I came across this news story from last October, and then decided to investigate more. Results from my efforts below:
The investigational monoclonal antibody trevogrumab was associated with lean mass preservation and greater loss of fat mass in people taking semaglutide, an interim trial data showed.
Findings from Regeneron Pharmaceuticals Inc’s ongoing phase 2 COURAGE trial were presented at European Association for the Study of Diabetes (EASD) 2025 Annual Meeting by Ofri Mosenzon, MD, of the company. The trial also included an arm of another antibody, garetosmab, which was associated with significant side effects.
Both trevogrumab and garetosmab are fully human immunoglobulin G4 monoclonal antibodies developed to block key negative regulators of muscle mass, myostatin, and activin A, respectively.
See this Medscape story: https://www.medscape.com/viewarticle/myostatin-blocker-preserves-muscle-glp-1-treatment-2025a1000qs4
Myostatin Blockers in Development and Testing:
The landscape of myostatin inhibition has bifurcated into two distinct clinical tracks: neuromuscular disease (specifically Spinal Muscular Atrophy - SMA) and cardiometabolic health (specifically “quality weight loss” as an adjunct to GLP-1 agonists).
Below is the status of myostatin blockers currently in development or clinical trials as of early 2026.
Executive Summary of Clinical Status
- Neuromuscular Track: The field has faced significant regulatory and clinical headwinds in late 2025. Scholar Rock’s Apitegromab received a Complete Response Letter (CRL) from the FDA in September 2025, delaying approval. Biohaven’s Taldefgrobep alfa failed its primary endpoint in the Phase 3 RESILIENT trial.
- Metabolic/Longevity Track: This sector is accelerating. Major players (Lilly, Regeneron) are pivoting myostatin inhibitors to be “muscle preservation” agents used alongside Semaglutide or Tirzepatide to prevent sarcopenic obesity.
Active Clinical Pipeline (2025-2026)
| Drug Candidate | Company | Mechanism of Action | Indication | Development Phase / Status |
|---|---|---|---|---|
| Apitegromab (SRK-015) | Scholar Rock | Selective Inhibitor: Binds pro- and latent myostatin (prevents activation). Avoids GDF11/Activin. | SMA (Types 2 & 3) |
Regulatory (CRL): Phase 3 (SAPPHIRE) was successful, but FDA issued a CRL in Sept 2025. Resubmission expected 2026. Phase 2 (OPAL) ongoing for infants. |
| Bimagrumab | Eli Lilly (via Versanis) | ActRII Blocker: Monoclonal antibody against Activin Receptor Type II. Blocks Myostatin + Activin A/B. | Obesity (w/ Semaglutide) | Phase 2b/3 (BELIEVE): Active. Positioning as a “quality weight loss” agent to increase lean mass while cutting fat. |
| Trevogrumab (REGN1033) | Regeneron | GDF-8 mAb: Monoclonal antibody neutralizing myostatin directly. | Obesity (w/ Semaglutide) | Phase 2 (COURAGE): Data released Sept 2025 showing ~50% retention of lean mass when combined with Semaglutide. |
| Taldefgrobep Alfa (BHV-2000) | Biohaven | Adnectin / Ligand Trap: Modified adnectin that binds myostatin and lowers free levels. | SMA; Obesity | Phase 3 (Failed): Missed primary endpoint in RESILIENT trial (SMA) in Aug 2025. Future of program uncertain. |
| GYM329 (Emugrobart) | Roche / Chugai | Sweeping Antibody: “Sweeps” latent myostatin from plasma; recycles antibody. | SMA (w/ Risdiplam) | Phase 2/3 (MANATEE): Recruitment completed. Evaluating efficacy in combination with Risdiplam. |
| SRK-439 | Scholar Rock | Selective Inhibitor: Next-gen selective inhibitor of pro-myostatin (high specificity). | Obesity / Cardiometabolic | Phase 1: Healthy volunteer study ongoing. Topline data expected H2 2026. |
Detailed Analysis of Key Assets
1. Apitegromab (Scholar Rock)
- The Science: Unlike earlier failures (e.g., Pfizer’s Domagrozumab) that targeted mature myostatin (which is structurally similar to GDF11 and Activin), Apitegromab targets the precursor forms (pro- and latent myostatin). This specificity is hypothesized to reduce off-target toxicity (e.g., bleeding events associated with GDF11 inhibition).
