I’ve been interested in Rapamycin for some time now and I’ve ordered some from India that’s bound to arrive soon.
However, I do have multiple sclerosis and after a quick search about MS/remyelination and Rapamycin, I’m finding contrasting results: some studies showed that remyelination is inhibited by Rapamycin, others (honestly less “reputable”) imply there might be some benefit. Another mTOR inhibitor, Metformin, is a promising remyelinating agent currently being tested both as standalone and coupled with Clemastine (and possibly Simvastatin).
So my question I guess is: anyone got direct experience or has more information about the role of mTOR/Rapamycin in MS?
The article highlights the central role of autophagy in MS progression. This is the same conclusion I came to and do extensive autophagy induction. I do fortnightly 100mg Dasatinib with Quercetin (and Fisetin for luck ).
I’m currently doing the DAV protocol and feel amazing!!!
I do weekly whole body cryotherapy which is also drastically reducing inflammation.
One thing I became aware of was that antioxidants don’t mix well with trying to induce autophagy. Trying to save those pesky senescent cells can lead to toxicity. Note the below:
For this reason I am a big user (every morning with my 100% cocoa powder) Treehelose:
Spermidine is also great and I get this with my ‘super cereal’ of Walnuts, seeds, nuts, probiotic yogurt, high polyphenol extra virgin olive oil (40ml), Chia seed oil (10ml), Wheat Germ Oil (10ml) [good source of spermidine and relatively cheap compared to “spermidine supplements”, goji berries.
Taurine is also VERY good for MS and I get this in my protein shake with Glycine (10 grams of each).
Oh I forgot to mention (but this goes without saying) I take 6mg rapamycin every Monday
***standard small print - nothing I post in this forum or elsewhere is intended to be taken as medical advice. I am not a trained medical practitioner!!!
It seems that the two protocols you refer to above are about clearing senescence more than they are about general autophagy - how do you think about those two concepts while overlapping in someways not being the same thing? Seems that was is needed for MS is more the autophagy part?
Good point. True, I suppose not all dysfunctional cells are senescent. My protocols seems to target the latter (senescent cells) as a subset of the former (dysfunctional cells), whereas autophagy (targeting any dysfunctional cell) is the larger concept (which includes senescence clearance, given that a senescent cell is dysfunctional). Have I understood that correctly?
I need to look into autophagy proper, I have just been going with D&Q, Fisetin, Treehelose and Spermidine as doing both, but you’re right - I’m not sure that it clears dysfunctional cells that are not senescent.
Think that may be directionally correct, but I’m not that well read up on this.
(May be more corner cases, but fwiiw, also think there may also be cases of senescent/zombie cells that “normal” autophagy may fail to clear but that senolytic therapy can clear)
Beginning from day 7 post immunization (d.p.i.), animals received an i.p. injection of saline, DM 0.1 mg/kg (DM-0.1) or DM 10 mg/kg (DM-10) (Sigma) once daily.
Overall, our results reveal a novel protective effect of low dose DM dextrometorphan) in autoimmune CNS inflammation, and demonstrate that a possible mechanism of action is via inhibition of NADPH oxidase and decrease of CNS leukocytes infiltration. These exciting findings may provide useful information leading to a new, inexpensive strategy for treating MS.
.1 divided by 12.3 times 70 (70 kilo human) is about a half mg a day. The adult dose for cough is 20 mg four times daily. So that is one fortieth of the cough dose, taken once a day. Cough dose is taken four times a day. Dextrometorphan plain (no expectorant like guaifenesin) is available over the counter (CVS, Walgreens). The dose may need to be increased, to match the DM in the mice’s system, after injection. But even at 2 mg per day, Dextrometorphan still has effects on NADPH oxidase, which seems to be the mechanism of action.
There is also a DM formulation with low dose quinidine.
Avanir Pharmaceuticals has been conducting trials of AVP-923 in its current and related formulations for several years as a treatment for pseudobulbar affect in a number of disorders, including MS, ALS, Alzheimer’s disease and stroke. AVP-923 is a patented, orally-administered combination of dextromethorphan and an enzyme inhibitor known as quinidine; quinidine is a drug that inhibits the metabolism of dextromethorphan which results in a sustained elevation of dextromethorphan in the brain.
Cheap, generic medicine for allergy helps repair in MS in one trial, other trial stopped
To our knowledge, this is the first randomised controlled trial to document efficacy of a remyelinating drug for the treatment of chronic demyelinating injury in multiple sclerosis. Our findings suggest that myelin repair can be achieved even following prolonged damage.
Clemastine fumarate treatment was associated with fatigue, but no serious adverse events were reported.
in patients with relapsing multiple sclerosis with chronic demyelinating optic neuropathy on stable immunomodulatory therapy. Patients who fulfilled international panel criteria for diagnosis with disease duration of less than 15 years were eligible.
receive either clemastine fumarate (5·36 mg orally twice daily) for 90 days followed by placebo for 60 days (group 1), or placebo for 90 days followed by clemastine fumarate (5·36 mg orally twice daily) for*** 60 days (group 2)***.
