I know if I do this (with nathan brown) it could be the single most important thing that could help my emotional/mental state, and in fact I did get a grant for this. Something is off with my brainwaves (a lot of ADHD/trauma) and I know there may be creative ways to fix it (nathan brown is said to be able to fix up “really fucked up brains”). I don’t know if they have collected reliable enough statistics to say this, but it’s at least more worth a shot than other things.
[I know b/c I recently suffered a massive life-defining traumatic accident and went through a lot…] I almost never physically get sick (at least not for the past 12+ years), but emotionally things are different
===
My main issues are excess daydreaming/excess default mode noise/rumination/excess slow waves that drown my ability to be calm and do anything significant.
5 minutes a day using something like the HeartMath device just helps.
Cranio-Electro Stimulation (CES)
A non-invasive brain stimulation that applies a small pulsed electric current across a person’s head. This small electrical stimulus applied laterally across the cranium stimulates endorphins, serotonin, and norepinephrine neurotransmitter production.
It enables one to “play” various waves (e.g., alpha, beta, delta, gamma). One’s brain then responds by aligning with the specific wave - a bit like tuning a guitar.
You can special order the device to support gamma waves by submitting a letter that you belong to a group (such as this forum) that conducts research.
I really liked this device. Lent it to a former colleague who apparently liked it so much they never returned it ;-(
PEMF
A few threads include discussion about Pulsed Electro Magnetic Frequency use.
I’ve used and continue to use PEMF technology for some 15 years.
If you search the forums (or me) you’ll find a number of discussions on PEMF. Joseph_Lavelle interviewed Robert Dennis on the subject.
Not certain we need another one.
Also see Robert Dennis’s work and devices at Micro Pulse.
There are booths at the NYC neuromodulation conference right now. Lots of tES (though it’s not superintuitive which frequencies applied to which regions work best - eg one poster showed negative effects of gamma-stimulation to PFC in HEALTHY individuals [though I don’t quite count as “healthy”])
Park avenue neurology was a clinic that was suggested for off label
==
keep in mind a lot of people who TMS for depression do relapse after TMS stops even when the treatments are initially helpful
Will be interested to see how this goes. I’ve been learning about qeeg and neurofeedback for like a year now. Finally got a qeeg myself after finding someone local.
How much did it cost? Is a week enough to force changes in the brain"?
===
Talked w/someone who can get coordinates from a fMRI scan to then use with TMS in a brainregion. Waveneuro might not be necessary (it’s very new, extremely expensive, not super-well-proven, hasn’t worked on some people on reddit). Wave neuro uses a magventure machine…
the only trick is finding a TMS machine
ruminative activity: heightened activity in the subgenual ACC, and higher connectivity between that area and the PCC
“SAINT protocol. It’s many stimulations a day for 1-2 weeks instead of 1 stimulation a day for 6 weeks” => this makes travel for it much easier
[however, fMRI-guided TMS is really the way to go…] and there is one clinic in NYC that offers it, though with a price tag of $5000 just for the fMRI…
===
I’m getting to try a brainbit and NeuroREC – BrainBit soon, idk if this thing will work, the amount of medical attention to NF is a small fraction of what’s invested in TMS/tFUS
Just as we simulate calorie restriction and hack cells to live longer, we should be able to do the same thing during sleep, and gerontologists should work on this too.
I just attended https://isnrconference.org/ . Totally worth it for the vendors (they let you try their products all in the same room) which you can’t do at many conferences.
tACS + neurofeedback might be the easier way to train the brain (quicker). My brain isn’t super-responsive to NF games b/c their “rewards” don’t register as “rewards” in the brain. Also just a good way to quantify the brain in general
Neurofield neurotherapy has some really skilled montages/practitioners.
