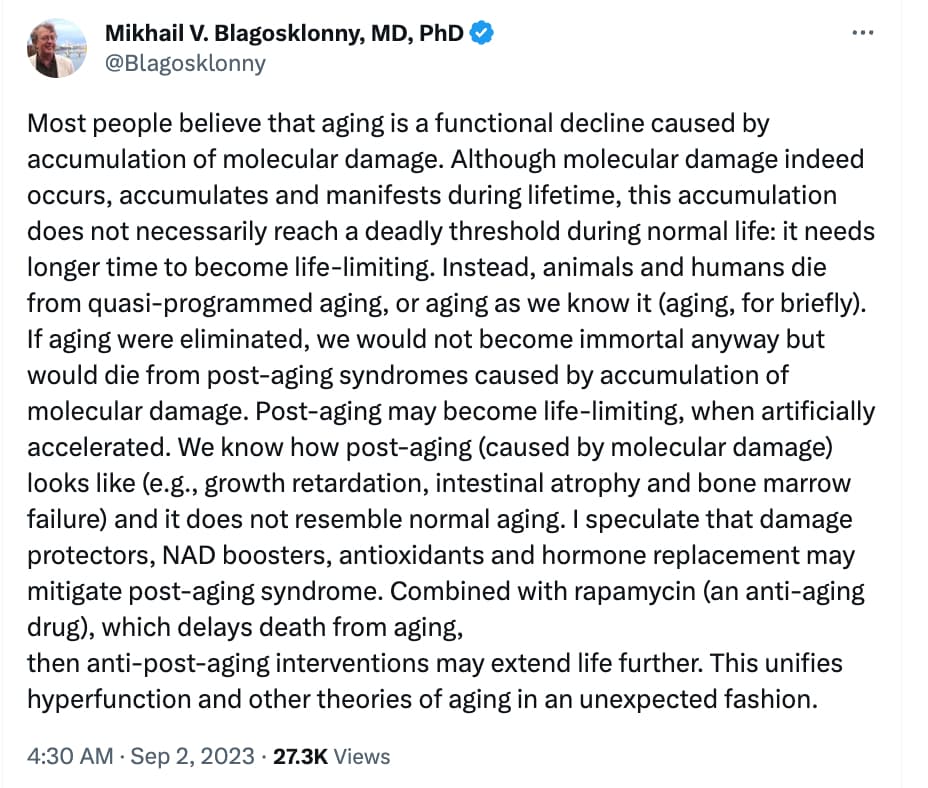
Essentially that aging is driven by mTor, but accumulated damage (what he calls “post-aging”) is actually real and would eventually become a separate problem if it weren’t for the fact that aging kills us first.
3 Likes
Any theory of aging needs to fit the known facts and have a mechanism (or mechanisms). The mechanism for mTOR AFAICS relates to mitochondrial efficiency. I dont see the linked post identifying an actual mechanism that drives the aging phenotype. Hence i see no reason why his conclusions should be valid.
2 Likes
It’s very similar to what reprogramming people say… Do Peter Fedichev’s theories (of 150 years) fit in with post-aging? My guess is not exactly, but it is somewhat in that direction
Is post-aging what supercentenarians die of? They are more resistant to “quasi-programmed aging” (often because they do have some special genetic program in them that resists damage despite many of them being smokers), though not maximally resistant to it.
I don’t think he’s right on all the details. Hormone replacement is more important for “quasi-programmed aging”. Anti-glycative/crosslinking agents (and damage clearance/slowdown [eg getting exosomes to extrude out damaged proteins before they become an issue]) is more important for post-aging syndrome.
Smoker supercentenarians is the group we have to test these hypotheses on
2 Likes
How would this theory separate the accumulation of damage issue (post aging?) from the deterioration of repair function caused by excessive growth mode and insufficient autophagy mode…that leads to accelerated accumulation of damage?
I think it’s just a definition thing. If you were able to stop all damage caused by mtor pathway / growth / hyperfunction… you’d still be slowly accumulating other damages over time. This is just that “other” category.
2 Likes
1 Like