Yeah, muscarinic antagonists (clemastine has some off target muscarinic antagonism) have been shown to increase remyelination in vitro. The fact that the progressive patients saw a worsening might be due to clemastine’s other cholinergic off target effects (from memory only the M3 appears important in remyelination, but clemastine also affects M1 & M2) and progressive patients tend to have less cognitive reserve to compensate for cholinergic effects.
Interesting that above dextromethorphan was mentioned. It’s a known NMDA receptor antagonist. Know what is prescribed off label for MS-associated fatigue? Amantadine, another NMDAr antagonist (though it’s also a dopaminergic agent. It works very well for fatigue, btw)
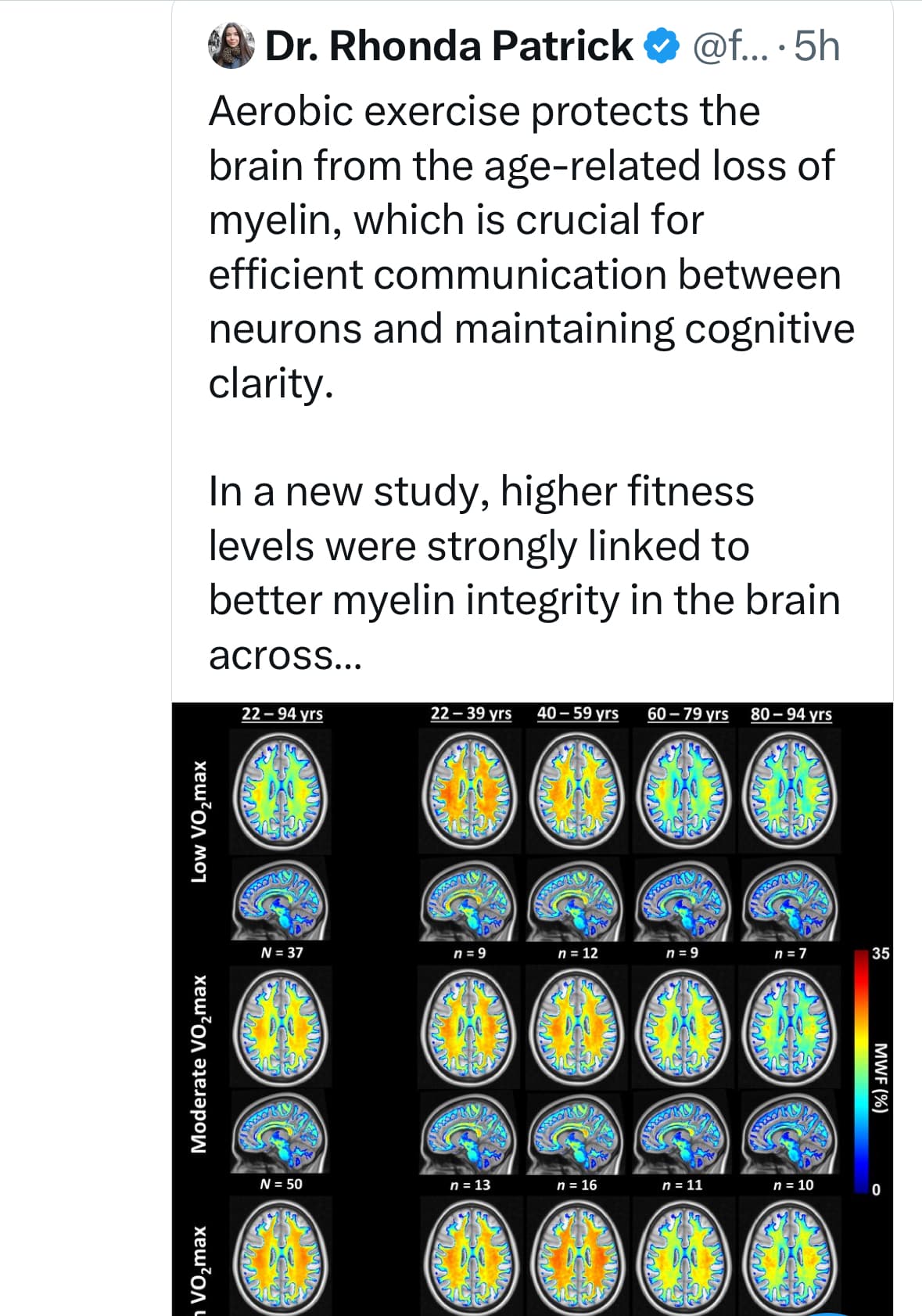
@A_User did you know it helps with myelin sheet growth - I don’t think most people were aware of that…
That is a massive issue in several big diseases like MS (and aging) - and while big biotech investments have gone into it no one has cracked it via any medicine or therapeutic yet
So for people on this specific thread this might be very interesting because of the specific focus of her tweet and the study , not because of that exercise is generally goo
I don’t think it does so it does not inform me on whether to exercise or not (and I think the same would be true for MS patients), lots of good reasons to exercise either way.