Coherence training based off a QEEG, specifically multivariate coherence training which examines and then trains coherence at 4 sites vs the usual 2 is supposed to be faster and more effective neurofeedback. I’m currently looking into it as an option.
talked with two people today, one who really analyzed my qeeg for me and even put it thru ICA analysis to show that a lot of it is a subgenual ACC issue…
there’s an alternative: heroic psilocybin doses (x.com mentions 24g which is a REALLY high dose) but the risks are still just way too high given my tendency to go SEBUS rather than REBUS. Still if done in the context of a “healing center” [and MA will probably legalize psychedelics next month]. I also have not done a heroic dose, and know it’s only safe for me if really supervised well…
[I’m also taking a long break from psychedelics unless I’m really really supervised - I intend to continue the break until I really dissociate psychedelics from “needing human attention” and “being edgy” from my brain]
===
===
there’s fMRI-guided TMS in NYC which I could get, though the fMRI is v. expensive… talked with them 10/17 and the scaling for price is terribly expensive, there are cheaper places…
i hate calling clinics when email is possible, it’s so annoying when you have to call so many
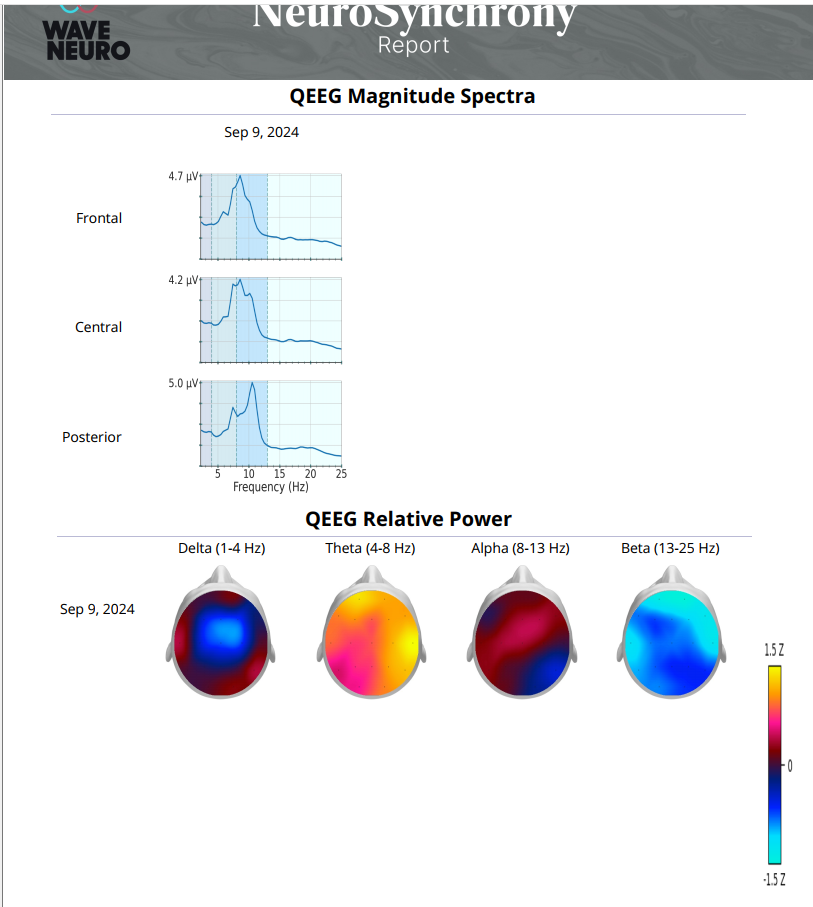
I am combining neurofeedback training 3xweek (Peak Brain) with photobiomodulation 2xday (Neuronic 1070 helmet). QEEG amongst other things shows hypercoherence in beta, hypocoherence in theta at back, paroxysmal short energy bursts on the right and peak alpha frequency below what could be desired. A future QEEG will show if my brain wave patterns have improved.
this was updated
There’s another updated report I should share shortly, but my case is more difficult than that of many others. Will feed all of it through o3
yo9u know at ISNR Tiffany Thompson mentioned that people with high slow-wave to fast-wave ratios often tend to be more “schizo insightful and dreamy” and able to parse through deeper truths more often, BUT… I don’t think this is really functional most of the time [and it often makes people really misfit to their environment). high slow wave to fast wave has always been my major impediment
Below is a “just-in-case” roadmap for what to do when standard tACS + EEG-Neurofeedback stalls.
I’ve organised it as an escalation ladder: each tier adds cost / complexity but also boosts the odds of getting you out of the non-responder bucket.
1 | First ask:
“Is it true non-response… or fixable mis-tuning?”