- Current Reality: Despite the Phase 3 SAPPHIRE trial meeting its primary endpoint (improvement in HFMSE scores), the FDA’s rejection (CRL) in September 2025 suggests manufacturing or data handling issues rather than pure efficacy failure. The company is remediating for a 2026 resubmission.
2. Bimagrumab (Eli Lilly / Versanis)
- The Science: This is arguably the most potent agent for hypertrophy because it blocks the receptor (ActRII), effectively shutting down signaling from multiple ligands (Myostatin, Activin A, Activin B).
- The Trade-off: Broader inhibition often brings more side effects (muscle cramps, potential cardiovascular signals). Lilly is betting that intermittent dosing or combination with incretins (GLP-1s) will mitigate risks while stripping body fat and adding muscle.
- Relevance to Longevity: This drug mimics the “mighty mouse” phenotype more closely than others but requires careful safety monitoring due to the ActRII blockade.
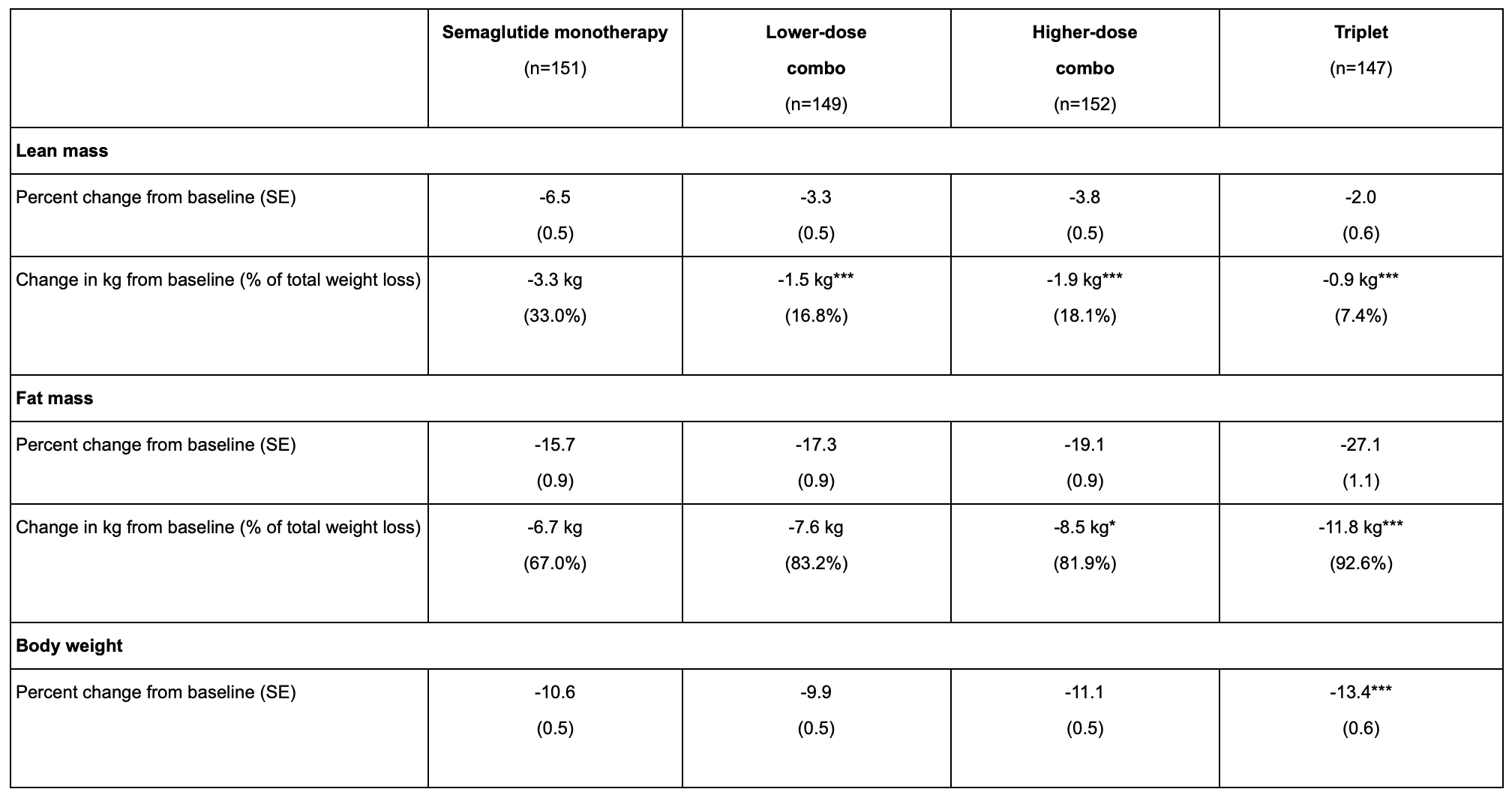
3. Trevogrumab (Regeneron)
- The Science: A classic monoclonal antibody neutralizing GDF-8.
- The Strategy: Regeneron is testing this alone and in a “triplet” with Garetosmab (anti-Activin A). The hypothesis is that blocking Myostatin alone preserves some muscle, but blocking both Myostatin and Activin A is required for maximal muscle retention during rapid weight loss.
- Status: The Phase 2 COURAGE trial data (Sept 2025) validated the “muscle preservation” thesis, showing distinct advantages over Semaglutide monotherapy.
4. Taldefgrobep Alfa (Biohaven)
- The Science: This molecule uses a different modality (Adnectin) to bind myostatin.
- Current Reality: The failure of the RESILIENT trial (Aug 2025) is a major blow. It failed to significantly improve motor function scores (MFM-32) over placebo in SMA patients. This reinforces the difficulty of translating myostatin inhibition into functional motor gains in neurodegenerative disease, as opposed to simple hypertrophy in metabolic contexts.
Discontinued / Historical Failures
- Domagrozumab (Pfizer): Discontinued (failed in DMD).
- Landogrozumab (Eli Lilly): Discontinued (failed in sarcopenia/hip fracture).
- ACE-083 (Acceleron): Discontinued (local injection proved ineffective).
Knowledge Gap & Next Steps
The critical debate in 2026 is no longer “Can we inhibit myostatin?” but “Does inhibiting myostatin improve function or just aesthetics/mass?” The SMA trials suggest mass function in diseased muscle. However, the obesity trials suggest mass = metabolic health in otherwise healthy adults.
Delivery Mechanisms / Routes:
None of the drugs currently leading the clinical race for myostatin inhibition are oral small molecules. They are all biologics (large protein molecules) requiring injection.
Because myostatin and its receptors are complex protein structures, blocking them typically requires a monoclonal antibody (mAb) or a large fusion protein, which would be destroyed by the stomach if swallowed.
Here is the breakdown of the delivery methods for the specific assets mentioned in my previous response.
1. Subcutaneous Injection (The “At-Home” Standard)
Most companies are aggressively pivoting to subcutaneous (fat tissue) injection pens to match the convenience of drugs like Ozempic/Wegovy.
| Drug | Delivery Method | Frequency (Est.) | Notes |
|---|---|---|---|
| Trevogrumab (Regeneron) | Subcutaneous (SC) | Weekly | Designed to be co-formulated or co-administered with Semaglutide (also weekly). |
| Taldefgrobep Alfa (Biohaven) | Subcutaneous (SC) | Weekly | Being developed as a self-administered pen for the obesity market. |
| GYM329 (Roche) | Subcutaneous (SC) | Monthly (Every 4 weeks) | The long half-life allows for less frequent dosing than the weekly GLP-1s. |
| Bimagrumab (Lilly) | Subcutaneous (SC) | Monthly | Note: Originally developed as an IV infusion (intravenous), Lilly/Versanis transitioned it to a subcutaneous formulation to make it viable for the mass obesity market. |
2. Intravenous Infusion (Medical/Clinic Use)
These are generally less desirable for biohacking or longevity purposes due to the need for a clinical setting, though formulations often evolve toward SC over time.
| Drug | Delivery Method | Frequency | Notes |
|---|---|---|---|
| Apitegromab (Scholar Rock) | IV Infusion | Every 4 weeks | Currently requires a ~1-hour infusion. Scholar Rock has discussed potential SC formulations, but the current Phase 3 data is based on IV delivery. |
Are there any Oral Myostatin Blockers?
Currently, no.
Developing an oral small molecule that can selectively block the myostatin receptor (ActRII) without causing off-target toxicity (like heart valve issues or bleeding) has proven extremely difficult.
- The “Oral” Alternative (BioAge): While not a myostatin blocker, Azelaprag (BGE-105) by BioAge is an oral small molecule (apelin receptor agonist) currently in Phase 2 trials. It mimics the “exercise signal” to prevent muscle atrophy during weight loss, but it works via a completely different pathway than myostatin.