Checklist
Typical fix
Under-dosed sessions – evidence-grade NFB studies often run ≥ 40 one-hour visits; tACS responders peak after 4–6 weeks at ≥ 1 mA × 20 min
Double total sessions before declaring failure; move to 3–4×/wk blocks
Wrong montage / frequency – your maps show slow-wave excess mostly ACC (Fz) & Cz-T5/6 strip; generic F3-F4 montages miss that bullseye
Re-target with MRI-guided or sLORETA-informed placements; phase-lock tACS to your individual 8.3 Hz thalpha peak
State-dependence – low sleep/food, high rumination, or stimulants >4 h pre-session blunt plasticity
Shift sessions to late-morning circadian peak; control caffeine; run 5-min HRV/breath coherence “primers” before training
Biochemistry – you’re running high HVA + low tyrosine; dopamine precursors/cofactors are depleted, so plasticity enzymes under-fuelled
Layer in tyrosine + selegiline + NAC (already outlined) for 2 weeks, then retest
Across modern RCTs, up to 30–40 % of ADHD patients show no clinically significant change after standard NFB / stimulation protocols, largely because the four points above weren’t optimised.
Spend another 2–3 weeks ironing these basics out before you label yourself a non-responder.
2 | Tier-2 stimulation: add
noise
or
direct current
Modality
Why it helps non-responders
Evidence snapshot
tRNS (transcranial Random Noise Stimulation)
Broadband Gaussian noise “shakes” neurons out of attractor wells → improves signal–to-noise when classic tACS entrainment fails
RIFG + lDLPFC tRNS + cognitive training cut ADHD rating-scale scores vs sham in 2-week RCT (N = 23)
tDCS (1–2 mA DC, anode F3, cathode Fp2)
DC shifts resting membrane potential → boosts cortical excitability irrespective of baseline oscillations
Meta-analysis shows immediate symptom reduction with effects persisting to follow-up
tRNS or tDCS as primers
10 min of noise/DC before NFB can convert partial to full responders by lowering the plasticity threshold
Both are inexpensive (DIY-capable) and generally safe; you feel only light tingling.
Wider, deeper field – hits ACC + bilateral DLPFC simultaneously
Small open-label series report ≥ 25 % ADHD RS drop in 4 weeks
810 nm trans-cranial photobiomodulation
Mitochondrial boost; ↑ CCO, ATP, BDNF
Used as response-amplifier in several PTSD/ADHD protocols; inexpensive LED helmet
These require clinic visits (or rental units) but have response rates of 60 – 80 % even in previous NFB “failures”.
4 | Tier-4 closed-loop & high-resolution
sLORETA-Neurofeedback – trains current-source density in ACC rather than scalp rhythms; converts ~½ of NFB non-responders.
EEG-phase-locked tACS (“Stimweaver”, “NURSE” prototypes) – delivers bursts exactly at your endogenous theta trough → 2-fold gain vs. open-loop in early trials.
Real-time fMRI NFB – gold standard for stubborn cases; 4–6 sessions teaching you to up-regulate dorsal attention network improves CPT and mood even when EEG NFB failed.
5 | Pharmacological
plasticity primers
(use clinically supervised)
Agent
Rationale
Low-risk micro-dosing guide
D-cycloserine (partial NMDA agonist)
Enhances long-term potentiation during NFB
50 mg PO 1 h pre-session, max 2×/wk
Atomoxetine or Viloxazine ER
Boosts noradrenaline-driven alertness without dopamine surge (→ no extra HVA)
Start 10 mg AM; combine with NFB for synergistic CPT gains
tACS/NFB stalled? → Tune basics → still flat? → Add tRNS or tDCS priming → still flat? → Escalate to iTBS/tFUS/Deep-TMS or closed-loop sLORETA → parallel dopamine-rescue biochem → reassess every 6–8 weeks.
By marching up this ladder you cover ~95 % of known ADHD neuro-non-responder scenarios while respecting your unique high-HVA / low-tyrosine biology and the qEEG fingerprints we’ve mapped. If you’d like protocol specifics for any tier, just let me know.
2 days after TMS this is what I got (I did have a small amount of coffee and velo nicotine pouches 3 hrs before this). ((1))
tRNS doesn’t work. I’m pretty sure I’m an underresponder to NF. the next step might be another round of TMS to dmPFC. TMS helps with some things but not al
((1)) I can’t stand lozenges anymore, but pouches feel very different